
Abstract
Background
Deep neck infection (DNI) is a severe infectious disorder of deep neck spaces that can cause serious complications. Long-term hospitalization is when a patient spends more time in the hospital than originally expected for a disease. There are few studies assessing the risk factors associated with long-term hospitalization for a DNI. This study investigated the factors causing DNI patients to experience long-term hospitalization.
Methods
Long-term hospitalization is defined as a length of hospital stay exceeding 28 days (> 4 weeks) in this research. A total of 362 subjects with a DNI between October 2017 and November 2022 were recruited. Among these patients, 20 required long-term hospitalization. The relevant clinical variables were assessed.
Results
In a univariate analysis, C-reactive protein (odds ratio [OR] = 1.003, 95% CI: 1.000−1.007, P = .044), involvement of ≥3 deep neck spaces (OR = 2.836, 95% CI: 1.140−7.050, P = .024), and mediastinitis (OR = 8.102, 95% CI: 3.041−21.58, P < .001) were significant risk factors for long-term hospitalization in DNI patients. In a multivariate analysis, mediastinitis (OR = 6.018, 95% CI: 2.058–17.59, P = .001) was a significant independent risk factor for long-term hospitalization for a DNI. There were no significant differences in pathogens between the patients with and without long-term hospitalization (all P > .05). However, the rates of no growth of specific pathogens were significantly different between patients with and without long-term hospitalization, and those with long-term hospitalization had greater rates of growth of specific pathogens (P = .032). The rate of tracheostomy in patients with long-term hospitalization was higher than for those without (P < .001). Nevertheless, the rates of surgical incision and drainage between patients with and without long-term hospitalization did not achieve statistical significance (P = .069).
Conclusions
Deep neck infection (DNI) is a critical, life-threatening disease that could lead to long-term hospitalization. The higher CRP and involvement of ≥3 deep neck spaces were significant risk factors in univariate analysis, while concurrent mediastinitis was an independent risk factor associated with long-term hospitalization. We suggest intensive care and prompt airway protection for DNI patients with concurrent mediastinitis.
Keywords
Introduction
Deep neck infection (DNI) is a dangerous bacterial infection that invades through cervical fascial planes and deep neck spaces.1,2 DNI is a clinical challenge for physicians due to the potential of a compromised airway, the complexity of the anatomy in the head and neck area, and the risk of spread of the infection into adjacent regions. 3 Despite the broad availability of antibiotics, improved diagnostic techniques, and timely surgery, 4 DNI can still cause a patient to have a long-term hospitalization.
Long-term hospitalization at our hospital is defined as a hospital stay lasting over 28 days (>4 weeks). Previous studies have found that patients with diabetes mellitus (DM), and other comorbid conditions have a prolonged length of hospital stay.5-7
Long-term hospitalization not only causes physical and mental stress for patients and their families, it also imposes a burden on the medical system. Thus, it is important to identify the clinical, laboratory, radiological, and pathogen factors that might predispose DNI patients to long-term hospitalization; however, there have been few studies of this issue.
In this study, we investigated the factors causing DNI patients to experience long-term hospitalization.
Materials and Methods
We retrospectively reviewed the medical charts of 362 patients diagnosed with DNI who were admitted to Chang Gung Memorial Hospital (Linkou, Taiwan) between October 2017 and November 2022. DNI was evaluated clinically, using computed tomography (CT) as a standard and essential imaging tool.8-10 The treatment course included antibiotics as well as surgical incision and drainage (I&D) as necessary. 11 I&D at our hospital is used when a DNI compromises the airway, the abscess is large (≥2 cm), and/or if there is no improvement in the DNI after 48 hours of intravenous empirical antibiotics. 12 Airway security included either intubation or tracheostomy. 13
The application of the antibiotics ceftriaxone (1 g, Q12h) and metronidazole (500 mg, Q8h) was based on previous reports to cover aerobic and anaerobic bacteria before the final culture results were available.14,15 In addition to antibiotic administration, postoperative wound irrigation is commonly required to obtain a better outcome and prognosis for DNI patients. 16
Postoperative irrigation was performed every 8 hours by doctors corresponding to the disease severity. 17 If there was any progression in symptoms after primary treatment, repeat CT was conducted, with the possibility of a second operation for some patients during their hospital stay. 18 At our hospital, long-term hospitalization is defined as a length of hospital stay exceeding 28 days (>4 weeks).
