
Abstract
Introduction
Deep neck infections (DNIs) are severe bacterial infections of the fascial planes and deep neck spaces that are typically affected by the upper aerodigestive tract. 1 -5 Treatment involves securing the airway, prompt surgical incision and drainage (I&D), and the provision of antibiotics. 2,6 Without proper management, DNI can lead to severe complications. 6,7
Population aging is occurring worldwide. For patients presenting with neck masses or swelling, DNI should be included in the differential diagnosis regardless of age. 8 Patients aged >65 years are classified as elderly. 9,10 Immunosenescence is a type of immune system dysregulation that increases susceptibility to bacterial infection in elderly patients. 11 Neutrophil function declines with age, reflected in a loss of phagocytosis and bactericidal ability. 9 However, according to the literature, the incidence of DNI mostly occurs in middle-aged adults. 12 -14
Treating DNI can be difficult in elderly patients because of the decline in immune function and high rates of comorbidities in this group. 10 Thus, a multidisciplinary treatment team is essential for elderly DNI patients. 15
However, few studies have specifically addressed DNI in elderly patients. Therefore, this study assessed the clinical characteristics, outcomes, and prognosis of elderly DNI patients.
Materials and Methods
We retrospectively reviewed the medical records of 398 patients diagnosed with DNI, including 113 elderly DNI patients, who presented to Linkou Chang Gung Memorial Hospital (a tertiary medical center in Taiwan) between November 2016 and November 2022. The patients were diagnosed based on their clinical presentations and computed tomography (CT) findings. 7,16,17 Contrast-enhanced CT, which is part of the routine investigations conducted at our hospital, is essential for identifying cellulitis and abscess formation. 18
For the management of DNI, patients are provided with airway support, broad-spectrum antibiotics, and I&D in accordance with clinical and radiological findings. 19 Airway management includes intubation and tracheostomy. 20 Pathogen cultures are typically collected via an aseptic procedure, and empirical antibiotics are routinely administered before the final culture results are available. 21 At our hospital, ceftriaxone (1 g q12h) and metronidazole (500 mg q8h) are used as empirical antibiotics for aerobic and anaerobic bacteria. 14,22,23 All of the patients in this study were adequately hydrated. Postoperatively, oral hygiene was maintained, and wound irrigation was performed as necessary. The elderly and adult patients were aged >65 and 18 to 65 years, respectively.
Exclusion Criteria
Patients with superficial infection, previous head and neck surgery, 24 a history of head and neck malignancy, 25 previous radiotherapy to the head and neck region, peritonsillar abscess, a history of traumatic neck injury, severe cardiopulmonary disease, or DNI secondary to swallowing of a foreign body were excluded. Furthermore, this study excluded patients performing surgical procedures under local anesthesia.
Data Collection
We collected data on gender; age; chief complaint and hospital stay durations; C-reactive protein (CRP) and blood sugar levels; the number of deep neck spaces involved [one, double, or 3 or more (multiple)]; deep neck space involvement (parapharyngeal, submandibular, retropharyngeal, masticator, parotid, anterior cervical, carotid, visceral, perivertebral, or posterior cervical space); diabetes mellitus (DM), mediastinitis, intubation, tracheostomy, and I&D status; and causative pathogens.
Statistical Analysis
All statistical analyses were performed using MedCalc software (version 18.6; MedCalc, Ostend, Belgium). Because the Kolmogorov–Smirnov test showed that the data were not normally distributed, the chi-square and Mann–Whitney U tests were used to analyze categorical and continuous variables, respectively. In addition, the multivariate forward stepwise selection procedure was applied for the relevant risk factors. P-values < .05 were considered statistically significant.
Results
Table 1 presents the clinical characteristics of the 398 DNIs enrolled in this study [252 (63.32%) men and 146 (36.68%) women; mean age = 53.88 ± 17.72 years]. The mean chief complaint duration was 4.64 ± 4.21 days, and the mean hospital stay was 10.44 ± 8.19 days. The mean CRP level was 159.45 ± 107.89 mg/L, the mean blood sugar level was 145.93 ± 70.85 mg/dL, and 175 (43.96%) patients had DM.
Clinical Characteristics of the 398 Deep Neck Infection Patients Enrolled in this Study.
