
Abstract
Introduction
Syphilis is a systemic bacterial infection caused by the spirochete Treponema pallidum. The sexually transmitted disease has a tropism for many organ systems and if allowed to progress, can cause complex clinical issues. The origin story behind syphilis remains a source of some controversy: while some historians believe it was firmly rotated in the “old world” (Europe, Asia, and Africa) others claim it was brought back from the Americas during the age of discovery. Regardless, syphilis has long been a menacing human pathogen and remains a pertinent global public health concern.1-3
Record keeping began in the 1940s with incidence of syphilis reaching a peak after WWII as a result of war demobilization. Great progress was made in controlling the infection through the discovery of penicillin. 3 Although the national rate of reported primary and secondary (P&S) syphilis cases was at an all-time low in 2000 at 2.1 cases per 100,000 population, there has been a resurgence of P&S syphilis in the U.S. with the rate increasing every year after 2001.3-5 In 2018, there was a 14.9% increase from the year before and more than five times the rate of 2000. 4
This sudden change in the epidemiology of syphilis can be traced to an increase in the number of sexual partners, decreased use of barrier methods of contraception due to a false sense of security that STIs are curable with current healthcare technology, and lack of knowledge regarding STIs.2,5,6 The men who have sex with men (MSM) population accounts for roughly two thirds of P&S syphilis cases and continues to increase, as seen by the 52% increase between the years 2014 and 2018. 4 However, in the last decade, cases among men who have sex with women (MSW) and women have increased substantially, accounting for 29.6% of cases in 2018. Between 2014 and 2018, a 172.7% increase in reported P&S syphilis was observed among women.
Syphilis can be transmitted through any close contact with a syphilitic lesion and vertically through pregnancy.2,7 The course of syphilis is separated into 3 stages: primary, secondary, and tertiary. 8 Head and neck mucosal manifestations of syphilis can be seen in all 3 stages. Most commonly they appear in the second stage, and up to 22% of all cases of secondary syphilis have some oral mucosal involvement. 9 Lesions can present in a variety of ways depending on the stage. The lesion of primary syphilis is known as a chancre which erupts at the site of inoculation. 1 There may be one lesion or multiple that appears initially as a papule-like lesion approximately 2–3 wk after inoculation and eventually ulcerates, producing a highly infectious chancre-ulcer that lasts up to 3–7 wk.4,7 Patients progress to the secondary stage 2–12 wk after the chancre appears. Disseminated lesions, often a nonpruritic rash on the trunk and extremities, and systemic symptoms of malaise, weight loss, and fevers indicate progression to the second stage of infection. 1 Tertiary syphilis presents after many years in the setting of untreated syphilis and is separated into gummatous, neuro, and cardiovascular syphilis. 2 This literature review aims to better understand and characterize the manifestation of these various syphilitic lesions within the mucosal surfaces of the head and neck.
Patients and Methods
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines were utilized to best define the search strategy. 10 A systematic search of PubMed, EMBASE, and clinical trials database (clinicaltrials.gov) was conducted using an extensive search strategy comprised with the assistance of librarians at the University of South Florida. The other searches were tailored for the individual databases.
Study titles and abstracts were initially screened for relevance independently by two authors. This yielded a timeline of literature dating from 1950 to 2022. All duplicate studies or manuscripts deemed not relevant to the above inclusion criteria by either author was excluded at this point. Conflicts between reviewers were resolved by consensus. Full text analysis was next conducted on manuscripts selected by either of the independent reviews. We endeavored to include all published case reports and series identified throughout the search. Our inclusion criteria for articles consisted of (1) original English language manuscripts published in peer reviewed journals available from database inception, (2) documented diagnoses of syphilis, and (3) documented involvement of the areas of interest (oral cavity, oropharynx, larynx, etc.).
Once manuscripts were chosen, data from individual cases were extracted and populated on a pre-coded data set. The study had three main focuses: describe the lesions, document the anatomical sites of these lesions, and assess the stage. For each study included, the following data of interest was collected: author, year of publication, number of cases, patient sex and age, lesion type, lesion site, extra-genital and extra-oral manifestations, specific diagnostic testing, stage of syphilis, HIV status, and treatment given. Cases were excluded if this data was not appropriately documented. Descriptive statistical assessment was completed on the data.
Oral mucosal manifestations were categorized into 6 distinct lesion types based on literature: chancre-ulcer, leukoplakia, mucosal patch, condyloma, tissue hypertrophy, and gumma. Chancre-ulcer is often described as a well-circumscribed painless ulcer. Mucosal patches are typically slightly raised plaques covered with a grayish white pseudomembrane, while leukoplakia is a homogenous white patch firmly attached to the mucous membrane. It was noted that differentiation between describing lesions as “ulceration” and “mucosal plaques/patches” was seldom made in literature. Condyloma is described as gray or white, moist, warty, verrucous papules, or plaques. Tissue hypertrophy is defined based on pathology from biopsy. Gummas are granulomatous lesions formed by a necrotic coagulated center and associated with small-vessel obliterative endarteritis.
