
Abstract
We report resolution of right-sided pulsatile tinnitus in a 44-year-old male who underwent stapedectomy for fenestral otosclerosis. Initial workup revealed a mixed hearing loss and absent stapedial reflexes consistent with ossicular fixation. CT angiography demonstrated near complete stenosis of the left-sided transverse and sigmoid sinuses and dominant contralateral venous outflow. We hypothesized that the dominant right cerebral venous outflow tract created turbulent flow that was conducted to cochlea. Successful stapedectomy was performed, and the pulsatile tinnitus resolved. This case report demonstrates evidence that the sound of turbulent blood flow can be conducted through bone and an instance where the perception of vascular tinnitus was eliminated with stapedectomy.
Introduction
Tinnitus is a common otologic symptom affecting 30% of the population worldwide. 1 Approximately 10% of these patients complain of pulsatile tinnitus (PT), defined as the perception of somatic sounds synchronized with the pulse in the absence of an external acoustic stimulus. 2 PT secondary to vascular etiologies results from a disruption in laminar flow causing local turbulence that may be perceived by the listener. Common vascular etiologies of PT include sigmoid sinus and jugular bulb diverticulae/stenosis, 4 intra-sigmoid arachnoid granulations, dural fistulae, arterio-venous malformations, and vessel dissections.
Vascular etiologies may be further subdivided into venous or arterial. Venous tinnitus is usually low-pitched and is often perceived to be right-sided more frequently than left-sided due to right-sided venous outflow dominance in 70% to 80% of cases. 3 Arterial tinnitus is usually high-pitched on auscultation. Differentiation helps to identify cases that may be amenable to intravascular stenting or surgical treatment.
The mechanism of sound perception in cases of PT has yet to be clearly described. Exposed vascular walls are thought to produce sound pressure waves that radiate through the mastoid cavity, producing movement of the tympanic membrane via air conduction. Thus, intravascular and surgical treatments are focused on the correction of the vascular abnormality and dampening exposed areas of the venous sinus system via stenting, occlusion of offending diverticulae, or resurfacing.5,6 Herein, we describe an unusual case of PT that was caused by sound conducted directly through the temporal bone to the cochlea that became perceptible due to the development of mixed hearing loss secondary to otosclerosis.