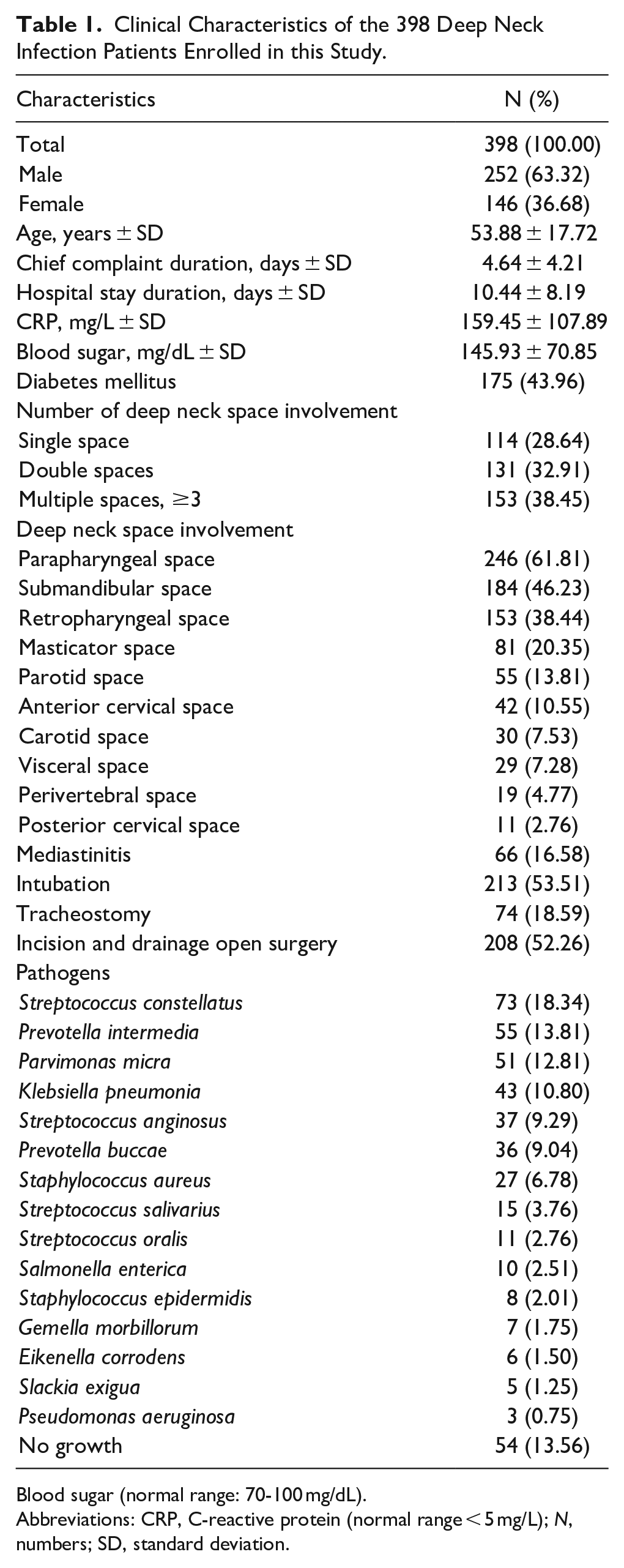
Blood sugar (normal range: 70-100 mg/dL).
Abbreviations: CRP, C-reactive protein (normal range < 5 mg/L); N, numbers; SD, standard deviation.
In total, 114 (28.64%), 131 (32.91%), and 153 (38.45%) patients exhibited involvement of one, double, and multiple deep neck spaces, respectively. There were 246 (61.81%), 184 (46.23%), 153 (38.44%), 81 (20.35%), 55 (13.81%), 42 (10.55%), 30 (7.53%), 29 (7.28%), 19 (4.77%), and 11 (2.76%) patients with parapharyngeal, submandibular, retropharyngeal, masticator, parotid, anterior cervical, carotid, visceral, perivertebral, and posterior cervical space involvement, respectively.
Mediastinitis was present in 66 (16.58%) patients. For airway management, intubation was used in 213 (53.51%) patients, and tracheostomy was performed in 74 (18.59%) patients. Finally, I&D was performed in 208 (52.26%) patients.
