
Abstract
Objective:
To evaluate the hearing outcomes and complications of primary malleus head interposition ossiculoplasty during canal wall down (CWD) tympano-mastoidectomy surgery in patients with cholesteatoma.
Background:
Most ossiculoplasty techniques depend on interposition or reposition ossiculoplasty. Therefore, in cases where the Incus is eroded, the malleus becomes the only remaining ossicle and can be used for interposition ossiculoplasty.
Patients and Methods:
This prospective study included 27 patients with cholesteatoma. All patients received primary malleus head interposition ossiculoplasty during CWD tympano-mastoidectomy. Follow-up of patients carried out in an outpatient clinic through routine follow-up visits at 1, 3, and 6 months using a pure tone audiometer.
Results:
Postoperative air bone gab (ABG) closure had values of 11.03, 9.63, 8.96, and 10.7 dB at 500, 1000, 2000, and 4000 Hz, respectively. The mean postoperative ABG decreased from 33.81 ± 5.69 to 24.85 ± 3.08 dB with an improvement of 9 dB that was statistically significant (P < .001).
Conclusions:
The malleus head interposition technique is simple and effective for ossiculoplasty in CWD tympano-mastoidectomy. This technique was considered effective in enhancing the stability of the graft and the efficacy of the overall ossiculoplasty procedure. It is characterized by availability, low cost, and low complication rate.
Introduction
Ossiculoplasty refers to the surgical reconstruction of the disrupted or damaged ossicles using techniques such as interposition or reposition. These techniques aim to reestablish the normal mechanics of the ossicles, allowing efficient conduction of sound. 1 The main goal of ossiculoplasty is to improve conductive hearing loss, especially for conversational speech, thereby enhancing the patient’s overall auditory function. 2 The incus is the most common ossicle to be eroded by cholesteatoma, with a ratio of total loss in 55.4% of patients and partial damage in 30.7%. 3 Ossiculoplasty can involve the use of natural materials, including autografts or homografts, and synthetic prostheses, including total and partial ossicular reconstruction prosthesis (TORP and PORP), like polyethylene, ceramic, hydroxyapatite, or titanium. 4 Synthetic materials have drawbacks of being costly and correlated with extrusion and displacement in spite of hydroxyapatite and titanium have become more successful with acceptable extrusion rates.5,6 By contrast, autografts including ossicle, cortical bone, and cartilage have the advantage of being easy to obtain from the same surgical site, having lower extrusion rates, being nontoxic, and showing minimal shrinkage and lateralization. 5
Various ossiculoplasty prostheses and techniques have been researched and documented in the literature. Common techniques such as incus or malleus interposition and malleus relocation techniques have achieved good results. Although there is considerable literature on the use of the incus in ossiculoplasty, there is limited research focusing on the malleus and its outcomes. Malleus may be the only autologous ossicle to be used when the incus is absent or eroded, with better options and results, especially during canal wall down (CWD) tympano-mastoidectomy. The malleus head interposition technique requires an intact and mobile stapes suprastructure as well as a mobile and appropriately positioned malleus. The objective of this study is to assess the outcomes of this technique during CWD tympano-mastoidectomy in patients with cholesteatoma, focusing on postoperative hearing outcomes and potential complications.
Patients and Methods
The study was a prospective study that included 27 patients diagnosed with cholesteatoma. The study was conducted between September 2022 and September 2024 with ethical approval of the Ethics Committee of the Menoufia Faculty of Medicine, with the IRB date and number 9/2022 ENT 35, and all patients provided written informed consent before the surgery.
The study depended on the EAONO/JOS staging system in the classification of patients. 7 The selected patients had cholesteatoma diagnosed by clinical and radiological evaluations. Patients with prior ear surgeries, mixed hearing loss, congenital anomalies, or maxillofacial malformations were excluded. All patients had been evaluated by history taking, clinical examination, radiological evaluation by high-resolution computed tomography (CT) temporal bone with coronal and axial cuts without contrast, and audiological testing by pure tone audiometer (PTA) using a diagnostic audiometer. ABG was determined as the average difference between the thresholds for air and bone conduction across different frequencies. A microscopic examination was performed to assess the perforation site and the condition of the ossicles before surgery. The patients were classified according to preoperative and postoperative ABG in 3 categories (20-30, 31-40, and <40 dB).