Results
Cohort Overview
The comprehensive search result is displayed in Figure 1. A total of 143 manuscripts were included in the literature review.5,7,11-50,51-100,101-151 From these, data on 236 individual patients were extracted. The mean age of patients in this cohort was 40.6 y with a median of 40 y. Men comprised of 75.4% (n = 178) and women made up 24.5% (n = 58) of the group. PRISMA flow chart illustrating the article selection process. Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement outlining stages of systematic search and abstract screening.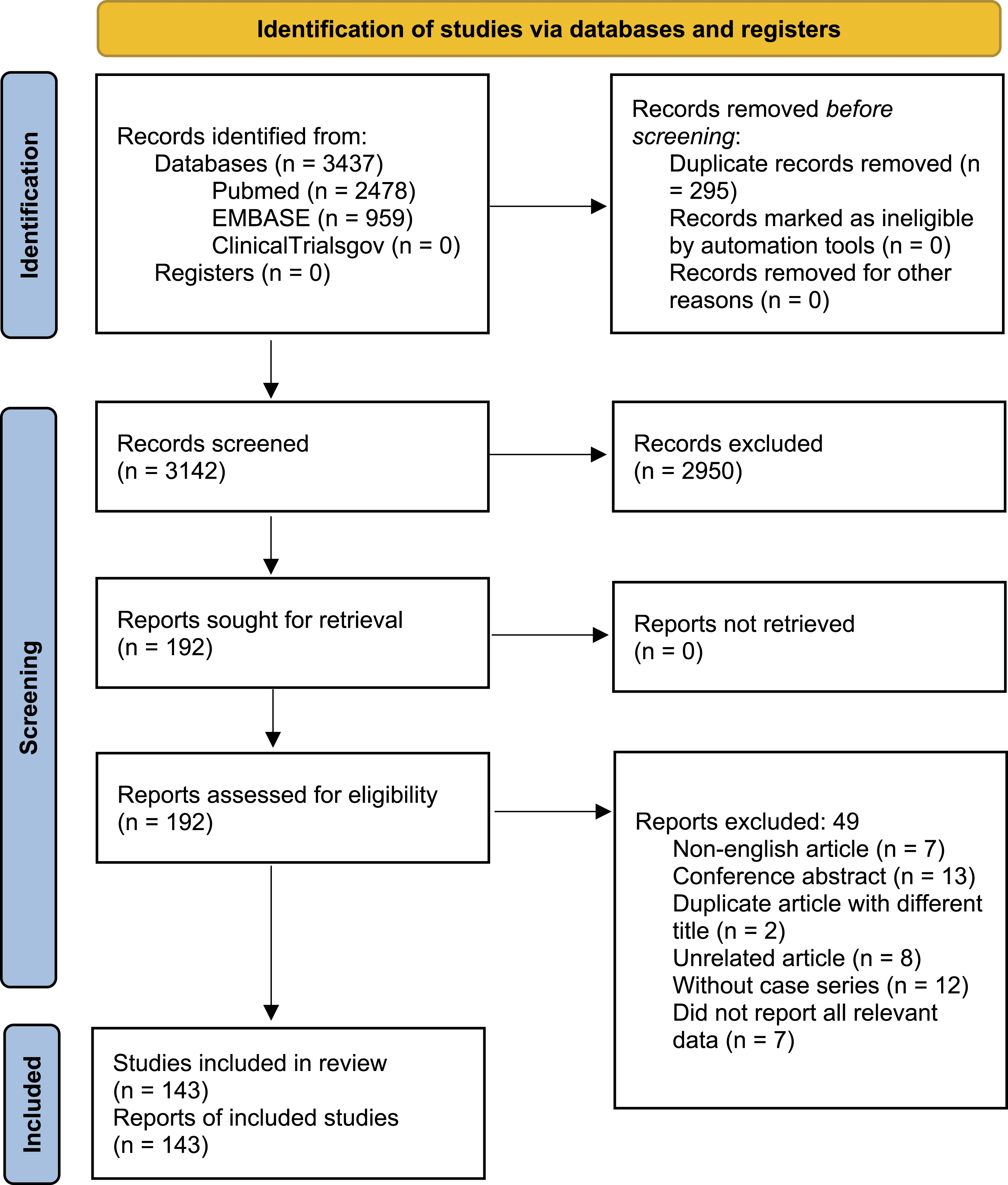
The majority of patients, 61.9% (n = 146) were in the secondary phase when presenting to a physician with a mucosal head & neck lesion. Fewer patients presented in primary and tertiary disease, at 19.5% (n = 46) and 8.1% (n = 19), respectively.
Primary Syphilis