Streptococcus constellatus, Prevotella intermedia, Parvimonas micra, Klebsiella pneumonia, Streptococcus anginosus, Prevotella buccae, Staphylococcus aureus, Streptococcus salivarius, Streptococcus oralis, Salmonella enterica, Staphylococcus epidermidis, Gemella morbillorum, Eikenella corrodens, Slackia exigua, Pseudomonas aeruginosa, and no specific pathogens were identified in 73 (18.34%), 55 (13.81%), 51 (12.81%), 43 (10.80%), 37 (9.29%), 36 (9.04%), 27 (6.78%), 15 (3.76%), 11 (2.76%), 10 (2.51%), 8 (2.01%), 7 (1.75%), 6 (1.50%), 5 (1.25%), 3 (0.75%), and 54 (13.56%) patients, respectively (Table 1).
Table 2 shows the comparison of clinical characteristics between elderly and adult patients. The elderly patients had longer hospital stays (P < .001), higher CRP and blood sugar levels (P = .021 and P = .012, respectively), and higher rates of DM (P = .025), intubation (P = .005), and I&D (P = .010) than the adult patients. After the multivariate analysis, higher blood sugar level is an independent risk factor for elderly [odds ratio (OR) = 1.005, 95% confidence intervals (CI) 1.002-1.008, P < .001].
Clinical Characteristics and Analysis of the Elderly and Adult Deep Neck Infection Groups.
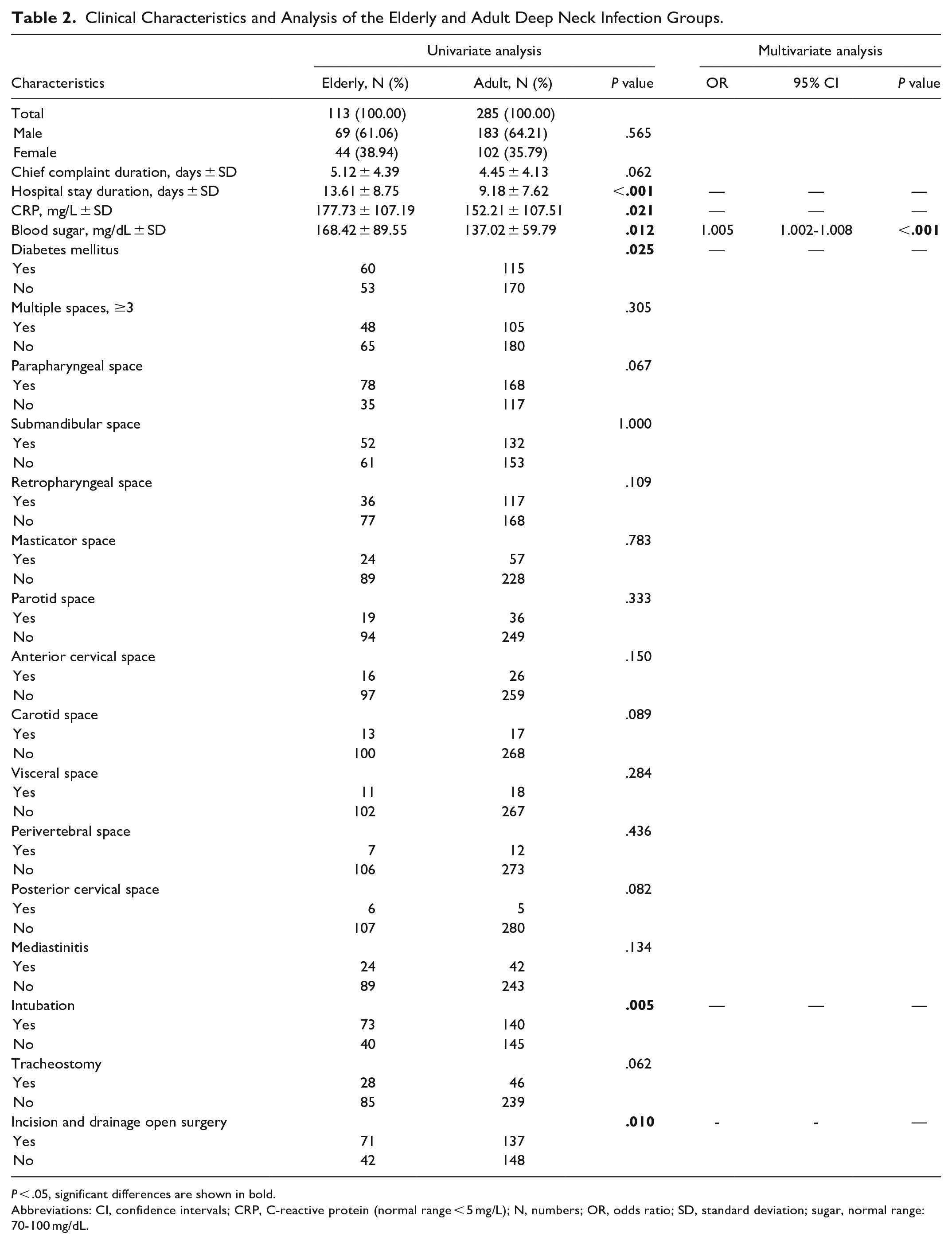
P < .05, significant differences are shown in bold.