Exclusion Criteria
The exclusion criteria were: patients <18 years of age, those with mis-swallowing of a foreign body, severe cardiopulmonary disease, previous head and neck tumor surgery, previous history of head and neck malignancy, 19 or those with previous chemoradiotherapy over the head and neck region. A total of 362 patients with DNI were enrolled in the study, of which 20 required long-term hospitalization.
Data Collection
We collected data on the patients’ gender, age, C-reactive protein (CRP) level, blood sugar level, DM status, multiple deep neck space involvement (≥3), the different deep neck spaces involved, presence of mediastinitis, species of pathogens, tracheostomy, performance of surgical I&D, and length of hospital stay.
Ethics Statement
All data were collected retrospectively. This study was approved by the Institutional Review Board (IRB) of the Chang Gung Medical Foundation (IRB no. 202201841B0). The IRB waived the need for informed consent. The patients were anonymized before data analysis.
Statistical Analysis
All data in this research were analyzed by MedCalc software (ver. 18.6; MedCalc, Ostend, Belgium). Because the Kolmogorov–Smirnov test displayed that the data were not distributed normally, we used the chi-square test for categorical variables. The Mann–Whitney U test was applied for the comparison of continuous variables. Logistic regression was utilized for univariate and multivariate analyses. A multivariate forward stepwise selection procedure was employed, and all of the variables in the univariate analysis were entered into the ultimate multivariate model. Statistical significance was set at P < .05.
Results
Clinical Characteristics of all 362 DNI Patients.
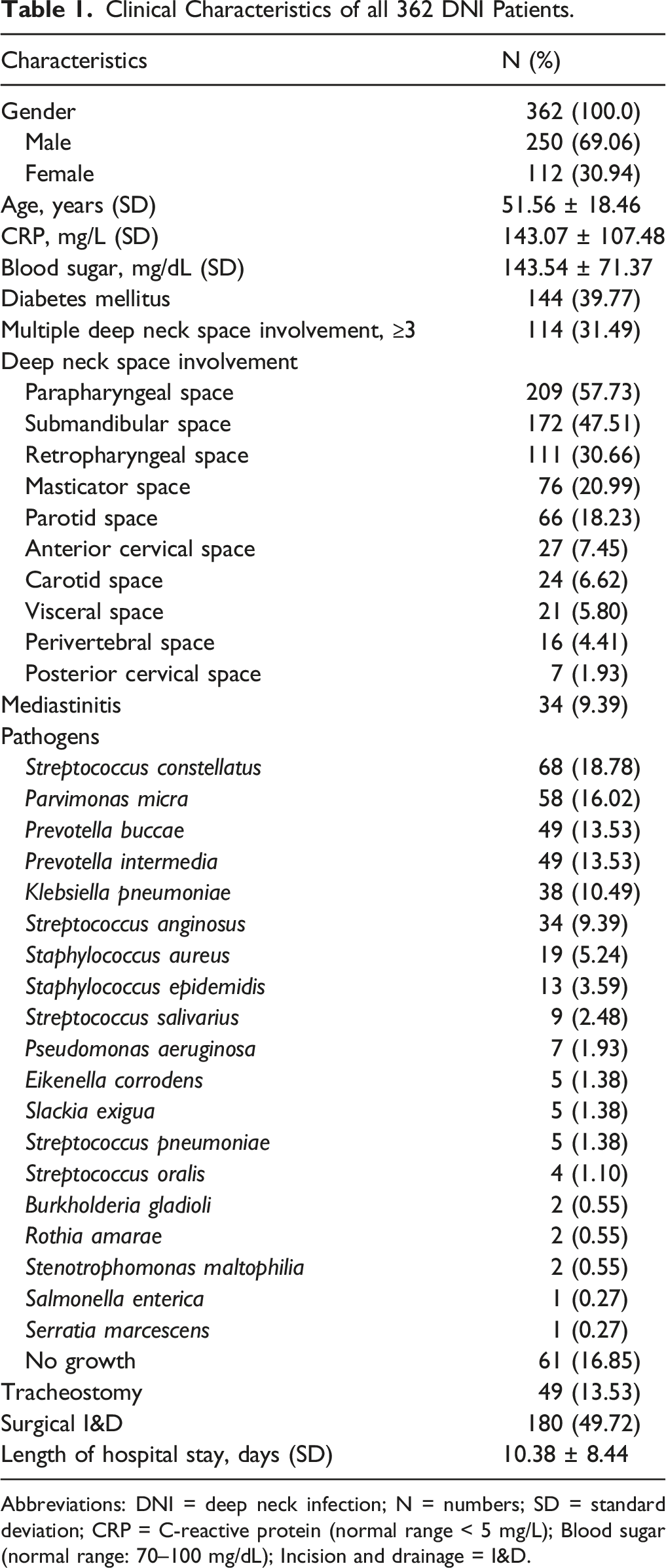
Abbreviations: DNI = deep neck infection; N = numbers; SD = standard deviation; CRP = C-reactive protein (normal range < 5 mg/L); Blood sugar (normal range: 70–100 mg/dL); Incision and drainage = I&D.
