
Abstract
Sigmoid sinus diverticula are relatively rare but typically cause pulsatile tinnitus (PT) in the involved ear. Occasionally, symptoms produced by blood flowing through the diverticulum are severe enough to necessitate recontouring the sigmoid sinus. Recently, a 59-year-old female was evaluated after years of worsening unilateral PT. CT angiography identified a 5 mm sigmoid sinus diverticulum near the sinodural angle. Given the severity of symptoms, the patient’s diverticulum was surgically decompressed and recontoured using hydroxyapatite bone cement.
Significance Statement
Sigmoid sinus diverticula are relatively rare but typically cause pulsatile tinnitus (PT) in the involved ear. Occasionally, symptoms produced by blood flowing through the diverticulum are severe enough to necessitate recontouring the sigmoid sinus. Recently, a 59-year-old female was evaluated after years of worsening unilateral PT. CT angiography identified a 5 mm sigmoid sinus diverticulum near the sinodural angle. Given the severity of symptoms, the patient’s diverticulum was surgically decompressed and recontoured using hydroxyapatite bone cement.
Introduction
Although tinnitus is a common complaint that may or may not have a discernible cause, workup for pulsatile tinnitus typically yields a distinct etiology that may require treatment. The pulsatile nature of the symptoms suggests vascular etiology, and common causes of pulsatile tinnitus include arteriosclerosis, arterial dissection, fibromuscular dysplasia, arteriovenous fistulae, vascular skull base tumor, or intracranial hypertension. 1 Sigmoid sinus defects are seen in 4–20% of patients with pulsatile tinnitus; however, there is some debate regarding appropriate management of sigmoid sinus diverticula given the rarity of these defects. 2