The surgical procedure involved performing CWD tympano-mastoidectomy with primary malleus head interposition ossiculoplasty in a single session. Under general anesthesia, through a post-auricular approach, a CWD tympano-mastoidectomy was performed. The malleus was carefully separated from the tensor tympani muscle, the tympanic membrane, and associated ligaments. The malleus head was reshaped with a burr to create a facet that fits securely over the stapes suprastructure. The reshaped malleus head was positioned and stabilized using gelfoam (Figure 1).
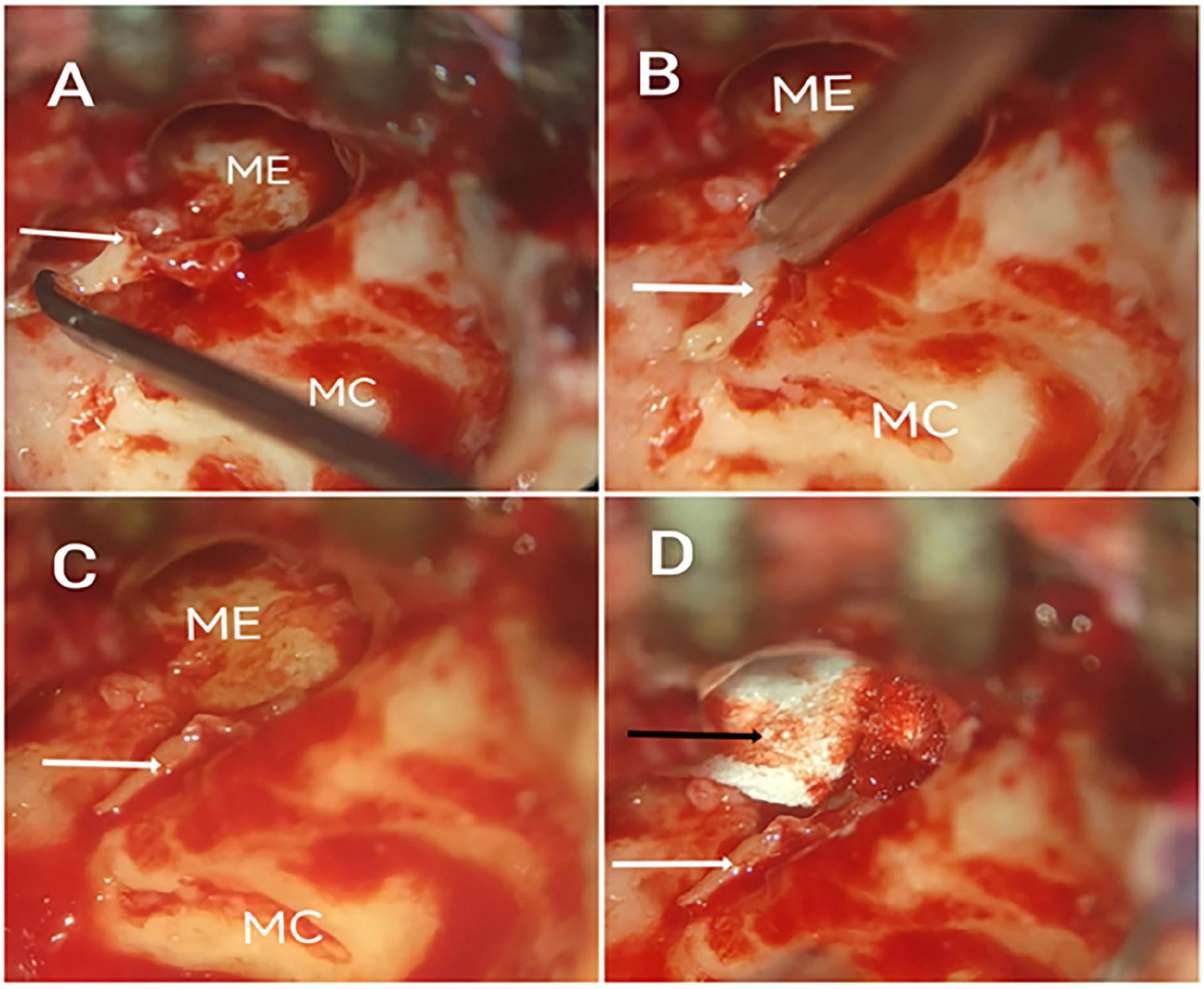
Steps of malleus head interposition ossiculoplasty. (A) malleus (white arrow) is cleared from associated ligaments. (B) malleus head (white arrow) is fitted on head of stapes. (C) malleus is well situated and positioned over stapes suprastructure. (D) malleus is fixed by gelfoam (black arrow). ME, middle ear; MC, mastoid cavity.