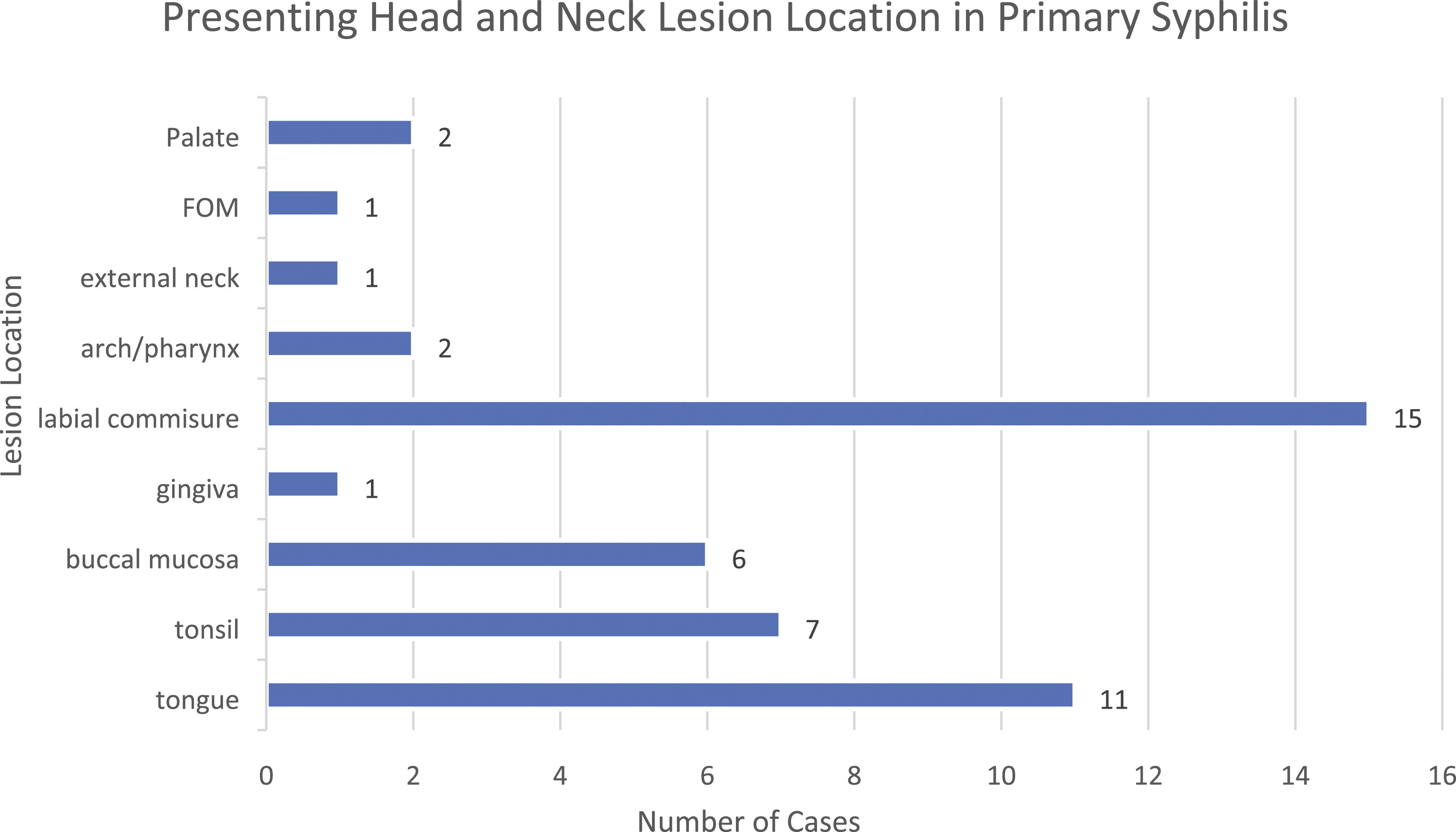
Of the 46 patients with primary syphilis, 87% (n = 40) presented with the classic ulcer-chancre. Many of the other various lesions did arise in low numbers including leukoplakia (n = 2), mucosal patches (n = 2), gumma (n = 1), and tissue hypertrophy (n = 1) (Figure 2). The most common anatomic localization of these lesions was the labial commissure (n = 15, 32.6%) and tongue (n = 11, 23.9%). Lesions also commonly arise in the tonsil (n = 7, 15.2%) and buccal mucosa (n = 6, 13%). Other less common locations of primary syphilis lesions were the hard palate, nonspecific palate, gingiva, pharynx, external neck, and floor of mouth (Figure 3). Presenting lesion in primary syphilis. Breakdown of presenting lesion type in patients diagnosed with primary stage syphilis. Presenting location in primary syphilis. Breakdown of presenting lesion location in patients diagnosed with primary stage syphilis.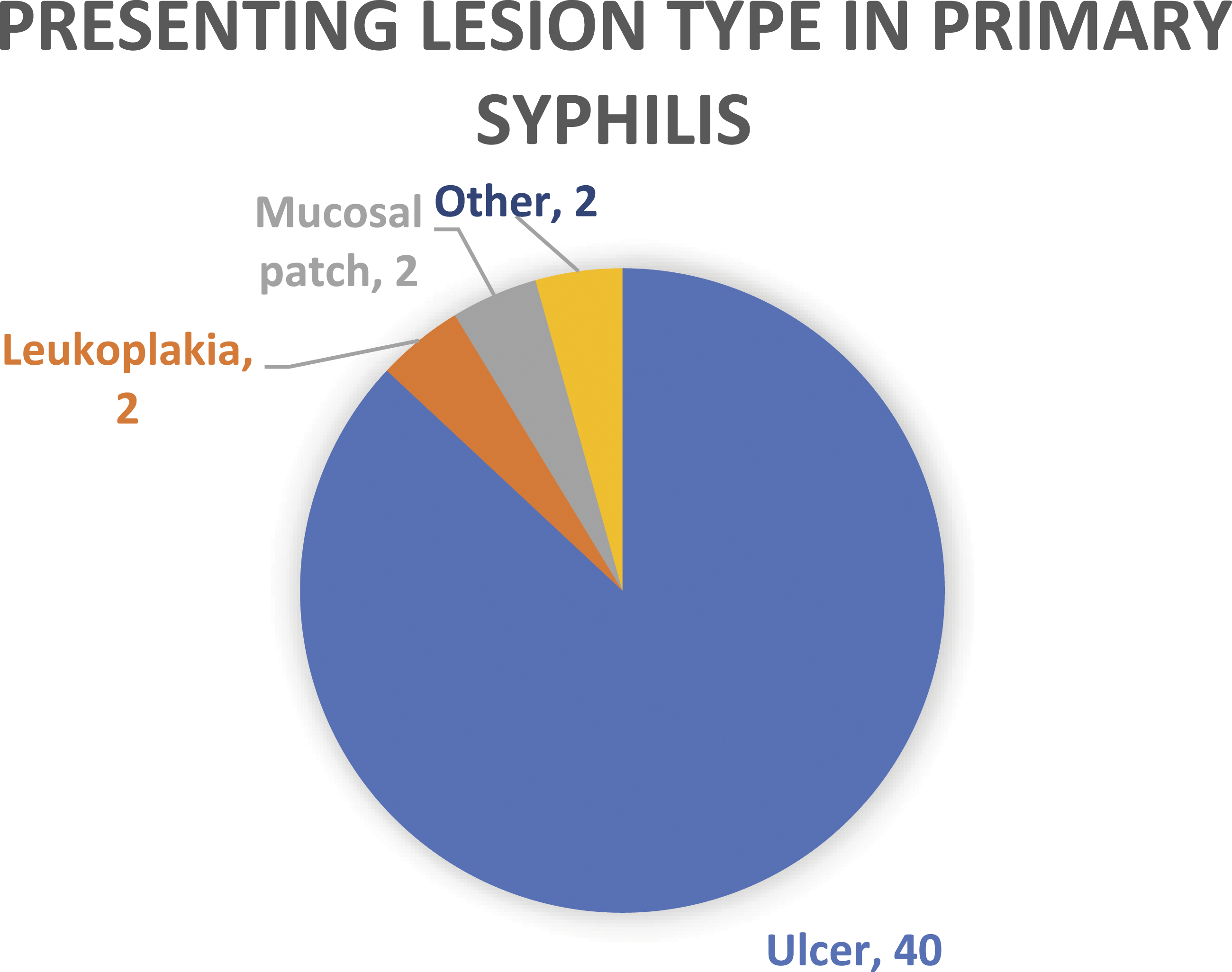