Case
A 59-year-old female patient presented with unilateral pulsatile tinnitus of her left ear which had progressively worsened over several years. The patient noted that her tinnitus improved when she placed firm pressure on the left side of her neck, and auscultation of the left jugulodigastric region demonstrated a bruit. Otherwise, the physical examination of her head and neck was unremarkable. Audiologic examination revealed normal hearing and type A tympanograms bilaterally. Acoustic reflexes were present on right, but absent on the left side. Microscopic exam of both tympanic membranes was normal.
Based on her symptoms of unilateral pulsatile tinnitus, the patient underwent a CT scan and CT angiography of the head and neck. The angiogram demonstrated a 5 mm diverticulum along the left sigmoid sinus (Figure 1). Based on the severity of the patient’s symptoms and the CT findings, the patient elected to undergo surgical intervention to minimize the diverticulum and recontour the sigmoid sinus in an attempt to decrease the turbulence within the sigmoid sinus. CT angiography of the patient’s head and neck revealed a 5 mm diverticulum of the left sigmoid sinus.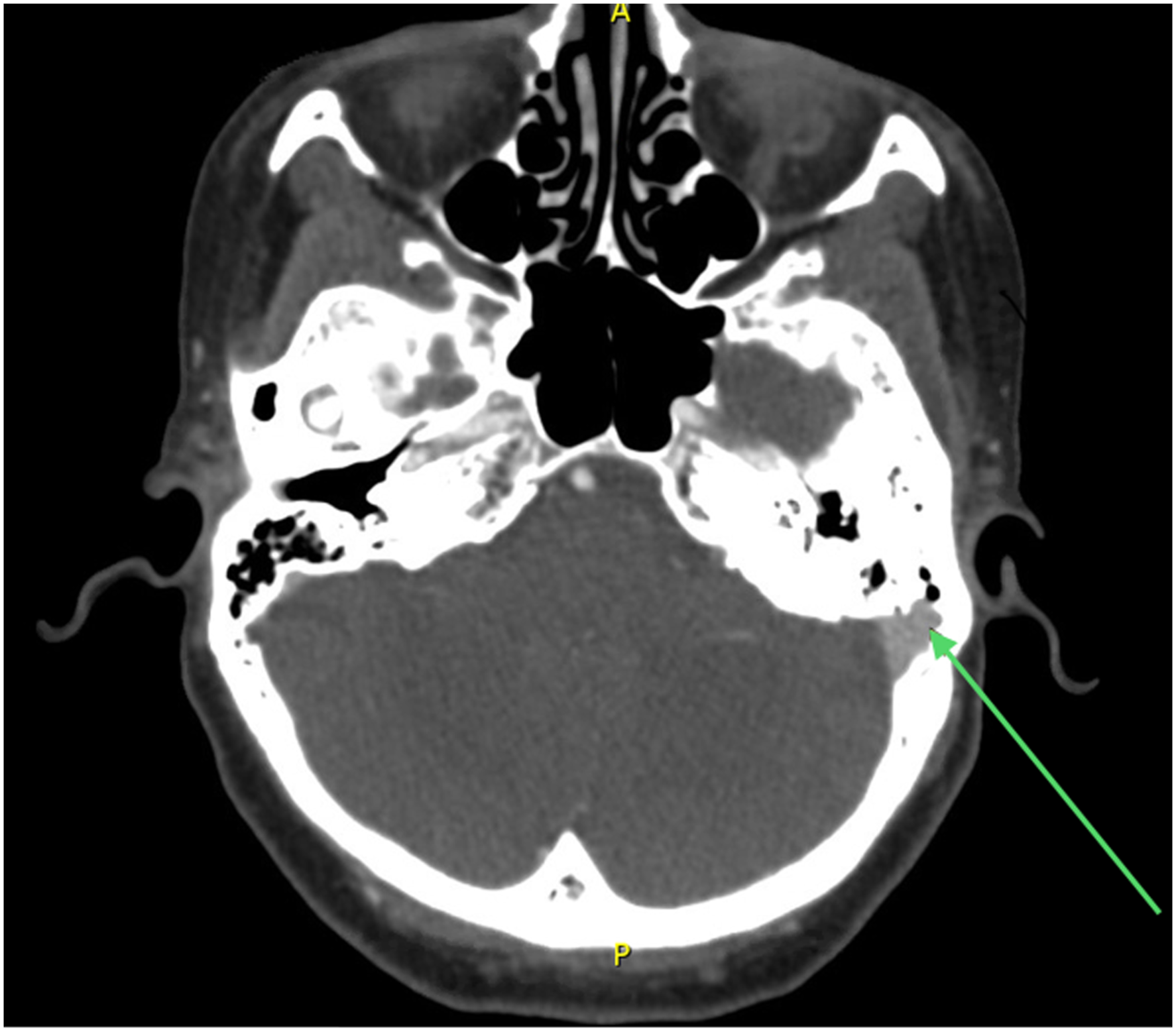
In April of 2021, the patient underwent a mastoidectomy with skeletonization of the sigmoid sinus. The diverticulum was located on the superior aspect of the sigmoid sinus near the sinodural angle. The bone overlying the diverticulum was carefully removed using fine diamond burrs. The wall of the diverticulum