A total of 114 (31.49%) patients had involvement of ≥3 deep neck spaces. The different deep neck spaces involved was presented in Table 1. Mediastinitis was detected in 34 (9.39%) patients.
Table 1 also lists the pathogens cultured from the DNI patients. The non-growth of a specific pathogen was detected in 61 (16.85%) patients. Tracheostomy was performed in 49 (13.53%) patients. A total of 180 (49.72%) patients underwent surgical I&D for DNI. The overall mean length of the hospital stay was 10.38 ± 8.44 days.
Univariate and Multivariate Analysis Results of DNI Patients With Long-Term Hospitalization.
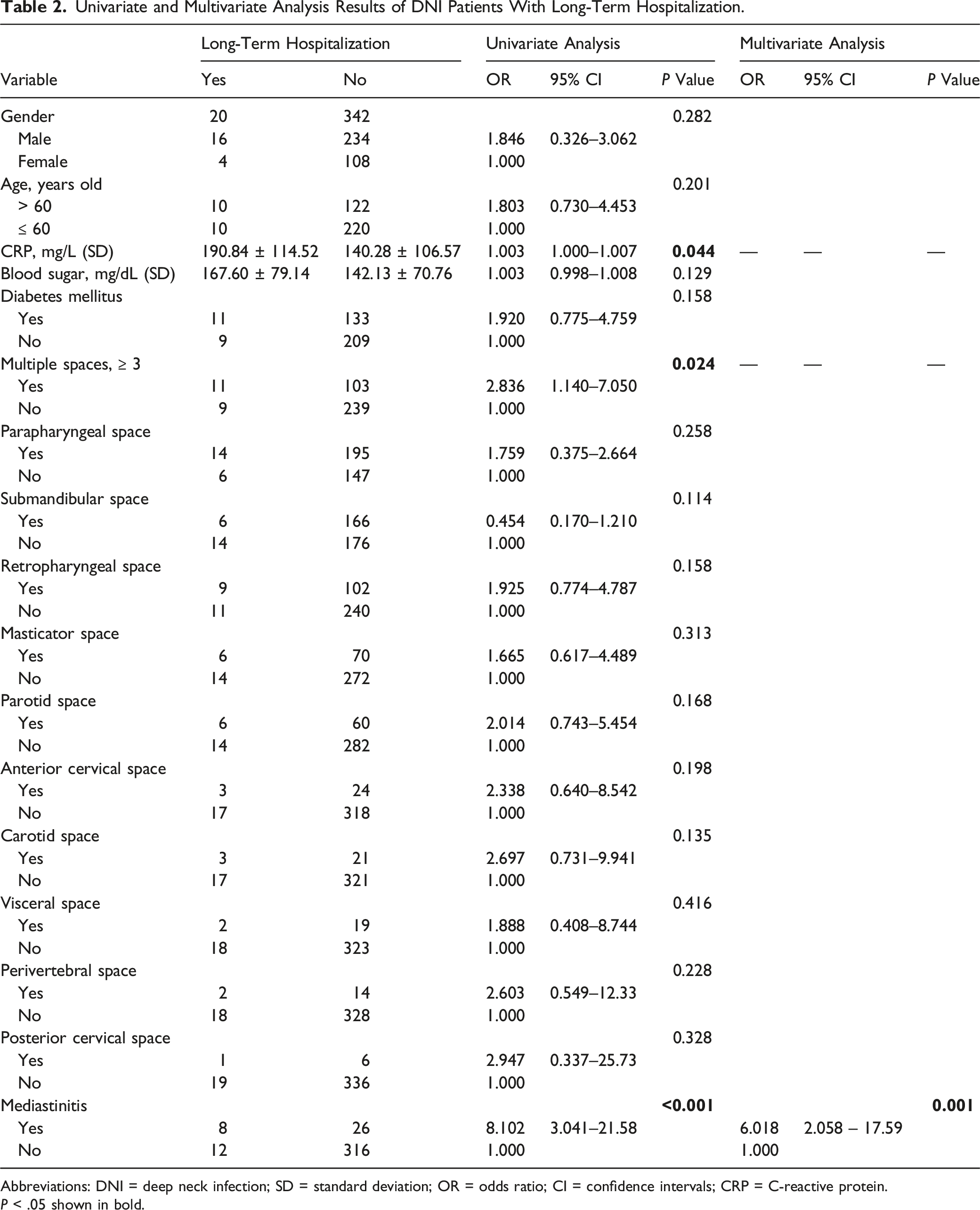
Abbreviations: DNI = deep neck infection; SD = standard deviation; OR = odds ratio; CI = confidence intervals; CRP = C-reactive protein.
P < .05 shown in bold.
Comparison of Pathogens Between DNI Patients With and Without Long-Term Hospitalization.