Abbreviations: CI, confidence intervals; CRP, C-reactive protein (normal range < 5 mg/L); N, numbers; OR, odds ratio; SD, standard deviation; sugar, normal range: 70-100 mg/dL.
Table 3 displays the comparison of pathogens between elderly and adult patients. The pathogen distributions did not show a significant difference between the elderly and adult patients, 11 (9.73%) and 43 (15.08%) of whom had no specific pathogens, respectively.
Pathogen Distributions of the Elderly and Adult Deep Neck Infection Groups.
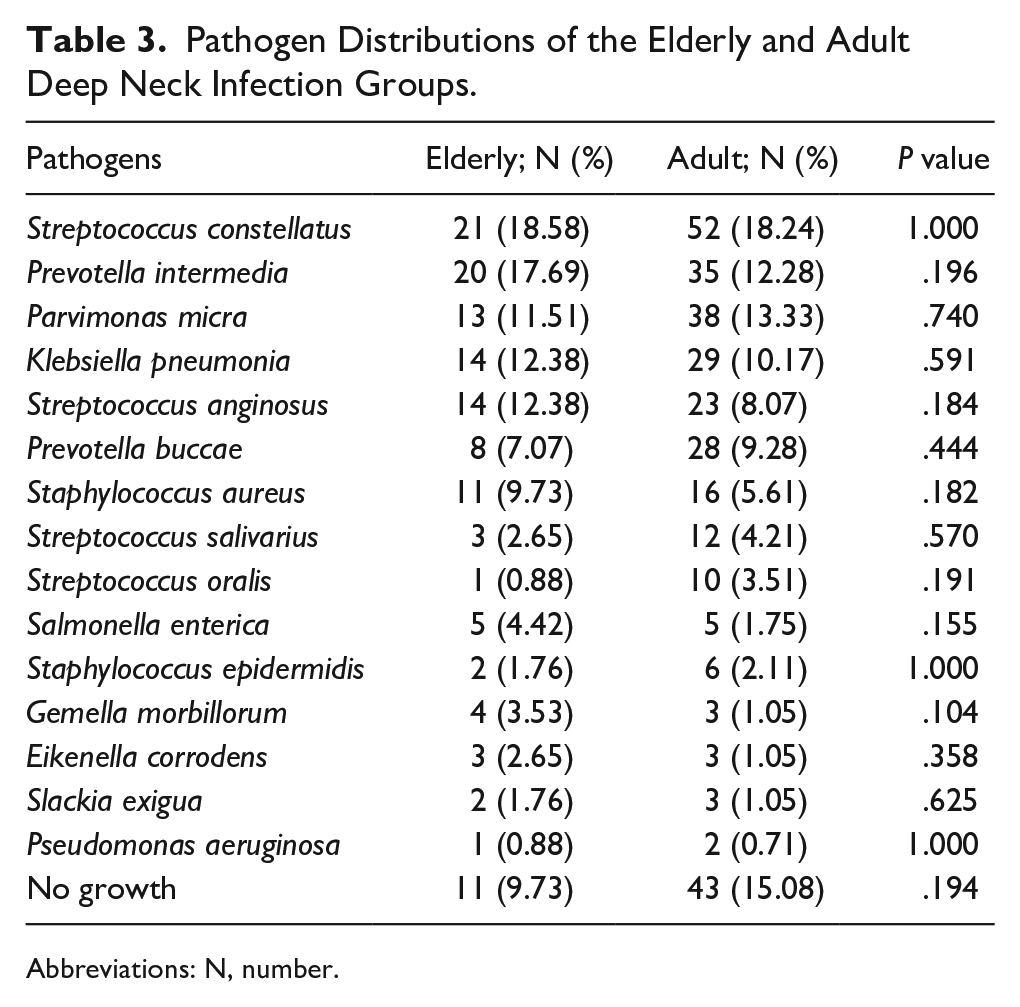
Abbreviations: N, number.