Case Report
A 44-year-old male physician presented with a two-month history of constant, right-sided PT, without any other otologic complaints. He denied any history of hearing loss, prior otologic operations, head/ear trauma, or focal neurologic symptoms. Head and neck examination revealed decreased hearing in the right earwith bone conduction greater than air conduction and Weber tuning fork testing lateralizing to the right ear. There were no peri-auricular or cranial bruits. PT did not alter in intensity with position change or digital pressure applied to either internal jugular vein in either sitting or supine positions.
Audiometric testing revealed right-sided mixed hearing loss, a speech reception threshold of 40 dB, 100% word recognition at 80 dB HTL with 50 dB of masking in the left ear, and absent stapedial reflexes ipsilaterally and contralaterally with the test probe in the right ear. The contralateral ear was found to have mild high frequency sensorineural hearing loss (Figure 1A). Audiograms: (A) Preoperative audiogram demonstrating moderate, right-sided mixed hearing loss and (B) postoperative audiogram one month status post right stapedectomy demonstrating near complete closure of the preoperative air-bone gap.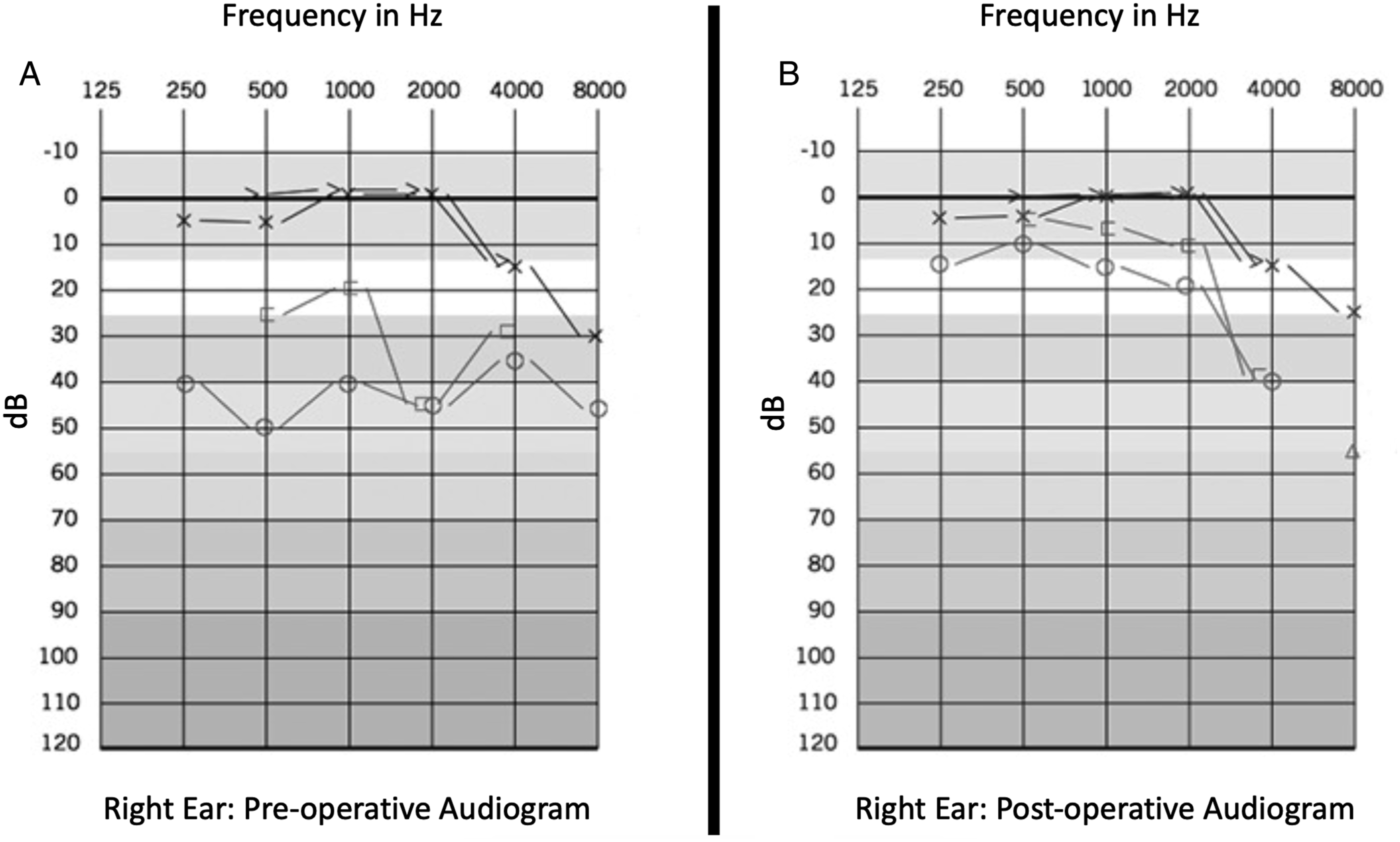
A tentative diagnosis of right otosclerosis was made. A CT scan of the temporal bones was consistent with fenestral otosclerosis. There was no evidence of superior semi-circular canal dehiscence.
A magnetic resonance imaging scan and magnetic resonance angiogram revealed dominant right transverse and sigmoid sinuses, no signal from the left transverse sinus, symmetric carotid and vertebral arteries, an intact circle-of-Willis, and normal courses of the carotid arteries. There was no evidence of dissection, fibromuscular dysplasia, vasculopathy, major branch occlusion, aneurysm, or stenosis. A magnetic resonance angiogram/venogram revealed a hypoplastic left transverse sinus consistent with a congenital variant (Figure 2). Magnetic resonance angiogram/venogram (MRA/MRV). MRA/MRV showing dominant right transverse and sigmoid sinuses (wide arrow) and a hypoplastic left transverse sinus without evidence of blood flow (thin arrow).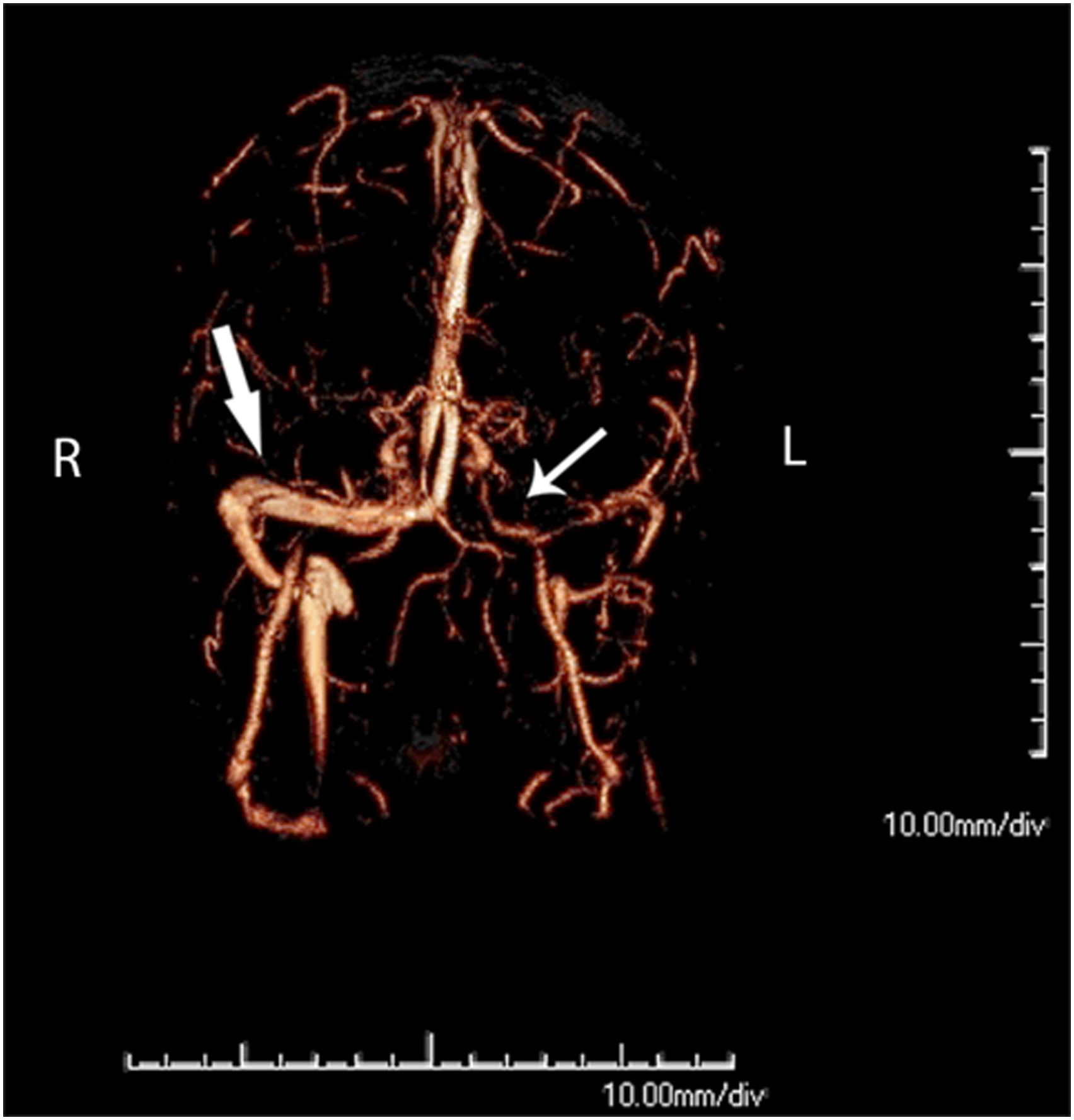
Discussion