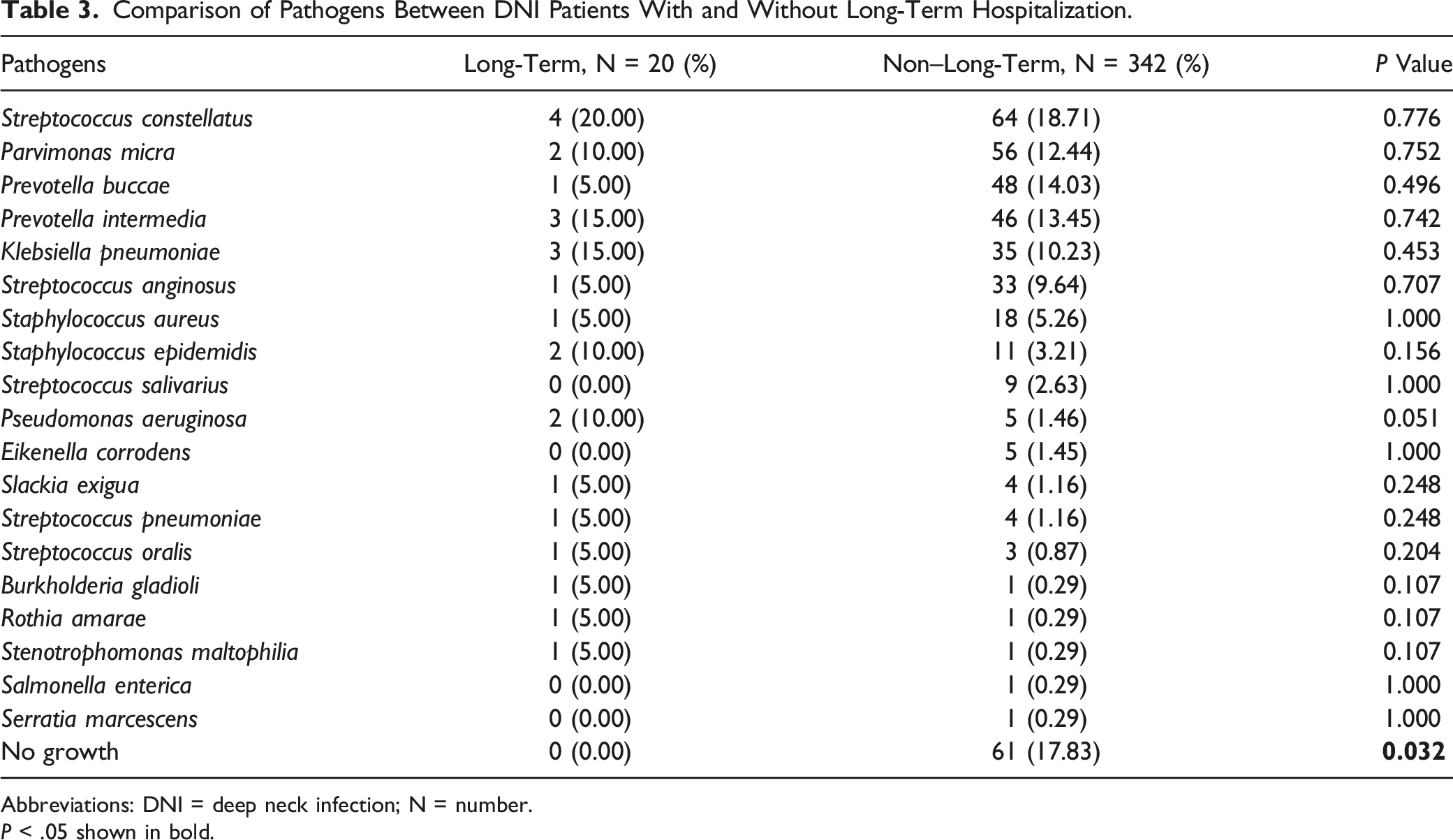
Abbreviations: DNI = deep neck infection; N = number.
P < .05 shown in bold.
Comparison of Intervention and Length of Hospital Stay Between DNI Patients With and Without Long-Term Hospitalization.
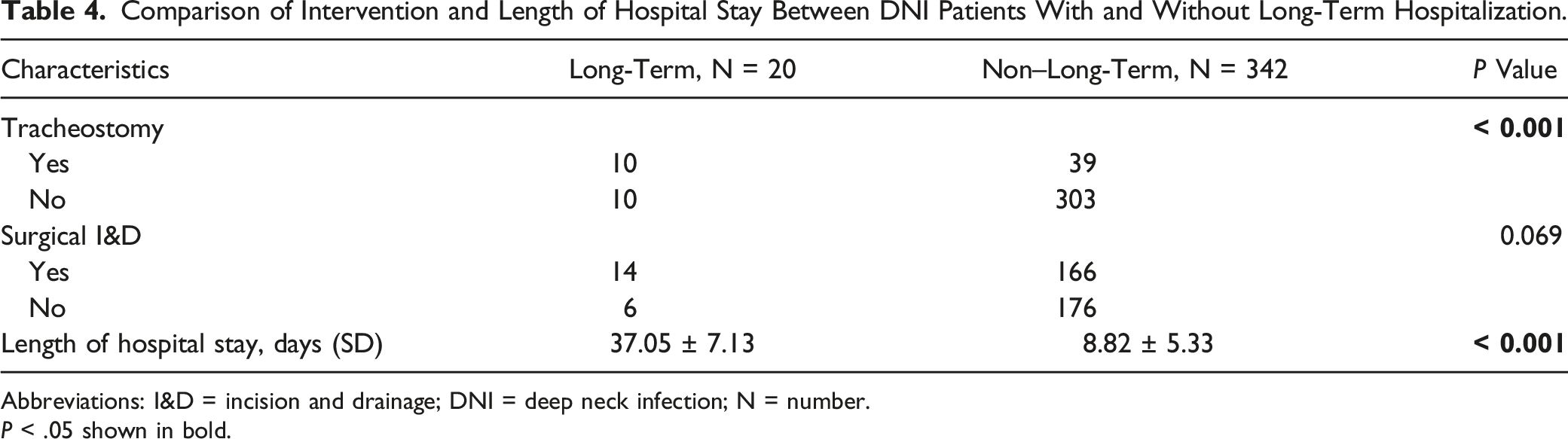
Abbreviations: I&D = incision and drainage; DNI = deep neck infection; N = number.
P < .05 shown in bold.