Then, the temporalis fascia graft was harvested and fitted over the cavity. Meatoplasty was performed in all patients.
All patients are followed up in the outpatient clinic through routine follow-up visits at 1, 3, and 6 months to identify the outcomes. Each ear was examined after 6 months within 2 years under the microscope with intensive ear clearance to ensure good clearance, epithelialization, and no complications were found. Each patient was followed up after 6 months with PTA reported as pure tone average represented as hearing threshold at frequencies 500, 1000, 2000, and 4000 Hz according to the guidelines of the American Academy of Otolaryngology. 8 Complications of the technique were recorded during the study.
Statistical analysis was performed with SPSS (IBM, Armonk, NY, USA) version 26 and open source epidemiological statistics for public health version 3.01. P < .05 was considered statistically significant.
Results
The demographic data of the studied patients were of 9 males (33.3%) and 18 females (66.8%) with mean age = 27.44 ± 13.06. The majority of patients (62.9%) were from rural areas (Table 1).
Demographic Data of the Studied Patients (N = 27).
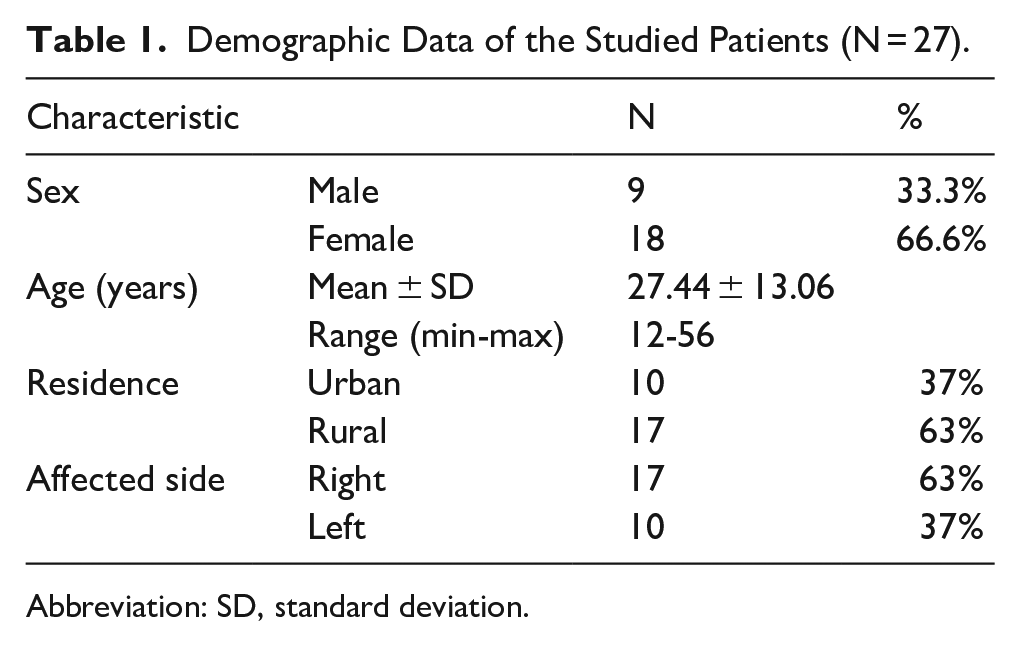
Abbreviation: SD, standard deviation.
According to the EAONO/JOS systems, 18 patients (66.6%) were in stage 1, 7 patients (26 %) in stage 2, and 2 patients (7.4 %) were in stage 3 who had facial palsy due to facial canal dehiscence and improved during postoperative follow-up.
