
Abstract
Introduction
Deep neck infection (DNI) encompasses several infections affecting spaces surrounding the neck1,2 and deep tissues, typically involving internal structures such as the pharynx, larynx, and trachea. It can lead to severe complications.3-11 The etiology of DNI commonly includes dental infections, tonsillar gland infections, and lymphadenitis. 12
Currently, contrast-enhanced computed tomography (CT) scan (Figures 1 and 2) is the main method for DNI. CT scan can accurately identify the edge of the abscess and adjacent tissues, which is helpful for abscess drainage. Basically, surgical drainage depends on the size and location of the abscess. Surgical drainage is required in patients with neurovascular complications, airway compromise, or failure to improve after at least 48 hours of intravenous antibiotics. Based on previous reports, use empiric antibiotics to cover aerobic and anaerobic bacteria until pathogen culture results are obtained, including ceftriaxone 1 g every 12 hours and metronidazole 500 mg every 8 hours.13-16
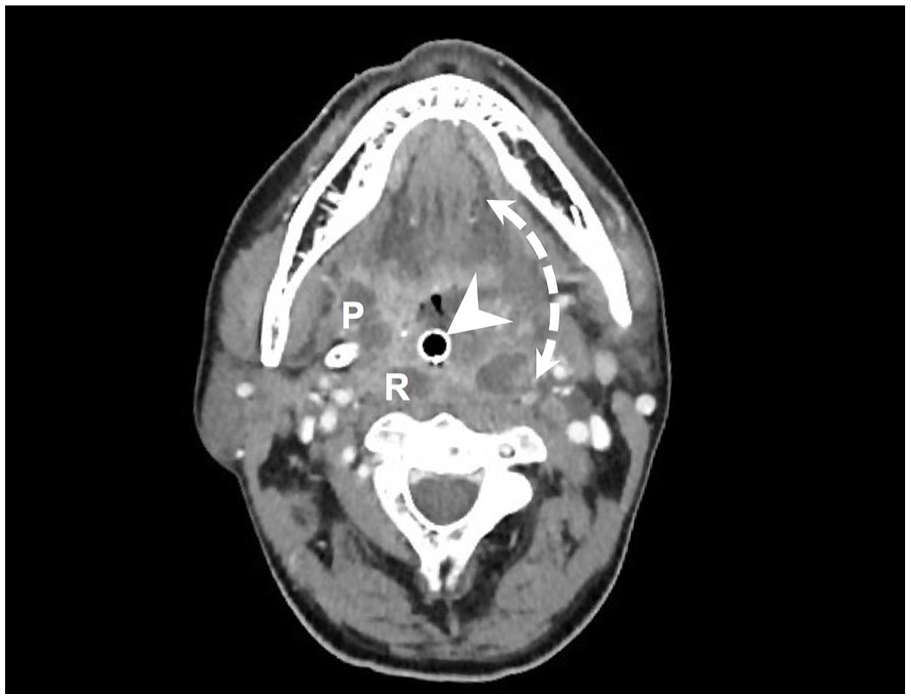
An axial computed tomography scan of the head and neck of a patient with DNI. The arrowhead points to the endotracheal tube. The area shown by the double-dot arrow represents the range of DNI. P, parapharyngeal space; R, retropharyngeal space.
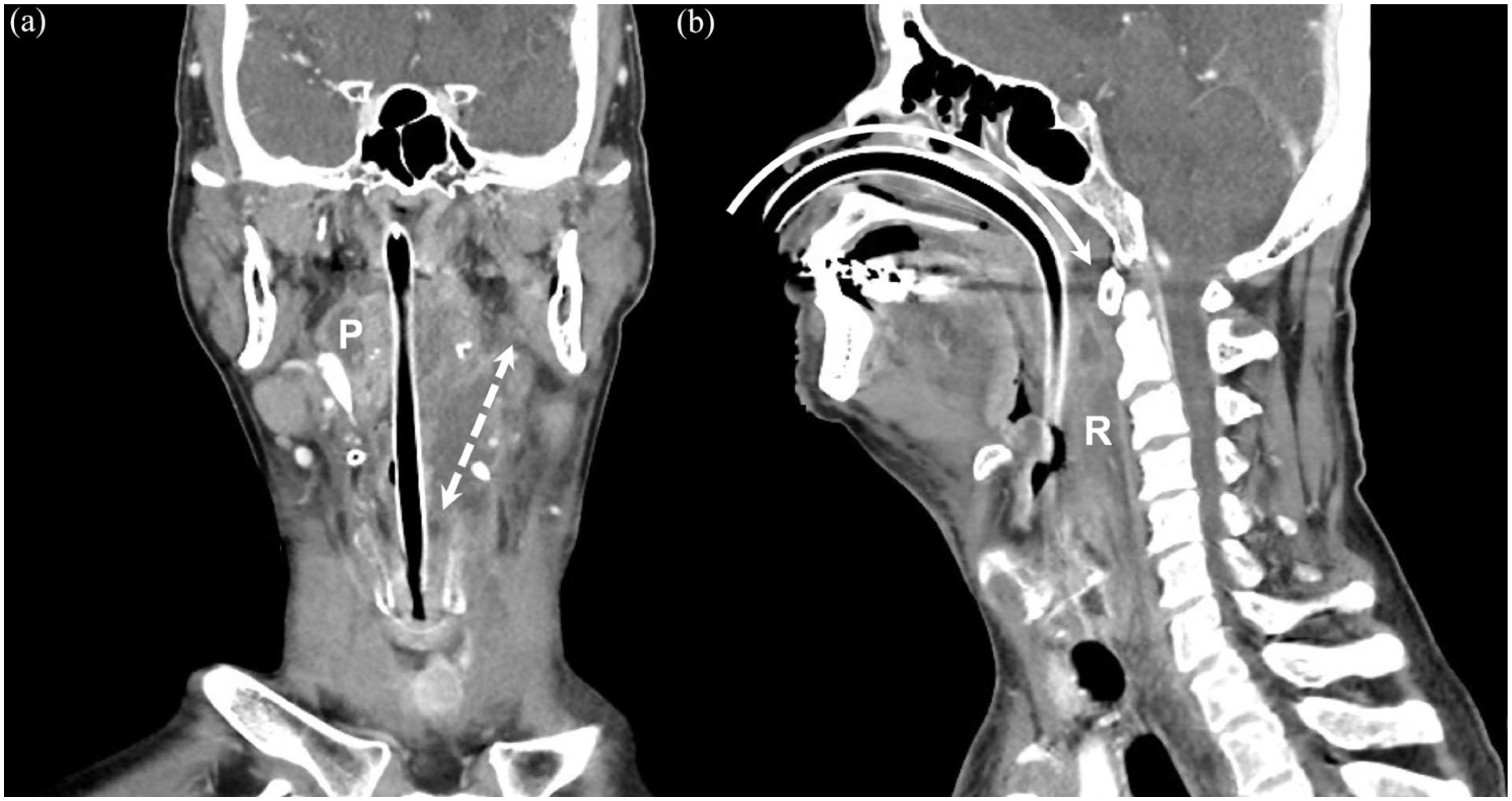
The coronal (A) and sagittal (B) computed tomography images of the head and neck of a patient with deep neck infection. Coronal view shows that the patient has obvious inflammation and abscess lesions in the parapharyngeal space, and the double dotted arrows indicate their expansion. For the sagittal view, the curved arrow represents the trajectory of the nasotracheal intubation. Because inflammation and swelling in the retropharyngeal and parapharyngeal spaces are too severe to open the patient’s mouth, the endotracheal tube is inserted through the nose rather than through the mouth. P, parapharyngeal space; R, retropharyngeal space.