An initial diagnosis was made of right stapedial otosclerosis with mixed hearing loss and congenital hypoplasia of the left sinuses of the dura mater. The majority of intracranial venous outflow was flowing through the right sinuses of the dura mater. The perception of right pulsatile tinnitus was secondary to sound that was being generated by turbulence secondary to high venous outflow through the right sinuses of the dura mater and was conducted to the right cochlea. A standard right-sided stapedectomy was performed using a 4.0 mm titanium Robinson cup stapes prosthesis over a vein graft. The procedure resulted in near complete closure of the preoperative air-bone gap and resolution of PT (Figure 1B).
Herein, we describe a case of PT conducted through the temporal bone to the cochlea, becoming perceptible to the patient due to progressive mixed hearing loss. We postulate that the patient had a lifetime of increased venous outflow through the right sinuses of the dura mater but was unable to perceive the transmitted sound until he slowly developed a mixed hearing loss secondary to fenestral otosclerosis. The congenital venous anomaly combined with a mixed hearing loss created an internal bone conduction Weber phenomenon resulting in perceptible PT.
Important to our treatment of this patient was knowledge that sound travels through the skull with 0 dB attenuation bilaterally and will lateralize to an ear with a mixed hearing loss secondary to stapedial otosclerosis. Complete resolution of audible PT was successfully achieved through stapedectomy. Without any changes to the vascular origin of the turbulent sound, the patient no longer perceived PT due to conversion of his mixed hearing loss to a mild conductive loss.
To our knowledge, this is the first case report of vascular tinnitus that has been improved by stapedectomy and underlines the need for comprehensive audiometric testing and imaging when evaluating PT.
Footnotes
Acknowledgments
We thank the patient for granting permission to publish this information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for open access was provided by the Department of Otolaryngology-Head & Neck Surgery, Wake Forest School of Medicine, Medical Center Blvd., Winston-Salem, NC 27157, USA.
Statement of Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Data Availability
No new data were created or analyzed in this study. Data sharing is not applicable to this article.