The postoperative follow-up of the studied patients after the surgery revealed that 2 patients (7.4%) had a dehiscent wound, while 25 patients (92.5%) had no wound complications. Twenty-two patients (81.5%) had early cavity epithelialization <3 months, and the remaining 5 patients (18.5%) had delayed cavity epithelialization >3 months. In the malleus condition, during follow-up, there was no extrusion, protrusion, or lateralization of the malleus. No bone resorption. No patient in the study had recurrent disease during follow-up.
According to pre- and postoperative ABG, 5 patients (18.5%) were at 20 to 30 dB before the surgery. 4 of them (14.8%) improved and were still at 20 to 30 dB, and 1 patient deteriorated to 31 to 40 dB during postoperative follow-up.
Eighteen patients (66.6%) were at 31 to 40 dB. Ten of them (37%) improved to 20 to 30 dB, 7 patients were still at 31 to 40 dB (25.9%), and 1 patient deteriorated >40 dB.
Four patients (14.8%) were >40 dB. Two patients improved and became at 31 to 40 dB (7.4%). And 2 were still >40 dB (7.4%; Table 2).
Comparison Between Pre- and Postoperative ABG of the Studied Patients at Different Ranges (N = 27).
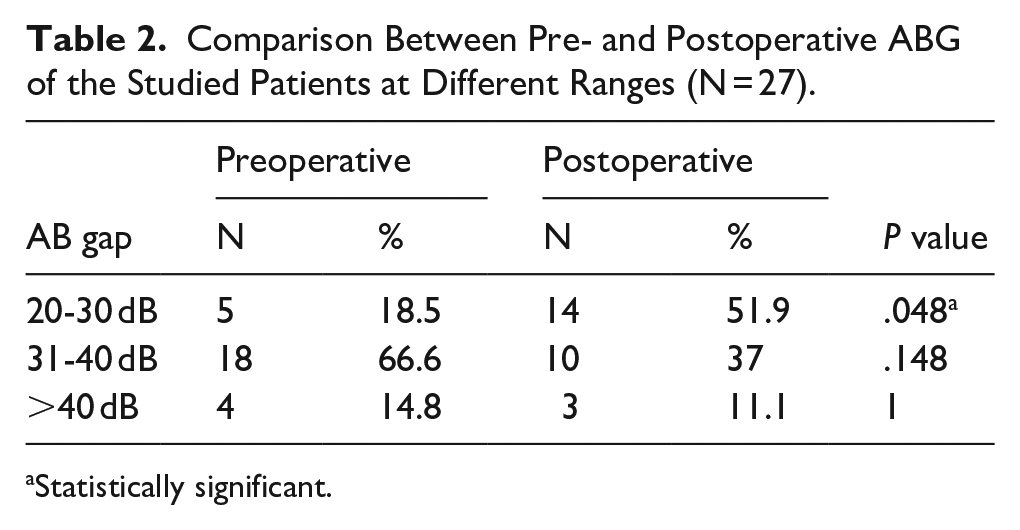
Statistically significant.
According to preoperative and postoperative ABG at different frequencies, there was ABG closure about 11.03, 9.63, 8.96, and 10.7 dB at 500, 1000, 2000, and 4000 Hz. (The P value is statistically highly significant <.001.) The mean preoperative ABG was 33.81 ± 5.69 dB. A significant improvement was observed with closure of the postoperative ABG to an average of 24.85 ± 3.08 dB with an improvement of 9 dB, which was statistically significant as determined by a paired t-test (P < .001; Table 3).
Comparison Between ABG of the Studied Patients Pre- and Postoperative at Different Frequencies and Mean ABG.