Discussion
Due to the gradual aging of the general population, the number of elderly DNI patients is increasing worldwide. Moreover, many immune changes associated with aging increase the severity of DNI. 10 Airway security, surgical drainage, and adequate antibiotic treatment are important for DNI management, regardless of age. 26,27 The mortality rate of DNI has decreased because of advances in diagnostic techniques, greater access to antibiotics, and the use of surgical procedures. 28,29 Nevertheless, due to the rapid onset and fast progression of DNI, delayed management can lead to lethal complications. 9,15,21,22,30 -44 Thus, appropriate management is crucial for DNI patients.
Immunocompromised patients are more vulnerable to infections. 45 Immunosenescence is defined as an age-related decline in immunologic function that can increase susceptibility to bacterial infections, autoimmune diseases, and even malignant tumors. 46 Thus, immunosenescence (along with DM and hemodialysis) is associated with a more severe disease course in elderly DNI patients. 47 The elderly DNI patients in this study tended to have a more severe disease course and poorer prognosis than the adult patients, as well as higher rates of intubation and I&D. However, the pathogen distributions showed no significant group differences.
As shown in Table 1, the mean age of our entire cohort was 53.88 ± 17.72 years; this accords with previous studies demonstrating that DNI typically occurs in middle-aged adults. 48,49 As shown in Table 2, our elderly DNI patients had significantly longer hospital stays than the adult patients, consistent with a study in which the mean hospital stays of elderly and adult DNI groups were 11.1 and 8.2 days, respectively. 10 One plausible reason for this difference is that the rates of multiple neck space involvement and complications are higher in elderly populations. In another study, age was positively correlated with the hospital stay duration of DNI patients. 1
The elderly DNI patients in this study had higher CRP levels than the adult patients. In a previous study of DNI patients, an elevated preoperative CRP level was a significant risk factor for persistent discharge after surgical drainage. 50 CRP also correlated with the period of hospital stay. 51 Furthermore, CRP levels were higher in DNI patients who underwent surgical drainage; the CRP cut-off value for surgical drainage was 133 mg/L. 52 In addition, an elevated CRP level is the main indicator of odontogenic infection in DNI. 41,53 However, Brajkovic et al 54,55 considered CRP is not a sensitive predictor for DNI outcome.
DM is a major public health issue worldwide. 56 The incidence of DM is particularly high among the elderly population of the United States, at approximately 30%. 57 Furthermore, DM is a risk factor for DNI 58 ; in fact, it reportedly shows the strongest association with DNI among several common systemic illnesses. 39 The incidence rates of DM and cardiac illness are high in elderly populations. 9 The incidence rate of DM in our elderly DNI group was 53.09% (n = 60/113), significantly higher than in the adult group (40.35%; n = 115/285).
Our elderly patients had high blood sugar levels, and we found higher blood sugar level is an independent risk factor for elderly. Patients with DM are usually accompanied by high blood sugar levels, and the previous study found that DM patients had low lymphocyte counts, which may explain the impaired immune function and high risk of infection seen among patients with poorly controlled DM. 9 This would cause difficulties in infection control. If infection control is difficult, I&D will be needed to treat the patient. This may be the reason for the higher proportion of I&D in elderly patients in this study.