Intensive care units (ICUs) of hospitals are designed for critically ill patients who require highly intensive medical care. To prevent interference and infection transmission, ICUs adopt a closed design and strictly limit visitor entry and meeting time. They are equipped with various equipment and instruments to continuously monitor vital signs and physiological changes in patients. Medical staff work in shifts to provide comprehensive care. 17 For patients with DNI, particularly those who are critically ill, admission to the ICU is necessary. In the ICU, continuous monitoring by medical staff working in 24 hours shifts facilitates the prompt detection and management of worsening DNI. Emergency tracheostomy and intubation is necessary to save the lives of patients with airway compromise. 18 In cases of rapid development of DNI, the opportunity to transfer these critically ill patients to the ICU may be missed. However, the factors associated with need for ICU admission in patients with DNI have not been investigated. Therefore, this study explored the predictors of ICU admission in this population.
Materials and Methods
A total of 350 patients aged >18 years who were diagnosed with DNI at Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan, between October 2018 and October 2023 were enrolled retrospectively. Clinical manifestations and diagnosis were recorded. The diagnosis of DNI was confirmed based on radiological imaging and laboratory and microbial testing. 19 A total of 62 patients with DNI were admitted to the ICU.
Patient data were collected to investigate risk factors for ICU transfer in patients with DNI (Table 1) including laboratory data such as C-reactive protein (CRP) level (at initial emergency admission; normal range <5 mg/L) and blood glucose level (at initial emergency admission; normal range: 70-100 mg/dL).
Clinical Characteristics of the 350 Patients With DNI.