Secondary Syphilis
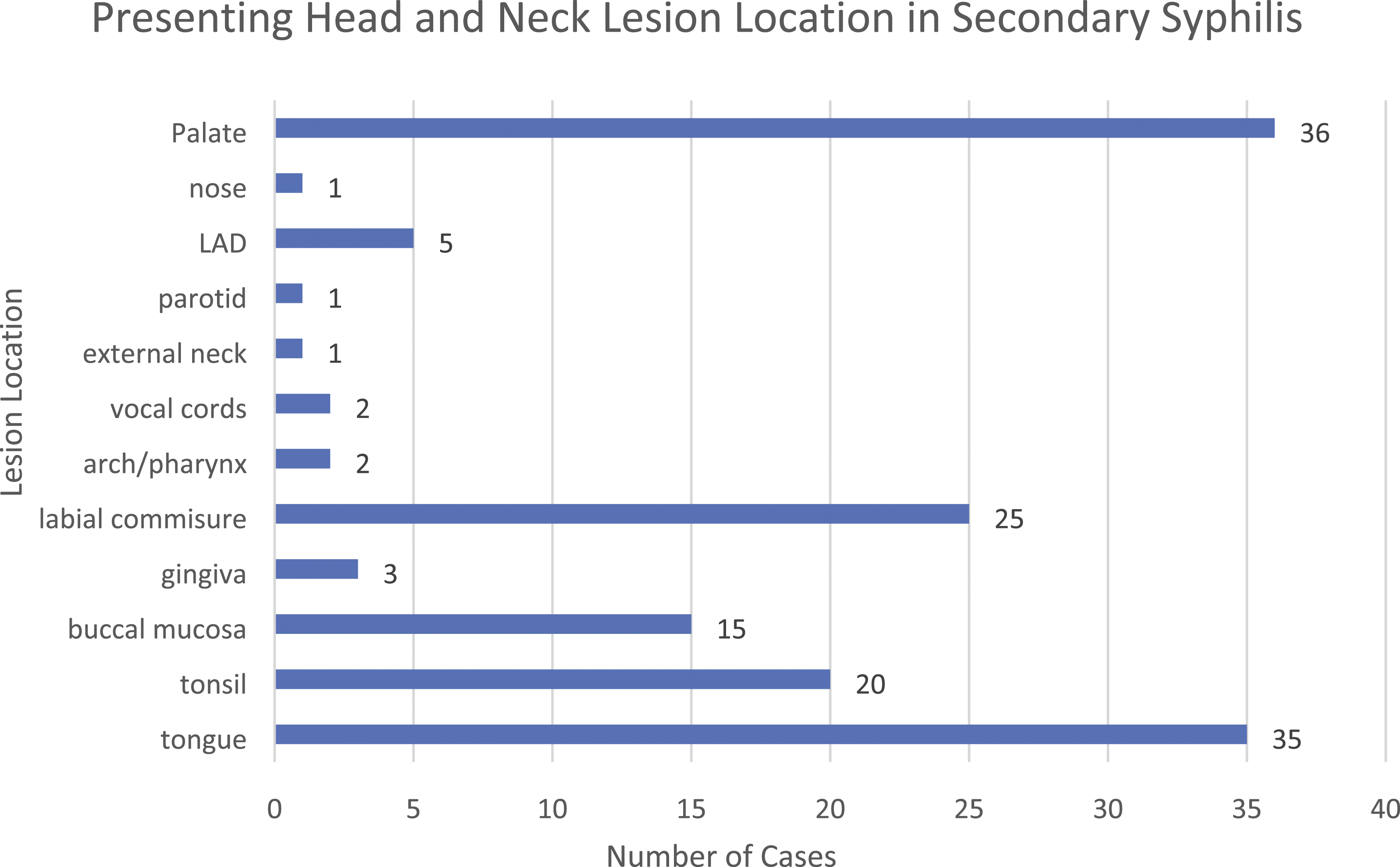
Of the 141 patients with secondary syphilis, 57% (n = 81) presented with the classic ulcer-chancre. The second most common lesion type was the mucosal patch (n = 32, 22.7%). Leukoplakia and tissue hypertrophy each accounted for 7.8% of cases (n = 11), while condyloma (n = 5) and gumma (n = 1) were seen less frequently (Figure 4). The most common anatomic location of these lesions was the tongue (n = 35, 23.9%) and labial commissure (n = 25, 17.1%). Lesions also commonly arise in the tonsils (n = 20, 13.6%), hard palate (n = 16, 11%), and buccal mucosa (n = 15, 10.3%). When hard, soft, and nonspecific palatal lesions are grouped together, this becomes the most common