Discussion
Deep neck infections (DNIs) remain a clinical difficulty for physicians from medical, surgical, and even socioeconomic perspectives.6,20 During the pre-antibiotic era, most DNIs followed peritonsillar infections. Currently, the most common infection source appears to be odontogenic. 6 However, in nearly 50% of DNI patients, the origin of the infection is unknown.21,22 The management of DNI includes airway protection such as intubation or tracheostomy, timely surgical drainage, and broad-spectrum intravenous antibiotics. 23
Deep neck infection (DNI) can cause various complications, including emphysema, pericarditis, necrotizing fasciitis, aspiration pneumonia, vertebral osteomyelitis, epidural abscess, esophageal perforation, lung abscess, severe sepsis, aortic-pulmonary fistula, acute renal failure, carotid artery erosion, cavernous sinus thrombosis, descending necrotizing mediastinitis, disseminated intravascular coagulation, cranial nerve palsies, thrombophlebitis of the internal jugular vein, hematogenous dissemination to distant organs, and even mortality.3,7,14,24-37 Some risk factors such as DM, as well as end-stage renal disease, have been shown to be associated with a higher risk of complications.2,38
Deep neck infection (DNI) in adult patients occurs mostly in men, with the highest incidence in those ranging from 40 to 60 years in age.39,40 This is in concordance with the results shown in Table 1. In fact, older age is a known risk factor for DNI. 41 Some authors have associated longer hospital stays with patients older than 65 years. 25 In this research, the overall tracheostomy rate was (13.53%), which is consistent with Velhonoja et al. 1 (13.0%). The mean hospital stay of our patients was 10.38 days; Parhiscar et al. 42 reported 9.5 days, while Ridder et al. 43 indicated a mean hospital stay of 13.1 days.
A higher CRP level, ≥3 deep neck spaces, and mediastinitis were risk factors for long-term hospitalization for DNI patients in univariate analysis (Table 2). CRP is produced in the liver as part of an acute response to stimulation by certain biomarkers from sites of inflammation. 44 Liu et al. 41 found CRP to be an independent factor correlated with persistent discharge. Wang et al. 45 found that patients with a higher CRP level were more likely to have complicated DNIs, resulting in prolonged hospitalization.
Clinical manifestations of DNI depend on the spaces involved and include pain, swelling, odynophagia, dysphagia, trismus, dysphonia, and dyspnea. 46 In our research, the parapharyngeal space was the most commonly identified location for a DNI, followed by the submandibular space. Nonetheless, we did not find a difference between the different abscess sites and length of hospitalization. In addition, an infection is expected to be advanced when the DNI involves multiple spaces. 1 The incidence of multiple space involvement has remained significantly higher in patients with DM, and DNI patients with DM showed significantly longer hospitalizations than patients without DM. 33 Srivanitchapoom et al. 47 showed that white blood cell counts are correlated significantly with multiple space involvement on univariate analysis. Some have also indicated the involvement of multiple deep neck spaces as an independent predictor of complications.7,39 Others have considered multiple deep neck space involvement as a risk factor for mortality in DNI patients, and that elderly patients with DNI also tended to have more multiple space involvement. 48 In fact, the need for repeated surgery is more likely in multiple-space DNI patients, which, in turn, leads to long-term hospitalization.
Multivariate analysis is a statistical tool for detecting the distinctive contributions of several factors to single events. 49 This statistical assessment can find which clinical variables are related to an adverse prognosis independently. 7 Our results revealed mediastinitis as an independent risk factor for long-term hospitalization with DNI in both univariate and multivariate analyses.
Mediastinitis is a mortal infectious disease, in which a DNI spreads along the cervical fascia and the neck spaces and down to the mediastinum (Figure 1A and B).
50
The spread of an infection toward the mediastinum is facilitated by gravity and negative intrathoracic pressure during respiration.51,52 The most important route for a descending infection reported in the literature is the retropharyngeal space.46,53 Celakovsky et al.
53
reported the predisposing factors for mediastinal extension of a DNI as cardiovascular and pulmonary diseases. Some have shown that risk factors such as DM, chronic renal failure, human immunodeficiency virus infection, and alcoholism contribute to the extension of DNIs into the mediastinal space.
54
Tapiovaara et al.
3
also found that mediastinal involvement prolongs the requirement for hospitalization. Currently, multidisciplinary approaches and comprehensive medical treatment can significantly reduce the mortality caused by mediastinitis.