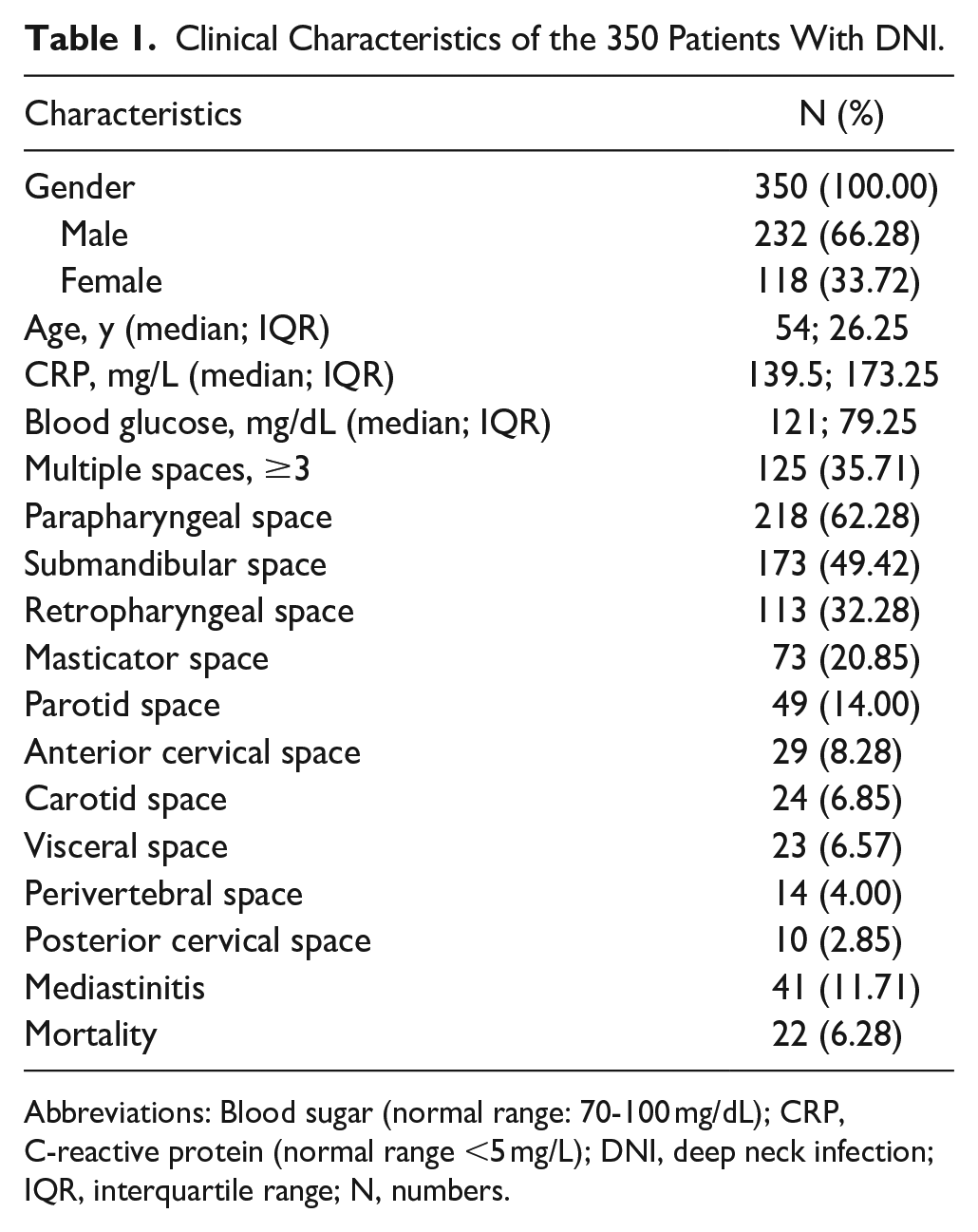
Abbreviations: Blood sugar (normal range: 70-100 mg/dL); CRP, C-reactive protein (normal range <5 mg/L); DNI, deep neck infection; IQR, interquartile range; N, numbers.
The attending physician decided whether to transfer the patient to the ICU based on clinical condition. Patients admitted to the ICU often had unstable vital signs or respiratory obstruction. The vital signs of patients were continuously monitored in the ICU, and emergency airway management was promptly initiated when indicated.
Patients are usually transferred to the ICU for treatment under 2 circumstances after initial treatment in the emergency room. One is that if symptoms worsen or airway obstruction occurs, the patient will be transferred to the ICU. Second, after the abscess is incised and drained, the patient still needs ICU care.
Exclusion Criteria
Patients who had previously undergone head and neck tumor surgery, head and neck radiotherapy, or swallowed foreign bodies were excluded.
Ethics Statement
Institutional Review Board (IRB) of the Chang Gung Memorial Medical Foundation approved this study (IRB number: 202301870B0) and waived the need for informed consent due to retrospective analysis.
Statistical Analysis
We used MedCalc software (version 18.6; MedCalc) to analyze all data. The chi-square test was used to analyze categorical variables, the Mann-Whitney U test was used to compare continuous variables, and logistic regression was used for univariate and multivariate analyses. The continuous variables were presented with median and IQR (interquartile range). P < .05 indicated statistical significance.