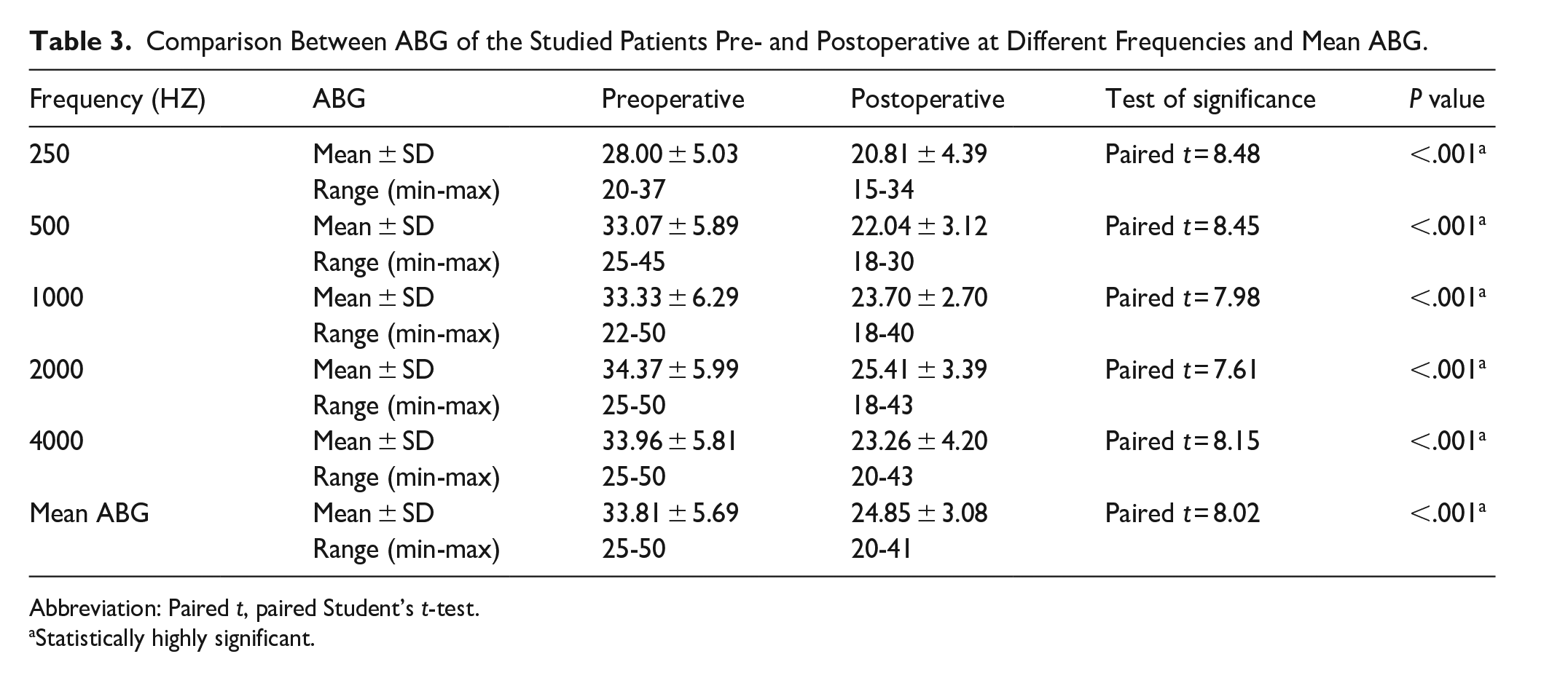
Abbreviation: Paired t, paired Student’s t-test.
Statistically highly significant.
Discussion
In choleastetoma, the incus is the most commonly eroded ossicle. Therefore, in such a situation, autograft malleus or myringostapedopexy remains a valuable option in developing countries with low resources. These options are advantageous due to their availability and lower complication rates in contrast with synthetic prostheses, which are costly and associated with a higher rate of extrusion. Our technique provides the surgeon with a wide range of options in selecting the appropriate technique during CWD surgery.
Our study focused on the evaluation of the hearing outcomes of malleus head interposition ossiculoplasty performed after CWD tympano-mastoidectomy in patients with cholesteatoma.
During cholesteatoma surgery, the main purpose of the surgery is to save the ear and prevent complications. Then, the hearing improvement comes in the second position. So, just keeping the hearing level consistent in a certain range and preventing its deterioration preoperatively and postoperatively is considered a success for the technique. So, any new techniques are acceptable to try improving the hearing outcomes and quality of life after the surgery.
Delayed cavity epithelialization in 5 patients (18.5%) during the study may be due to a lack of clearance and insufficient follow-up visits in low socioeconomic areas.