28
(A) Computed tomography axial view and (B) coronal view of a deep neck infection (DNI) patient with mediastinitis. Arrowhead: mediastinitis; arrow line, the direction of DNI progression and invasion into the mediastinum.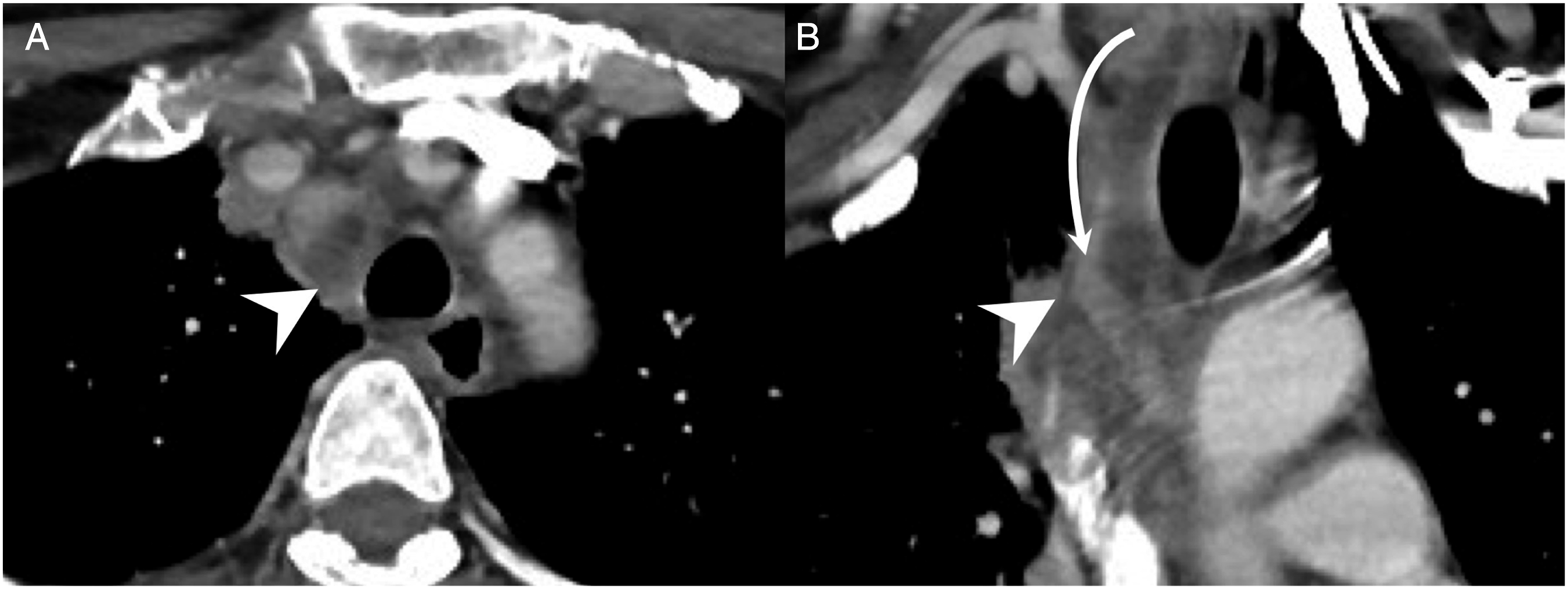
Usually, DNIs are polymicrobial in nature. 20 The most common cause of DNIs is considered to be odontogenic, 42 and the oral flora is composed of a mixture of aerobic and anaerobic bacteria. 55 Poor oral hygiene influences the host’s vulnerability to systemic illnesses by the formation of subgingival biofilms as reservoirs for Gram negative bacteria. 56 The microbiology of DNIs may change with time, and the resistance to antibiotics may affect the selection of empiric antibiotics. 25 Antibiotic therapy should always be modified by the culture and sensitivity findings while a specimen is obtained. 57 Yang et al. 25 found that compared with patients who had received effective antibiotics, the duration of hospital stay for patients with ineffective empiric antibiotics is significantly longer. The most common pathogen in the current study was Streptococcus constellatus; this finding is consistent with those of previous studies. 13 Streptococcus species are considered to be the most commonly isolated pathogen in the non-DM group, whereas Klebsiella species are the most common in DM patients.58,59
Parhiscar et al. 42 found no bacterial growth in 13% of cases. In our study, the overall rate of specific pathogen non-growth was 16.85% (Table 1). However, the long-term hospitalization group had 0% non-growth pathogens, whereas the group without a long-term hospital stay had 17.83% non-growth pathogens, as shown in Table 3. Some studies have indicated that no organism was cultured; this may have been due to the use of antibiotics at the time the cultures were sent. 20 In fact, when antibiotics have already been administered, blood culture is not a sensitive method for identifying pathogens.52,60 In addition, the utility antibiotics has greatly decreased the incidence of abscesses but has led to growing rates of antibiotic resistance.61–63
Due to the potential for airway obstruction, proper protection of the airway with close surveillance of respiratory function is important for DNI management. 64 Otolaryngologists and anesthesiologists should evaluate patients immediately for airway security. 65 In DNI, tracheostomy is used as the gold standard for the management of a compromised airway. 66 In Table 4, the group experiencing long-term hospitalization had a higher rate of tracheostomy conduction. Barber et al. 6 reported that a compromised airway prolongs hospitalization. However, Tapiovaara et al. 3 reported that tracheostomy patients requiring longer-term hospital care is a result of the disease, and not the chosen method of airway management.