Results
This study included 350 patients with DNI, including 232 males (66.28%) and 118 females (33.72%) with a median age of 54 (IQR = 26.25) years old. Table 1 presents the clinical features of the study participants. The median CRP level was 139.5 (IQR = 173.25) mg/L, and the median blood glucose level was 121 (IQR = 79.25) mg/dL. Multiple spaces were involved in 125 (35.71%) patients. The most commonly involved spaces were the parapharyngeal space (n = 218, 62.28%), submandibular space (n = 173, 49.42%), and retropharyngeal space (n = 113, 32.28%). Mediastinitis developed in 41 (11.71%) patients. A total of 22 people died, and the mortality rate was around 6.28% (22/350).
Univariate analysis revealed that, compared to the non-ICU group, the ICU group had a significantly older age [62; 32.5 vs 52; 25 years; odds ratio (OR) = 1.0324, 95% confidence interval (CI): 1.0155-1.0496, P = .0001], higher CRP level (243.5; 149 vs 123; 145 mg/L; OR = 1.0076, 95% CI: 1.0049-1.0103, P < .0001), and blood glucose level (156; 127.25 vs 119; 57 mg/dL; OR = 1.0057, 95% CI: 1.0023-1.0091, P = .0011), and more frequent involvement of multiple spaces (OR = 2.2366, 95% CI: 1.2827-3.8998, P = .0046) and mediastinitis (OR = 4.7134, 95% CI: 2.3537-9.4391, P < .0001; Table 2).
Univariate and Multivariate Analyses of Patients Admitting to ICU.
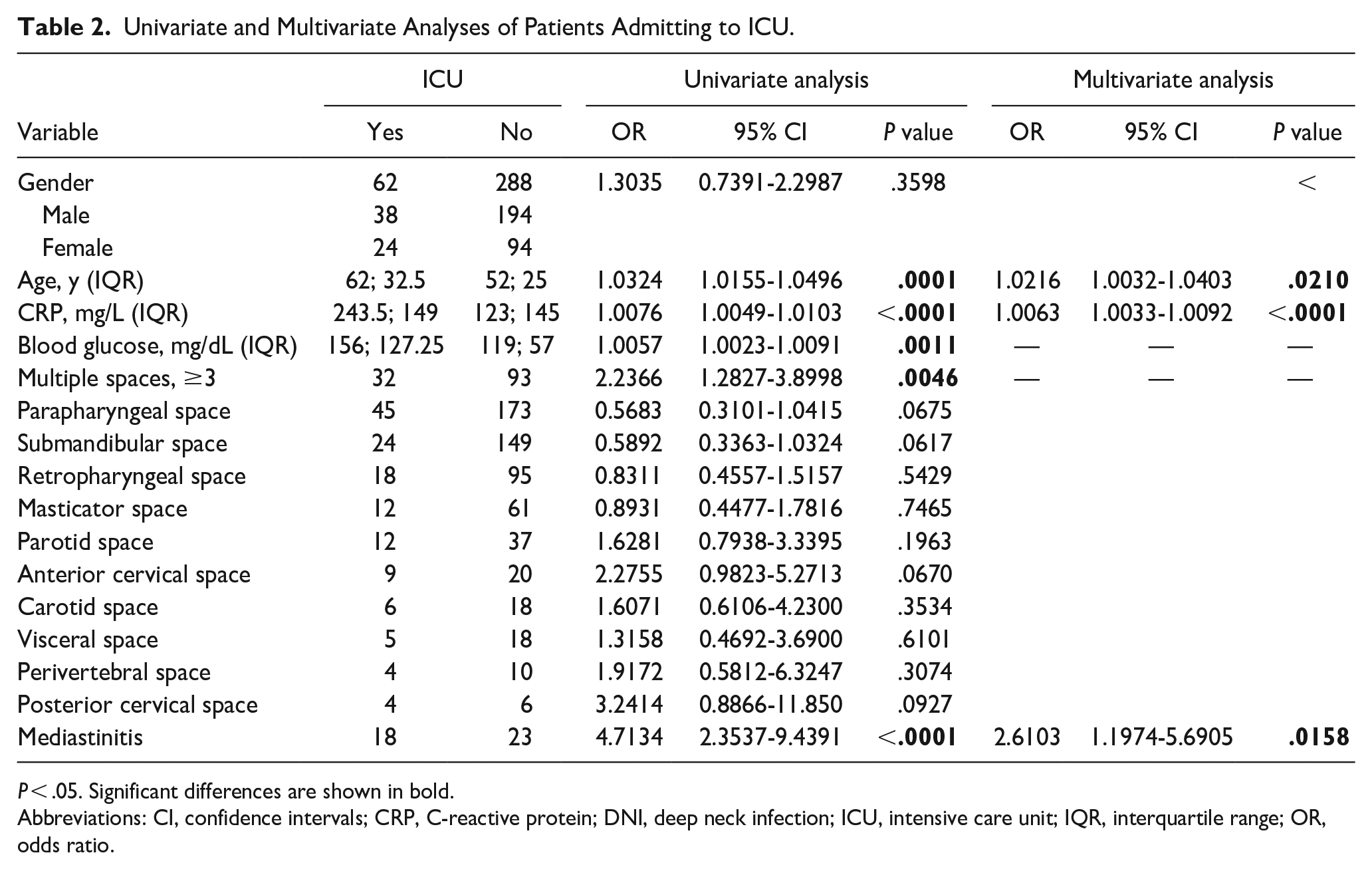
P < .05. Significant differences are shown in bold.