In our study, the mean preoperative ABG value was 33.81 ± 5.69 dB, which improved to 24.85 ± 3.08 dB postoperatively, with postoperative ABG closure ~9 dB (P < .001).
This aligns with the study by Shewel and Abougabal, which used the incus interposition technique in CWD surgery and revealed a significant improvement in the mean postoperative ABG from 30 ± 5 to 20 ± 5.8 dB (P < .0001). They also used TORP in 18 ears and had a preoperative ABG of 31 ± 6.2 dB with a postoperative ABG of 24 ± 6.8 dB. 9
Similarly, Karamert et al in their study used autograft malleus, incus, and cortical bone during CWD surgery in 56 (73.6%) patients and reported that the improvement in mean ABG was from 31.4 to 24.8 dB (P < .001). 10 Quaranta et al used a costal cartilage autograft and revealed that in CWD, postoperative ABG improved from 38.6 ± 9.4 to 29.6 ± 12 dB. 11
In another study by Michelle et al, who used cartilage ossiculoplasty in the T0 group after CWD surgery and showed an improvement in postoperative ABG from 27.5 ± 12.2 to 24.4 ± 14.1 dB. They also compared tympanoplasty with PORP and TORP after CWD surgery and revealed that in the PORP group, ABG decreased from 20.5 ± 10.0 to 13.6 ± 11.5 dB, and in the TORP group from 16.3 ± 13.3 to 13.4 ± 12.0 dB. 12
Goyal et al used the myringostapidopexy technique during CWD mastoidectomy and showed an improvement in postoperative ABG from 33.65 to 18.03 dB. 13 Gu and Chi used titanium TORP in CWD tympano-mastoidectomy and observed that postoperative ABG decreased from 28.1 ± 9.8 to 20.1 ± 9.0 dB, achieving an ABG closure of 8.0 ± 7.9 dB (P < .01). 14
According to our study, removal of the malleus head and the eroded incus during CWD tympano-mastoidectomy allows full ear exploration and disease eradication. Interposition of the malleus head on the stapes provides more stability of the graft, reducing ABG and improving hearing outcomes. Notably, none of the previous studies used our technique in CWD tympano-mastoidectomy in patients with cholesteatoma, despite its simplicity and minimal complications. This technique offers significant advantages for achieving favorable hearing outcomes.
The malleus head interposition technique requires an intact malleus and eroded incus. So, it is not recommended in cases of partial or complete erosion of the malleus head, which is less common. Other ossiculoplasty techniques may be used like myringostapedopexy, cartilage, or allograft prostheses. In cases of absent stapes suprastructures, TORP is recommended.
Limitations
The small sample size of the study and the short follow-up duration limit the ability to obtain robust statistical results and to thoroughly assess the long-term outcomes of the technique. In addition, performing statistical analysis on small groups may result in overestimated or misleading conclusions.
Conclusions
The malleus head interposition technique is a simple and effective technique for ossiculoplasty in CWD tympano-mastoidectomy, especially in cases of cholesteatoma that necessitate thorough ear exploration. This technique achieved acceptable results in comparison with synthetic prostheses and cartilage ossiculoplasty.
Footnotes
Ethical Considerations
This study received ethical approval from the Ethics Committee of the Menoufia Faculty of Medicine with the IRB date and number 9/2022 ENT 35.
Consent to Participate
All patients provided written informed consent prior to the surgery.
Author Contributions
Tarek Abdelrahman Abdelhafez: concepts; design; definition of intellectual content; literature search; clinical studies; data acquisition; manuscript preparation; manuscript review. Ahmed Ragab: design; clinical studies; experimental studies; data analysis; manuscript preparation; manuscript editing; manuscript editing. Ayman Ali Abdelfattah: concepts; design; clinical studies; data acquisition; data analysis; manuscript preparation; manuscript editing. Ahmed Sami Tahoun: design; definition of intellectual content; clinical studies; experimental studies; data analysis; manuscript editing; manuscript editing. Anwar Abdelaty Ibrahim: design; definition of intellectual content; clinical studies; experimental studies; data analysis; manuscript editing; manuscript editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting study findings are not publicly available due to privacy restrictions of the patients.