location of presentation (n = 36, 24.7%). Lymphadenopathy (LAD) is rarely seen (n = 5, 3.4%), with gingival, pharynx, vocal cord, external neck, parotid, and nasal lesions making up the remainder of presentations (Figure 5). Presenting lesion in secondary syphilis. Breakdown of presenting lesion type in patients diagnosed with secondary stage syphilis. Presenting location in secondary syphilis. Breakdown of presenting lesion location in patients diagnosed with secondary stage syphilis.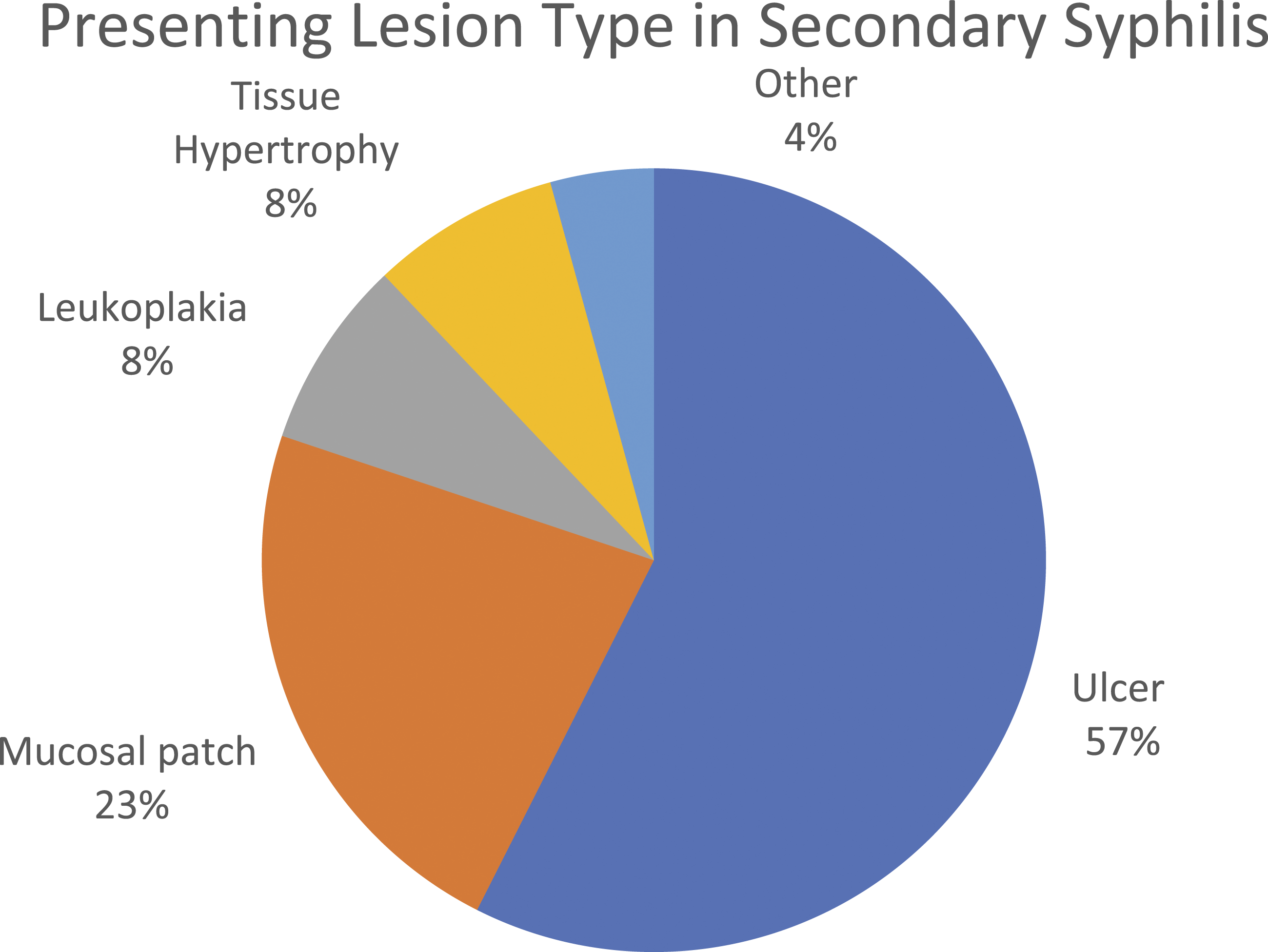
Tertiary Syphilis
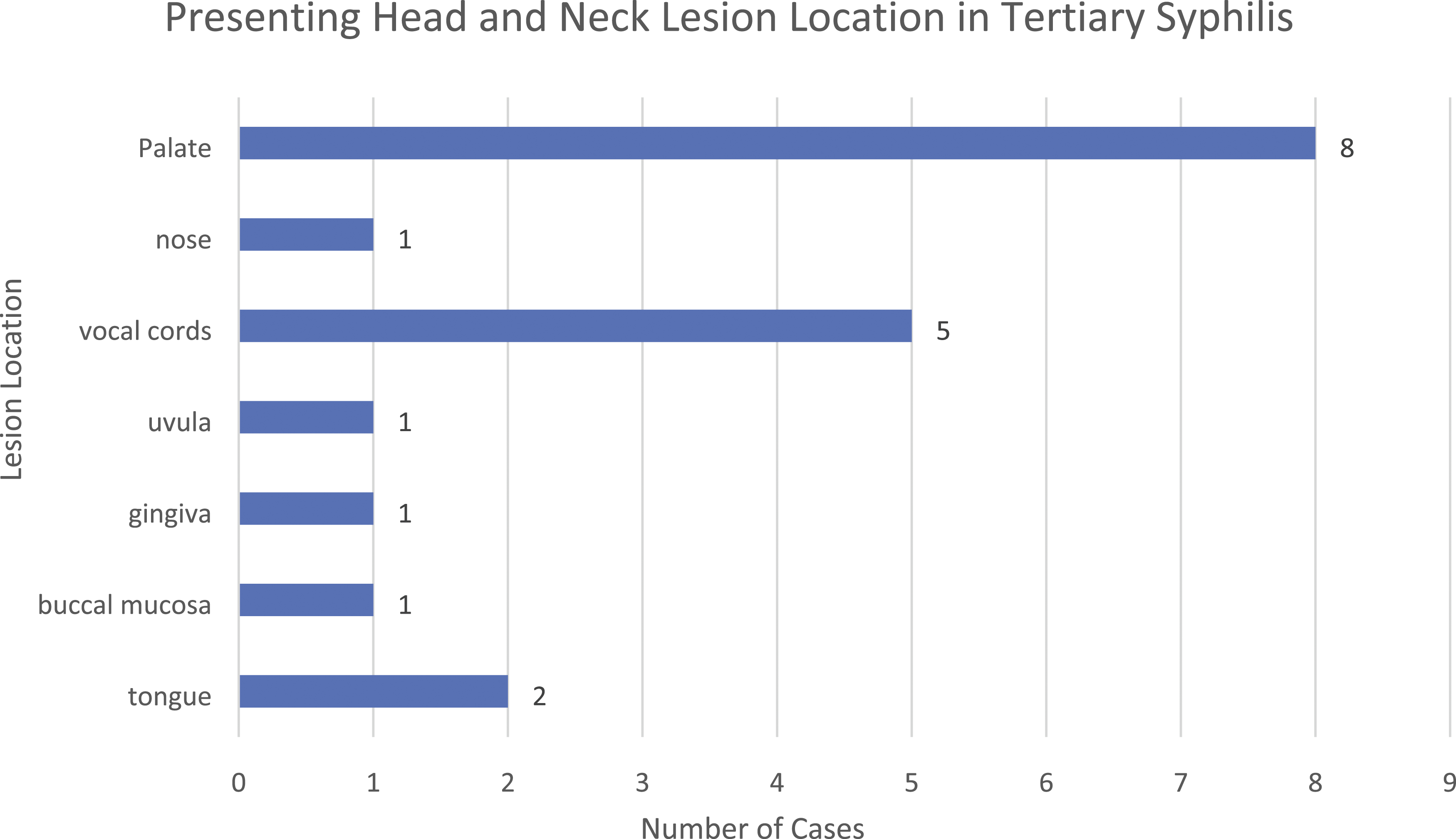
Of the 17 patients with tertiary syphilis, 76.5% (n = 13) presented with gumma. 3 patients (17.6%) presented with ulcer-chancre lesions, while a single patient presented with leukoplakia (Figure 6). Palatal lesions constituted 42.1% of tertiary syphilis lesions (n = 8), while