Abbreviations: CI, confidence intervals; CRP, C-reactive protein; DNI, deep neck infection; ICU, intensive care unit; IQR, interquartile range; OR, odds ratio.
Multivariate analysis revealed that patients with an older age (OR = 1.0216, 95% CI: 1.0032-1.0403, P = .0210), higher CRP level (OR = 1.0063, 95% CI: 1.0033-1.0092, P < .0001), and mediastinitis (OR = 2.6103, 95% CI: 1.1974-5.6905, P = .0158) were more likely to be admitted to the ICU.
Table 3 presents a comparison of the duration of hospital stay and management between patients with and without ICU admission. The median duration of hospital stay was significantly longer in the ICU group than in the non-ICU group (22; 12 vs 7; 6.75 days, P < .0001). The median length of ICU stay was 4 (IQR = 4) days. In addition, the proportion of patients requiring tracheostomy was significantly higher in the ICU group than in the non-ICU group (43.54% vs 9.72%, P < .0001). However, there were no significant differences in the proportion of patients undergoing open incision and drainage between the ICU and non-ICU groups (P = .2812). The mortality rate was also significantly higher in the ICU group than in the non-ICU group (12/62; 19.35% vs 10/288; 3.47%, P = .0001).
Comparison of Length of Hospital Stay and Management Between Patients With and Without Admitting to ICU.
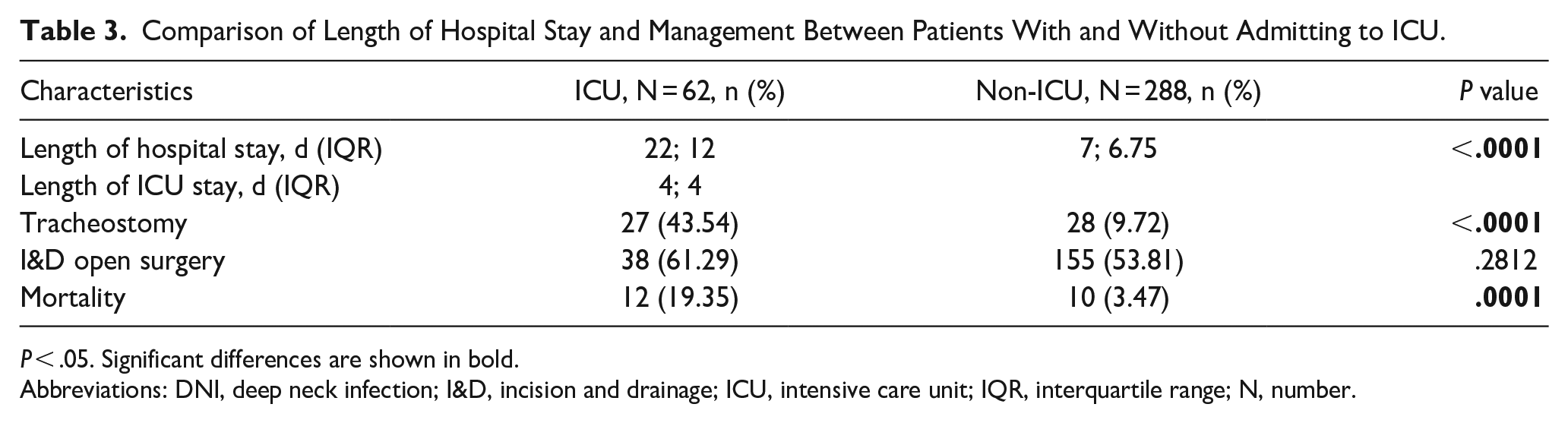
P < .05. Significant differences are shown in bold.
Abbreviations: DNI, deep neck infection; I&D, incision and drainage; ICU, intensive care unit; IQR, interquartile range; N, number.
Table 4 presents a comparison of pathogens between patients with and without ICU admission. For the patients admitted to the ICU, the most common pathogens were Streptococcus constellatus (24.19%), followed by Streptococcus anginosus (17.74%) and Klebsiella pneumonia (16.12%). In non-ICU patients, the most common pathogens were Parvimonas micra (15.97%), followed by S. constellatus (15.27%) and Prevotella intermedia (14.58%). However, there were no statistically different results between groups (P < .05).