Furthermore, DNI patients with high preoperative blood sugar may experience persistent discharge after surgery. 50 Previous research also found that a high blood sugar level is associated with repeated I&D in DNI. 12 Prompt blood sugar control can decrease the likelihood of infectious complications in DNI. 59,60 Finally, in addition to DM status and blood sugar level, education level and geographic location predict DNI severity. 61
Imaging studies are important to locate the site of DNI, determine its severity, and monitor disease progression. 62 Infection of the mediastinum could be promoted by negative intrathoracic pressure during respiration. 63,64 To avoid acute hypoxia and cardiac arrest, airway management is essential for DNI patients, 65 although one study reported that patients with airway management typically showed no symptoms of dyspnea. 66 In Table 2, we found that the proportion of intubation in elderly patients is higher than in adult patients, but there is no significant difference between the 2 groups for the site of deep neck abscesses. We consider the possible reason is that clinicians will be more cautious in protecting the airway of elderly patients. Intubation is a clinical decision made by the physician based on the patient’s respiratory status. When an elderly patient had dyspnea or a decreased blood oxygen saturation, the clinician will be more active in protecting the airway. Our elderly DNI group also had a significantly higher proportion of I&D than the adult group. The elderly DNI group in a previous study had a higher rate of surgical intervention than the adult DNI group (75.0% vs 38.8%). 10 Complete I&D of all deep space abscesses is essential to prevent reoperation and enhance survival. 67 Although needle aspiration can be performed in some DNI patients, draining a large number of abscesses is not recommended. 68,69
In our hospital, some DNI patients with airway compromise would be intubated to protect the airway, while I&D will be considered if the abscess is greater than 2 cm or antibiotics treatment is in vain. Thus, the rate of intubation is higher than that of I&D, and some cases were conservatively treated after the intubation.
In most cases, DNI has a dental origin, 70 -74 which is typically due to poor oral hygiene or delayed dental treatment. 10 Periapical infection of the second or third molars is particularly common; this is probably because the roots of these teeth extend downward toward the mandibular insertion of the mylohyoid muscle, which is near the parapharyngeal and submandibular spaces. 18 In another study, salivary gland infection was the second most common cause of DNI among elderly patients, which is concordant with the high prevalence of xerostomia seen in this age group. 10
DNIs can be caused by both aerobic and anaerobic polymicrobial organisms. 75 The pathogen distribution did not differ significantly between our elderly and adult DNI groups. Moreover, there were no specific pathogens in 11 (9.73%) and 43 (15.08%) of the elderly and adult patients, respectively. Prior to pus culture, empirical antibiotics tend to be provided, 76 which could explain the lack of specific pathogens seen in some DNI cases. 77 Although antibiotics decrease the risk of abscess formation, resistance to antibiotics has been growing. 78 -82 Finally, gas formation can facilitate the identification of anaerobic infection. 83
Study Limitations
This retrospective study was conducted at a single tertiary hospital. In this research, we did not compare the survival curve between the 2 groups to present the elderly patients’ poorer prognosis. Because pathogenic distributions may differ among hospitals according to the types of empirical antibiotics used, a multicenter study would have been preferable to improve the generalizability of the results.
Conclusion
The rates of intubation and I&D were higher in the elderly DNI group. Prompt intervention and treatment are particularly important for elderly patients with DNI. A higher blood sugar level is an independent risk factor for elderly. Although the elderly DNI patients had a more severe disease course and poorer prognosis than their adult counterparts, the pathogen distributions did not significantly differ between the groups in this study.
Footnotes
Acknowledgements
The authors thank all of the members of Department of Otorhinolaryngology—Head and Neck Surgery, Chang Gung Memorial Hospital, Linkou, for their invaluable help.
Authors’ Note
Author Contributions
Conceptualization: F-YH, C-YH, Y-CW, S-CC, and S-LC Methodology: F-YH, C-YH, K-CC, and S-LC. Validation: C-YH and S-LC. Data curation: S-LC. Writing—original draft preparation: F-YH and S-LC. Writing—review and editing: S-LC. Visualization: C-YH, K-CC, S-CC, and S-LC. Supervision: F-YH, Y-CW, and S-LC. Project administration: F-YH, C-YH, S-CC, and S-LC. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study was approved by the Institutional Review Board (IRB) of Chang Gung Medical Foundation (IRB number: 202300021B0). Data were collected retrospectively and anonymized before the analysis. The IRB waived the requirement for informed consent.