was quite thin, and the diverticulum appeared to be larger than the 5 mm size seen on preoperative imaging (Figure 2). Mastoidectomy revealed the sigmoid sinus defect, which was exposed with coarse and then fine diamond drilling prior to entry of the diverticulum.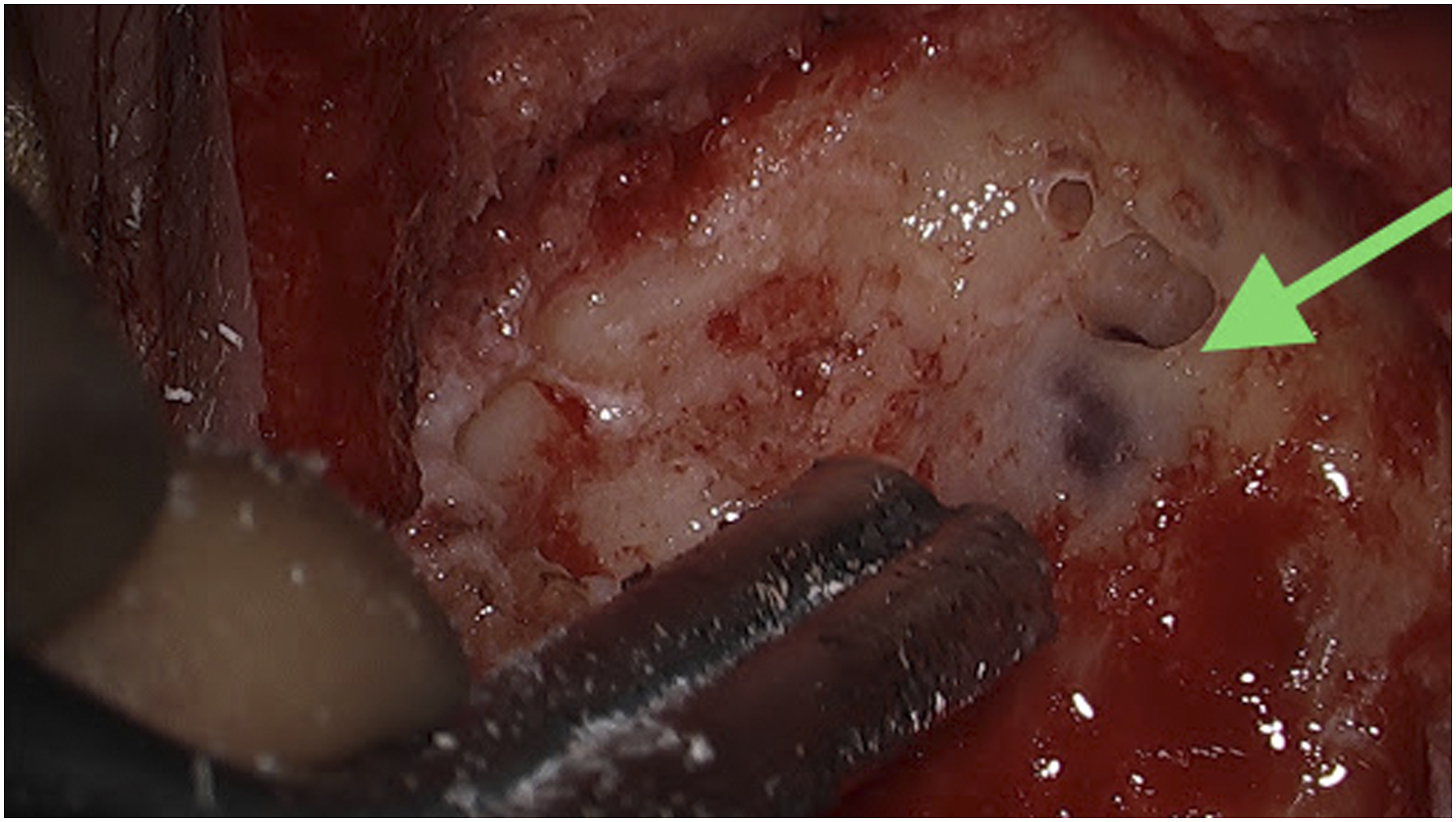
To shrink the diverticulum, the wall of the diverticulum was cauterized using bipolar cautery. Hemostasis was achieved using a combination of manual pressure, bipolar cautery, and Gelfoam. The diverticulum remnant was then compressed into the lumen of the sigmoid sinus and hydroxyapatite bone cement applied. The bone cement (Mimix) was allowed to set for approximately four minutes, reconstituting the normal bony wall surrounding the sigmoid sinus (Figure 3). The incision was closed, and a mastoid dressing applied. The patient experienced no complications and was discharged. Repair of the sigmoid sinus defect was performed with bone cement, which allowed for rigid recontouring of the mastoid.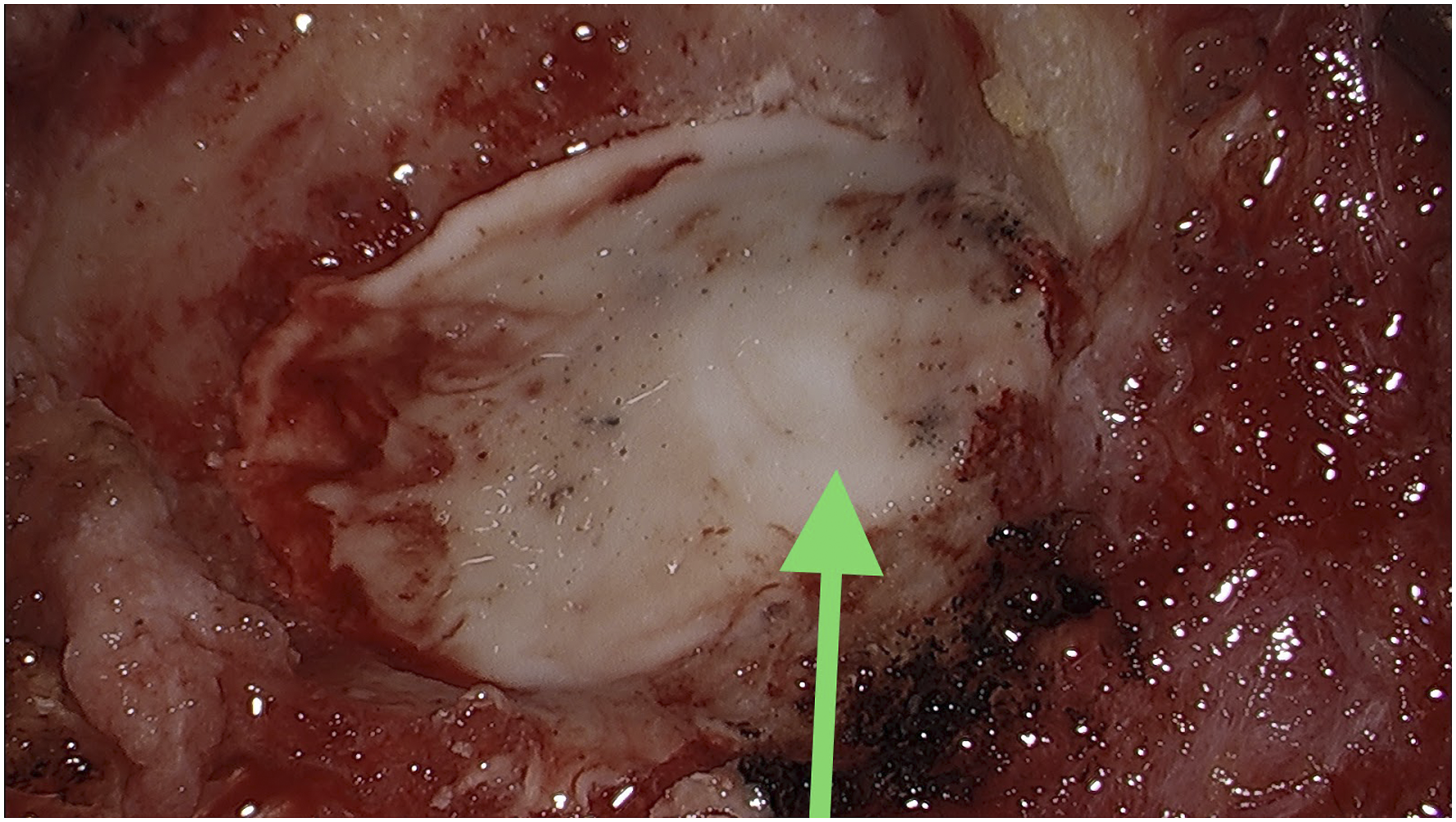
Three months postoperatively, the patient noted significant improvement in her left-sided pulsatile tinnitus, experiencing only mild symptoms upon exertion.
Discussion
Surgical intervention for sigmoid sinus diverticula involves revision and correction of the vascular defect. This may be done endovascularly or via open surgery with reconstruction.3,4 When performed in an open surgical manner, this is most commonly done with autologous temporalis fascial and bone chip grafting, but auricular cartilage or bone cement can also be used. 2 For this patient, hydroxyapatite bone cement was selected as a material. Although