Comparison of Pathogens Between Patients With and Without Admitting to ICU.
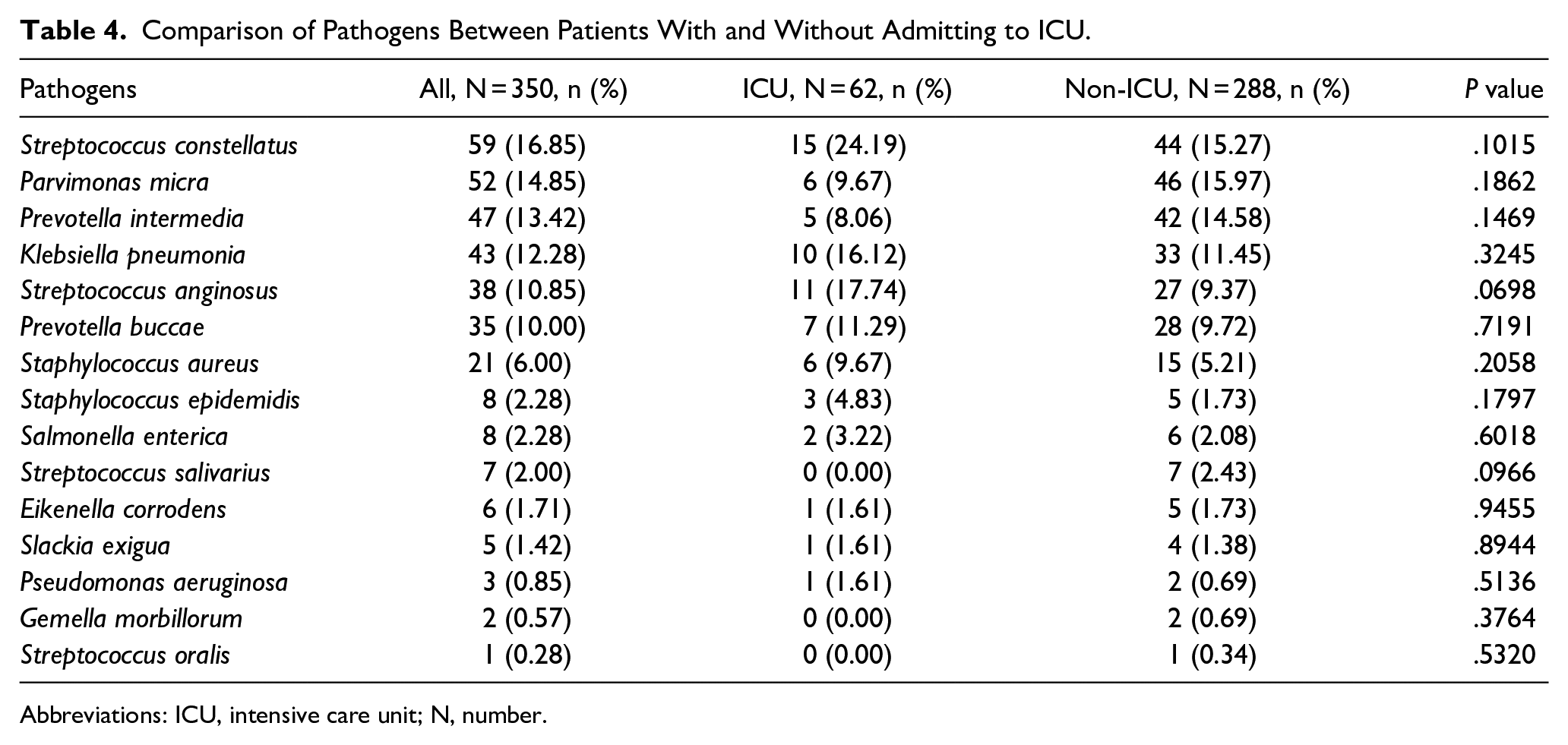
Abbreviations: ICU, intensive care unit; N, number.
Discussion
An ICU is a specialized medical facility designed for the treatment of critically ill patients, usually located within a highly specialized department of a hospital. In DNI, airway protection is essential for saving lives, particularly for individuals with severe respiratory or purulent infections. 20 Both endotracheal intubation and tracheostomy should be considered emergent procedures to stabilize the airway structure of patients.
Although patients are typically transferred to the ICU when symptoms worsen or airway obstruction develops, surgeons may make subjective decisions about whether patients require ICU transfer. In addition, the patient capacity of each ICU in each hospital also varies. These are the reasons why there are still no standards for patients to be transferred to ICU for treatment. This study attempts to identify risk factors for ICU transfer in patients with DNI. In this research, older age, a higher CRP level, and mediastinitis were independent risk factors for need of ICU transfer in patients with DNI. Patients requiring ICU admission had a longer hospital stay and a higher rate of tracheostomy than patients who did not require ICU admission. There were no differences in DNI pathogens between patients with and without ICU admission.
