
Abstract
Tornwaldt cyst is a relatively rare lesion that is found in the posterior wall of the nasopharynx. It occurs in the midline bursa of the nasopharynx and represents a persistent communication between the roof of the nasopharynx and the notochordal remnants. Smaller cysts are usually asymptomatic; cysts exceeding a diameter of 1 to 2 cm may be symptomatic. Magnetic resonance imaging is the best imaging modality for diagnosing Tornwaldt cyst. We present a rare case of a huge Tornwaldt cyst completely obstructing the nasopharyngeal airway.
A 62-year-old man was referred to the Department of Otolaryngology of our university’s hospital for the evaluation of a nasopharyngeal mass. He complained of a 9-month-old history of nasal obstruction, snoring, headache, ear fullness, and left-sided hearing loss that had progressed rapidly over a 3-week period. Nasal endoscopy revealed a yellowish cystic mass, with smooth margins, in the nasopharynx, completely obstructing its lumen (Figure 1), and polyps in both middle meati. Otoscopy revealed an amber-colored, left tympanic membrane, and pure tone audiometry demonstrated left hearing loss, with an air–bone gap of 27 dB.
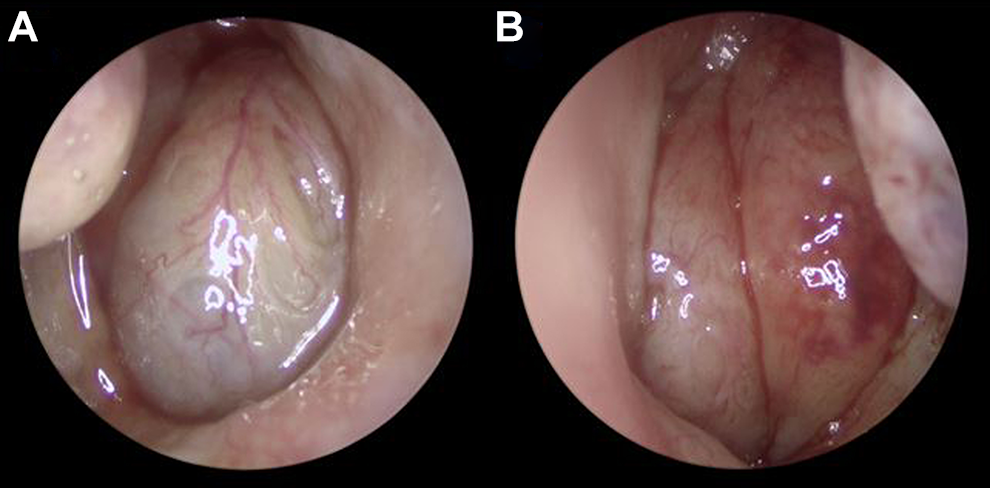
Nasal endoscopy showing a yellowish cystic mass with smooth margins in the nasopharynx, completely obstructing its lumen (A: right, B: left).
A computed tomography scan of the sinus was performed, which revealed lesions with soft tissue densities occupying the frontal, ethmoid, and maxillary sinuses, bilaterally. Magnetic resonance imaging was recommended for the evaluation of the nasopharyngeal mass, which revealed a 4 × 3 × 2 cm cystic mass in the nasopharynx. The mass was hyperintense on T1- and T2-weighted images, with mild thin wall enhancement, and completely obstructed the nasopharyngeal airway (Figure 2). A diagnosis of Tornwaldt cyst (TC) was made. Endoscopic sinus surgery was performed under general anesthesia. First, middle meatal antrostomy, ethmoidectomy, and frontal sinusotomy were performed. Subsequently, marsupialization of the cyst was performed with a microdebrider, using the endonasal endoscopic approach. The cyst was composed of a considerably thick wall, filled with a thick gelatinous discharge. The wall of the cyst was partially excised for pathological examination. The nasopharynx regained its wide patency after marsupialization. Pathological examination revealed a respiratory lined epithelial cyst, compatible with a TC (Figure 3). The postoperative period was uneventful, and the patient remained symptom-free. The preoperative air–bone gap was not visible on pure tone audiometry, 3 weeks after surgery. There was no recurrence during the postoperative follow-up.