vocal cord lesions (n = 5) made up 26.3% of cases. Tongue, nasal, buccal mucosa, uvula, and gingival lesions made up the remainder of presentations (Figure 7). Presenting lesion in tertiary syphilis. Breakdown of presenting lesion type in patients diagnosed with tertiary stage syphilis. Presenting location in tertiary syphilis. Breakdown of presenting lesion location in patients diagnosed with tertiary stage syphilis.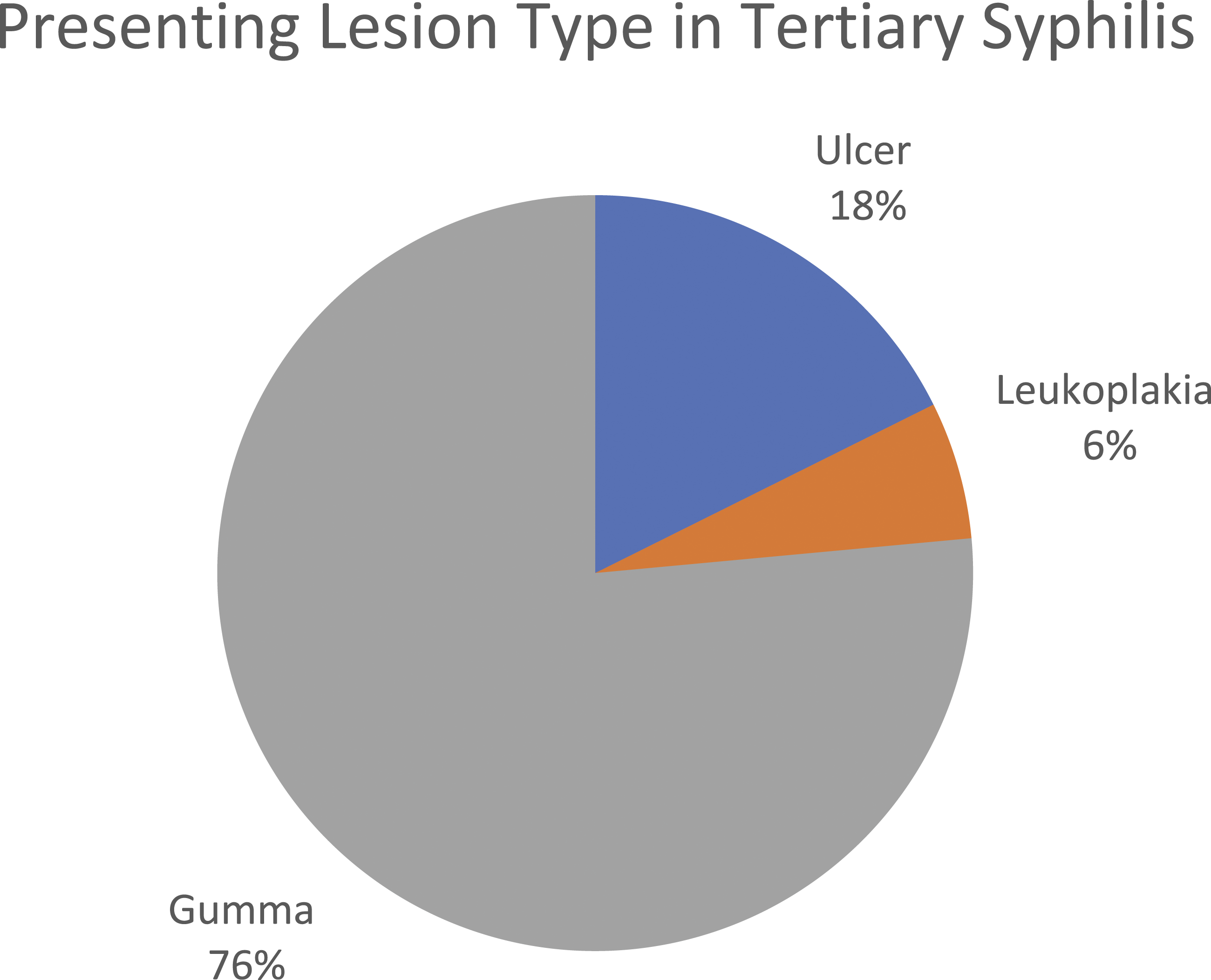
HIV Population
16.9% (n = 26) of patients were comorbidly infected with HIV and syphilis. Within the HIV population, 69.2% (n = 18) were in the secondary stage. Of the patients with HIV, 57.7% (n = 15) experienced non-oral extra-genital manifestations. Of these symptomatic patients, 26.7% (n = 4) had unusual findings including concomitant viral exanthems, ocular involvement, and neurosyphilis.