Univariate analysis revealed that a higher blood glucose level and involvement ≥3 spaces were risk factors for need of ICU transfer in DNI patients. A higher blood glucose level may be associated with a higher incidence rate and more severe complications of DNI.
Lin et al 21 revealed that patients with diabetes mellitus had a significantly higher complication rate, longer length of hospital stay, and more frequent need for tracheotomy than those without diabetes.
Similarly, Zheng et al 22 demonstrated that the blood glucose level was significantly higher in patients with complications than those without complications. A high blood glucose level is an independent risk factor of simultaneous DNI and cervical necrotizing fasciitis. 23
Thus, it should be monitored closely during hospitalization. Involvement of ≥3 deep neck spaces is associated with a longer length of hospital stay and higher rates of reoperation and mortality.24,25 However, involvement of multiple spaces is not an independent risk factor for ICU admission. Infection can spread rapidly between cervical spaces, which can worsen the clinical status of patients, which makes treatment challenging and predisposing to complications. Patients with a large abscess that is not located at a critical site and does not cause swallowing dysfunction are less likely to need ICU care.
Univariate and multivariate analyses revealed that older age, a higher CRP level, and mediastinitis are independent risk factors for ICU transfer in patients with DNI. Older patients are vulnerable and have more comorbidities, resulting in more complicated and unpredictable disease course. Previous studies have found that older patients had a longer length of hospital stay and higher risk of mortality.26,27 DNI typically involves a higher number of spaces in older patients than in those aged <18 years. 28 In addition, older age is a risk factor for the need of tracheostomy. 29 Older patients are more likely to have systemic diseases, such as hypertension and diabetes mellitus, and diabetes increases the risk of mortality in patients with DNI.21,30 Furthermore, patients aged >65 years had a longer hospital stay and poor response to antibiotics for DNI. 31 These patients are also predisposed to pneumonia because of the impaired gag reflex, decreased mucociliary function, waning immunity, impaired febrile response, and cardiopulmonary dysfunction. 32 Considering that the care of older patients is more complicated, older age is a risk factor for the need of ICU care in patients with DNI.
A higher CRP level is associated with more severe infection. In our study, the CRP level was significantly higher in the ICU group than in the non-ICU group, indicating that the former had more severe infection and inflammation and a higher risk of fatal complications. A previous study demonstrated that DNI patients with CRP level ˃100 mg/L had longer hospital stays. 33
Previous studies have demonstrated that the CRP level is highly correlated with the mortality rate and risk of cervical necrotizing fasciitis. 26 Ohata et al 34 found that the CRP level was significantly higher in older patients and those with diabetes mellitus or prolonged infections. Thus, it could be used to determine the need for ICU care in patients.
The diagnosis of mediastinitis is mainly based on characteristic radiographic features of mediastinitis. 11 Mediastinitis is a common potentially fatal complication of DNI. It can cause persistent infection, leading to the development of other diseases such as empyema, pericarditis, and vascular erosion. The mortality rate was significantly higher in patients with mediastinitis than in those without mediastinitis. 35 Gehrke et al 36 found that patients with mediastinitis exhibited significantly higher rates of surgical interventions and tracheotomy, elevated levels of inflammatory markers, a greater requirement for CT scans, prolonged hospitalization, and a higher likelihood of requiring changes in antibiotic therapy. Considering the intensive care required for patients with mediastinitis, clinicians should monitor the clinical condition carefully to determine the need for ICU transfer.
Airway management is essential in patients with DNI due to the potential airway compromise. Our study demonstrated that patients transferred to the ICU had a higher rate of tracheostomy. A previous study found that patients undergoing tracheotomy have a prolonged extended hospital stay, potentially attributable to the illness severity rather than the selected method of airway management. Similarly, we found that the ICU group had a longer length of hospital stay. Furthermore, Barber et al 37 demonstrated that airway compromise contributes to prolonged hospitalization. However, patients primarily treated with tracheotomy had a shorter ICU stay compared to those who were intubated without immediate extubation, although this difference was not statistically significant. Furthermore, performing tracheotomy within 7 days after intubation reduces the duration of artificial ventilation and length of ICU stay. 38 Mahafza et al 39 compared revealed that, compared to late tracheostomy, tracheotomy performed <3 weeks after intubation was associated with lower complication and mortality rates in the ICU (Table 5).
Findings and Descriptions Related With ICU Care of this Study in Literature.