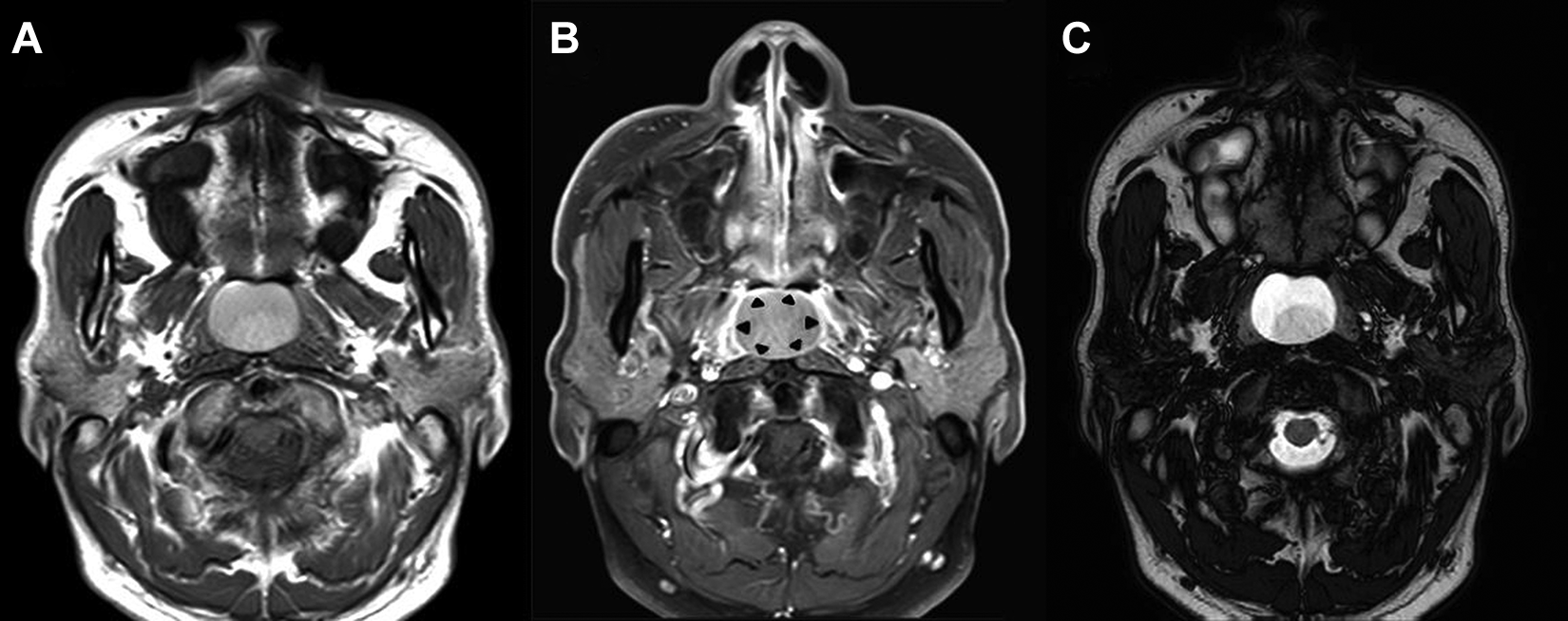
T1-weighted axial (A), T1-contrast enhanced axial (B), and T2-weighted axial (C) images showing a hyperintense cystic mass, measuring 4 × 3 × 2 cm, with complete obstruction of the nasopharyngeal airway. Contrast-enhanced fat suppression T1 image shows mild thin wall enhancement of the cystic mass (arrowheads).