Diagnosis and Treatment
Recorded testing yielded data indicating that 87.7% (n = 207) of patients were VDRL/RPR positive and 70.3% (n = 166) were FTabs/TPHA positive. Biopsies were performed on 65.2% of patients. The majority of patients, at 69.5% (n = 164), were treated with penicillin. A minority of patients were treated with doxycycline in 4.2% (n = 10) and amoxicillin in 3.8% (n = 9).
Discussion
Head and neck mucosal manifestations of syphilis pose a unique clinical challenge given the heterogenous impact of this disease in this region of the human body. By viewing this disease based on the stage of infection, differing clinical pictures emerge.
Primary Syphilis
Less than 20% of the patients identified in this review were diagnosed with primary syphilis. The initial stage of a syphilitic infection involves direct tissue invasion, and while T. pallidum is capable of directly entering through the non-keratinized oral mucosa, the majority of diagnosed primary syphilitic lesions remain to be in the genital and peri-anal areas, which are also characterized by decreased keratin distribution. 152 Primary syphilis presented as ulceration in almost 90% patients in our review. These lesions were most commonly on the lips and tongue but were also frequently seen on the buccal mucosa and tonsils, which is consistent with prior reports. 153
Secondary Syphilis
Over half of the patients identified by this review presented as secondary syphilis (n = 141, 60%), which is consistent with prior literature. 9 There is no formal explanation for the increased incidence of head and neck mucosal lesions with secondary syphilis compared to other stages, however, it is likely related to the systematic nature of this stage of the infection. T. pallidum spirochetes rapidly become systemic and invade the dermis and epidermis, promoting shedding of the bacterium and further infections. 152 The nature of this process is likely responsible for the various manifestations of syphilis and helps to explain its title as “the great imitator.” 8
Our review found the most common presenting lesion in secondary syphilis to be the classic chancre-ulcer lesion. This is counter to other literature that report mucous patches as the most common manifestation.40,49 However, Hook et al. defined mucous patches as “shallow, painless ulcerations on mucous membranes,” and the term “mucous patch” is likely interchanged with “ulceration” when located in the oral cavity. 1 When combined, chancre-ulcers and mucous patches constitute 80.1% of presentations of secondary syphilis in our review. Previous literature report secondary syphilis lesions occur most commonly on the lips, tongue, buccal mucosa, and palate, which we found consistent with our review.40,121,154 However, we found tonsillar lesions to be more commonly seen than previously documented.
Tertiary Syphilis
Only 8% of patients in our review were diagnosed with tertiary syphilis. Over 75% of these patients presented with gummata, which is consistent with prior reports.20,155 Gummata, a feature rarely seen in other stages of syphilis, are large, nontender nodular lesions with granulomas and large swaths of caseating necrosis found on biopsy. 156 Our review found these lesions most commonly in the palate and glottis. Interestingly, over 25% of these patients also complained of hoarseness and change in voice, with physical exam indicating vocal cord paralysis. This observation has been seen before, with one report noting grossly irregular vocal fold edges with keratotic and fibrinous changes. 73
Syphilis and HIV
Syphilis coinfection with HIV is well documented. According to the CDC, since the gradual increase in P&S syphilis incidence began in 2001, reported cases of P&S syphilis became significantly more characterized by a high rate of HIV coinfection. 5 This is especially true among MSM, with nearly 60% of P&S syphilis cases diagnosed in 2016 occurring in that population. 5 Likewise, current literature reports syphilis and HIV coinfection to be 47.0% for MSM, 10.7% for MSW, and 4.1% for women. 157 Despite this, our data reflected only 10.3% of patients (N = 22) were coinfected with HIV, which is a relatively low number compared to the CDCs rate of 38.5% of reported P&S syphilis cases coinfected with HIV in 2016. 158
Left untreated, syphilis facilitates the transmission and acquisition of HIV, and HIV coinfection may allow more rapid syphilitic disease progression.133,157,159 This relationship has been described as synergistic and may also result in aggressive and atypical syphilis sequelae.4,5 These patients often present with overlapping symptoms of different stages. In our review, 57.7% of coinfected patients also experienced extra-genital and extra-oral symptoms. In addition, coinfected patients experience more symptoms typically associated with secondary syphilis. 133 Syphilitic uveitis, which occurs more commonly in HIV coinfected people, may be the presenting symptom for these patients. 133 In our review, nearly 30% of the coinfected patients had unusual findings, 50% of which presented with uveitis.
Diagnosis and Treatment
A patient presenting to an otolaryngology clinic with an ulcerative lesion in the oral cavity or oropharynx will justifiably be worked up for malignancy, though this is also frequently the presentation of a patient with a mucosal syphilis lesion. Fortunately, syphilitic lesions have characteristic histopathological findings that would be discovered upon biopsy.