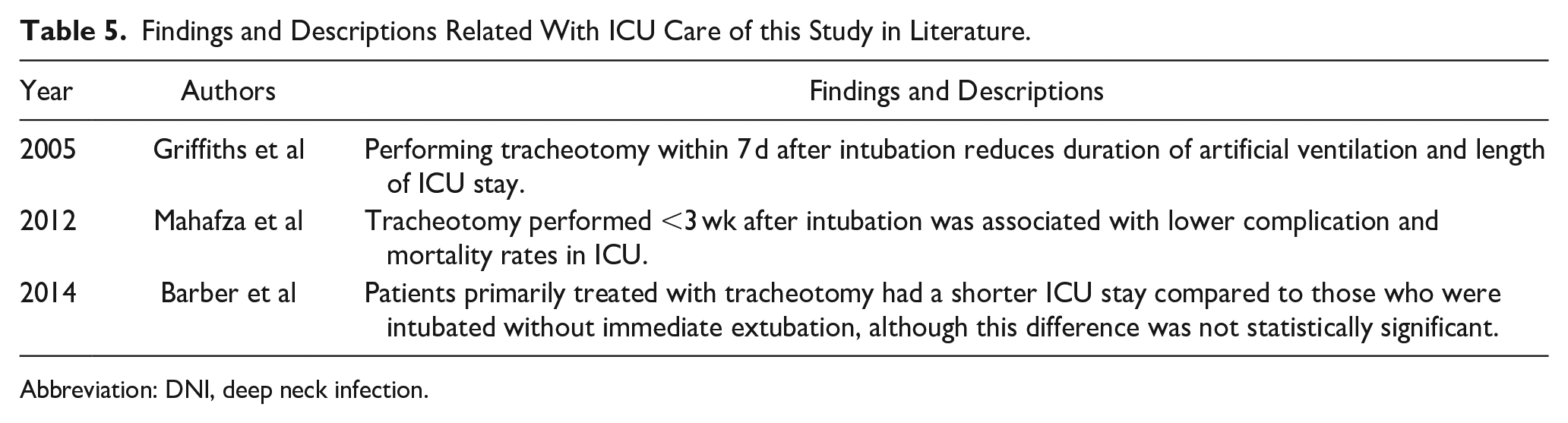
Abbreviation: DNI, deep neck infection.
Recently, artificial intelligence models have also been used to evaluate patients with DNI. One study retrospectively analyzed patients with DNI who underwent drainage surgery. Multivariable logistic regression analysis and the eXtrem Gradient Boosting algorithm were applied to develop a predictive model to guide clinical decisions for postoperative ICU admission in patients with DNI. 40
Our patients were initially treated with empirical, broad-spectrum, intravenous antibiotics, which were later adjusted based on culture results. There were no significant differences between patients admitted to the ICU and those who were not. In our cohort, S. constellatus was the most frequently isolated pathogen, followed by P. micra and P. intermedia. This contrasts with findings from previous studies, in which Streptococcus viridans, S. anginosus, K. pneumoniae, and Staphylococcus aureus were commonly isolated pathogens.13,41-43 Despite these differences, third-generation cephalosporin such as ceftriaxone plus metronidazole could effectively treat these pathogens. Empirical antibiotics were initiated and subsequently adjusted based on culture results. Considering the diverse pathogens associated with DNI, possibility of polymicrobial infections, and presence of aerobic and anaerobic organisms in the oropharyngeal microbial community, the selected antibiotics should cover both aerobic and anaerobic organisms. 44 When antibiotics have been administered previously, blood culture may not be a sensitive method for pathogen identification.45,46
Limitations of the Article
This study had several limitations. First, airway management, surgical procedures, and ICU transfer were based on surgeon discretion. Second, each hospital may have distinct protocols for transferring patients to the ICU, which makes comparisons between studies challenging. Furthermore, blood glucose is used more frequently as the presence of diabetes mellitus as a chronic disease and offers a more objective value in the literature. As a parameter, blood glucose in this article only represents the patient’s first arrival at the emergency room. Finally, this was a retrospective study conducted in a tertiary care hospital, which may be associated with suboptimal data collection.
Conclusion
This study evaluated the clinical risk factors for ICU admission in patients with DNI. Older patients and those with a higher CRP level and mediastinitis were more likely to be transferred to the ICU, resulting in a longer hospital stay and higher risk of tracheostomy. Clinicians should carefully evaluate patients regarding potential need for ICU transfer and promptly manage the airway based on the aforementioned laboratory parameters and complications.
Footnotes
Acknowledgements
The authors thank all of the members of Department of Otorhinolaryngology and Head and Neck Surgery, Linkou Chang Gung Memorial Hospital, for their invaluable help.
Author Contributions
Conceptualization: Y.C.H.; C.Y.H.; K.C.C; Y.C.W.; S.C.C.; S.L.C. Methodology: Y.C.H.; C.Y.H.; S.L.C. Validation: Y.C.H.; K.C.C; S.L.C. Data curation: Y.C.H.; S.L.C. Writing—original draft preparation: Y.C.H.; S.L.C. Writing—review and editing: S.L.C. Visualization: C.Y.H; S.C.C.; S.L.C. Supervision: Y.C.H.; Y.C.W.; S.L.C. Project administration: C.Y.H.; S.C.C.; S.L.C. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.