it is not as commonly used, this material offers significant ease of manipulation intraoperatively and is durable and inflexible when dry. As a result, it is a good option for reestablishment of the temporal bone structure in the area of the previous defect. 5
This patient’s presentation represents a rather unpleasant constellation of symptoms that was significantly impacting her quality of life. Although her neck pain had previously been treated surgically with some initial success, the worsening of her pain and eventual refractoriness necessitated further workup. The additional symptoms of unilateral pulsatile tinnitus and dizziness indicated the need for otolaryngologic examination. ENT workup revealed the uncommon etiology of sigmoid sinus diverticulum which caused this patient’s symptoms. Although this vascular lesion is particularly rare, the utility of vascular imaging for pulsatile tinnitus is evident. This allowed for appropriate surgical planning and execution, leading to the patient’s positive outcome.
The use of bone cement to reconstruct the sigmoid sinus wall and repair the defect is a rather novel technique that has several advantages, most importantly of which is the successful surgical management and resolution of this patient’s symptoms.
Conclusion
Sigmoid sinus diverticula are rare; however, when present, they can result in substantial unilateral pulsatile tinnitus. Shrinking the diverticulum using bipolar cautery and then recontouring the bony wall surrounding the sigmoid sinus with bone cement can markedly improve or eliminate the patient’s pulsatile tinnitus.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.