For long-term hospitalization, several paramedical factors and DNI severity are highly related. Geographic location and education level are also associated with DNI severity. 6 Some studies found that patients presenting to a tertiary care center from a geographic location >1 hour away had more severe DNI; this is because remote access to health care could lead to delayed presentation, thus resulting in a greater degree of airway compromise requiring critical intervention. 6 Rzepakowska et al. 24 also found that patients with hemoglobin levels <12.5 g/dL had significantly longer periods of hospitalization.
Some found that DM patients have a longer hospital stay than patients without DM, and their results were significant.67,68 Others have confirmed the link between gas formation and a more severe course of DNI, with a higher complication rate, increased mortality, and longer hospitalization. 1 In another study, unplanned reoperations tended to increase the length of the hospital stay, with no improvement in prognosis. 69 However, O’Brien et al. 2 demonstrated that the presence of a drain is not significant regarding the length of the hospital stay. This may encourage surgeons to utilize drains as medically indicated, with improved confidence that it should not significantly affect the postoperative length of hospital stay.
Study Limitations
In this research, choice of airway management, the surgical procedure, and even clinical treatments were based on the surgeons’ preferences. Additionally, the study was retrospective and performed at a single tertiary hospital. Complete medical history recruitment and data collection could be suboptimal in this study design. Furthermore, each hospital has different definitions of long-term hospitalization,6,7 thus making the comparison of different studies more difficult. In this article, we didn’t analyze mortality rates in the long-term and non–long-term hospital stay groups. A future prospective study to further assess the length of hospital stay would provide more evidence on this issue.
Conclusion
Deep neck infection (DNI) is a lethal and life-threatening illness, and mediastinitis was identified as an independent risk factor associated with long-term hospitalization in this study. Identifying risk factors for long-term hospitalization in DNI patients allows clinicians to provide appropriate and timely treatment to manage the infection. We suggest intensive care and prompt airway protection for DNI patients with mediastinitis.
Footnotes
Acknowledgments
The authors thank all of the members of Department of Otorhinolaryngology-Head and Neck Surgery, Chang Gung Memorial Hospital, Linkou, for their invaluable help.
Authors’ Note
Author Contributions
Conceptualization, C.-Y.H; K.-C.C; Y.-C.W.; S.-C.C; S.-L.C. Methodology, C.-Y.H; S.-L.C. Validation, C.-Y.H; S.-L.C. Data curation, C.-Y.H; S.-L.C. Writing—original draft preparation, C.-Y.H; S.-L.C. Writing—review and editing, S.-L.C. Visualization, C.-Y.H; K.-C.C; S.-C.C; S.-L.C. Supervision, C.-Y.H; Y.-C.W.; S.-L.C. Project administration, C.-Y.H; S.-C.C; S.-L.C. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.