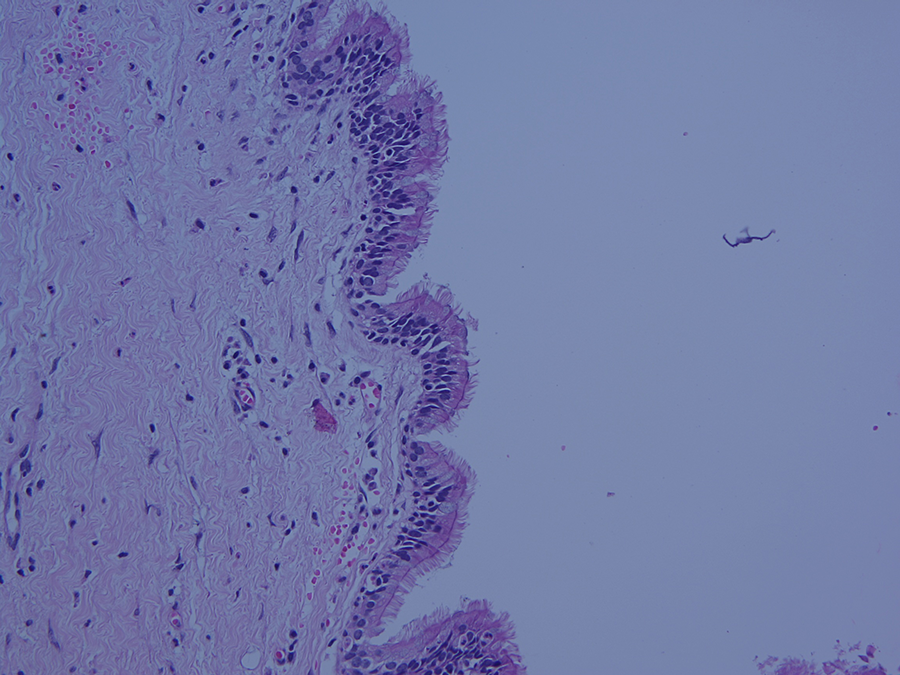
Pathological examination reveals a respiratory lined epithelial cyst, compatible with a Tornwaldt cyst (H&E stain, ×200).
Tornwaldt cyst is a relatively rare lesion that is found in the posterior wall of the nasopharynx. It has an incidence of 1.4% to 3.3% in the adult population. 1 It occurs in the midline bursa of the nasopharynx and represents a persistent communication between the roof of the nasopharynx and the notochordal remants. 2 Smaller cysts are usually asymptomatic; cysts exceeding a diameter of 1 to 2 cm may be symptomatic. The 3 most common symptoms are postnasal discharge, occipital headache, and halitosis. 3 Ear fullness and hearing loss may be caused by dysfunction of the eustachian tube, resulting in serous otitis media, secondary to inflammation or compression.
Nasal endoscopy plays a key role in the diagnosis of TC, depicting the well-encapsulated lesion located in the nasopharynx. Magnetic resonance imaging is the best imaging modality for diagnosing TC. The lesion usually has a characteristic high-signal intensity on T1- and T2-weighted images, due to its high protein content or association with hemorrhage within the cyst. 1 The diagnosis of nasopharyngeal cysts requires differentiation from other cysts. 4 The most common differential diagnoses include branchial cleft cyst, Rathke pouch cyst, and adenoidal retention cyst. Branchial cleft cysts are usually found at the lateral aspect of the nasopharyngeal space, but TC, Rathke pouch, and adenoid retention cysts are found near the midline. Tornwaldt cyst, Rathke pouch, and adenoid retention cysts have characteristic pathologic findings, respectively. Symptomatic cases can be treated via the endonasal or transoral approach. We performed endonasal endoscopic marsupialization of the cyst using microdebrider in this case. Endonasal endoscopic marsupialization provides an excellent field of vision for surgery and so the surgeons can avoid damaging the orifice of the eustachian tube. Endonasal endoscopic marsupialization is the preferred treatment for large TCs. Long-term (5 years) follow-up showed that endonasal endoscopic marsupialization of TC using microdebrider is a safe and effective procedure with no recurrence, eustachian tube damage, or postoperative complications. 5 We present a rare case of a huge TC completely obstructing the nasopharyngeal airway.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by Wonkwang University in 2020.