Three main histological findings have been associated with syphilitic pathology in the mucosa: gross and microscopic epithelial alterations, plasma cell infiltrate, and the presence of T. pallidum in the oral mucosa assessed by immunohistochemistry. 2 Primary syphilis specifically has ulcerated epithelium with superficial perivascular dermatitis, as well as spirochetes limited to the basal layer or dermal-epidermal junction.2,27 Secondary syphilis is characterized by psoriasiform or pseudo-epitheliomatous hyperplasia, and a dense superficial and deep inflammatory infiltrate with multiple spirochetes throughout the epithelium. 27 Gumma formation in tertiary stage presents with a central necrosis surrounded by a mixed infiltrate of plasma cells, lymphocytes, and histiocytes, with variable endarteritis and scarring.1,27
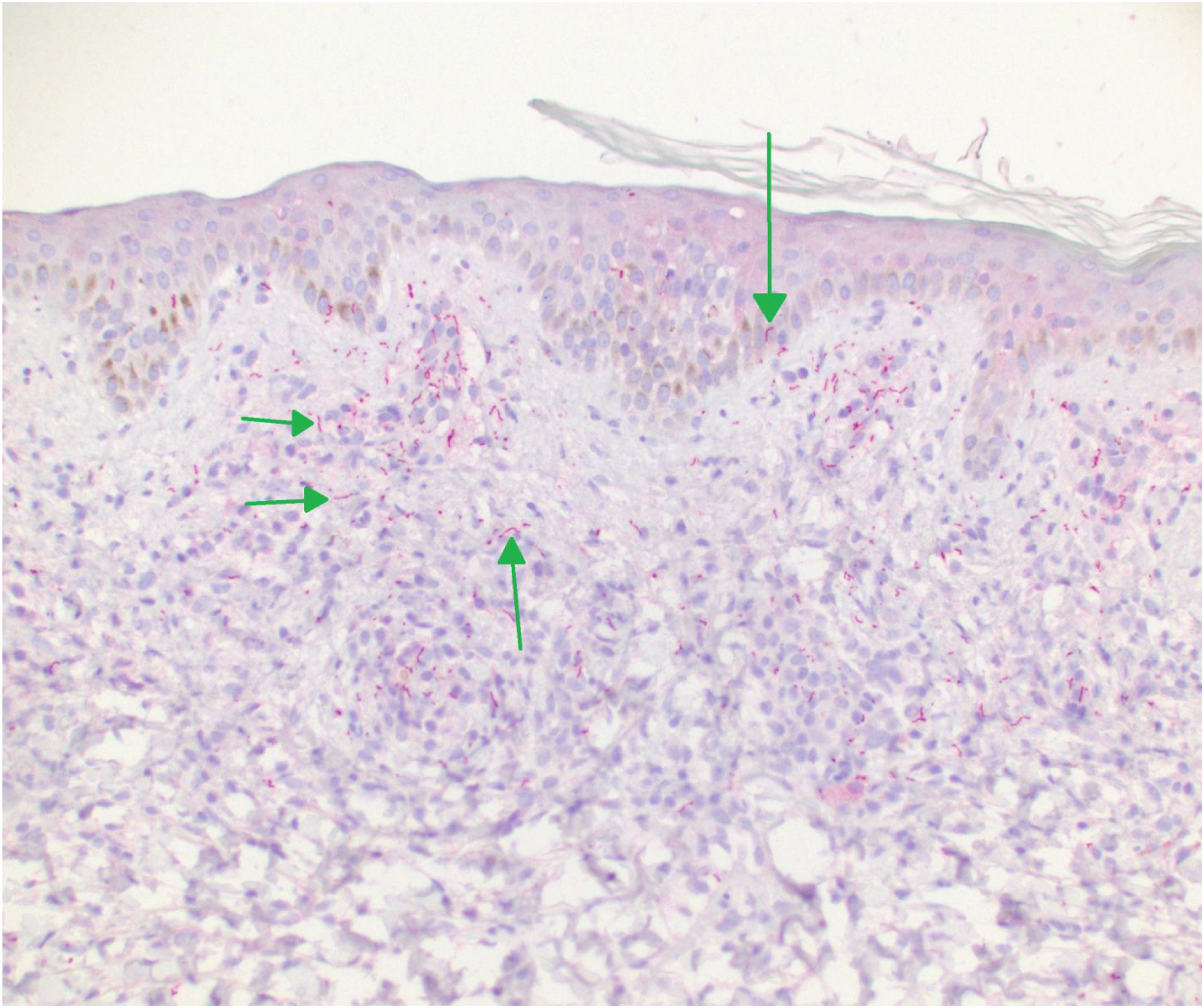
While a tissue biopsy of a suspicious syphilitic lesion should definitively rule out a malignancy, there are some further pathologic considerations in order to make the diagnosis of syphilis. Hematoxylin and eosin (H&E) staining will most typically show lymphoplasmacytic infiltrate (Figure 8), although this finding is not specific to syphilis. Notably, a positive treponema immunohistochemistry stain is the standard for tissue diagnosis of syphilis (Figure 9).
160
However, most institutions do not have this in-house and will not routinely perform this test. Additionally, the more widely available silver stain identifies spirochetes in general, which limits its utility in the mouth due to the presence of spirochetes in normal oral flora.
161
Any suspicion of syphilis should be relayed to the interpreting pathologist so the appropriate stains can be performed. This further reinforces the need for clinicians to be aware of syphilis, and to suspect it particularly when a biopsy returns with a lymphoplasmacytic infiltrate.
160
Treponemal hematoxylin and eosin (H&E) stain. Hematoxylin and eosin (H&E) stain of T. pallidum showing dense lymphoplasmacytic infiltration (infiltrate denoted with *) (×100 magnification). Treponemal immunohistochemistry stain. T. pallidum immunohistochemistry stain outlining corkscrew shaped organisms present in the epidermis and dermis appearing magenta in color (green arrows) (×200 magnification).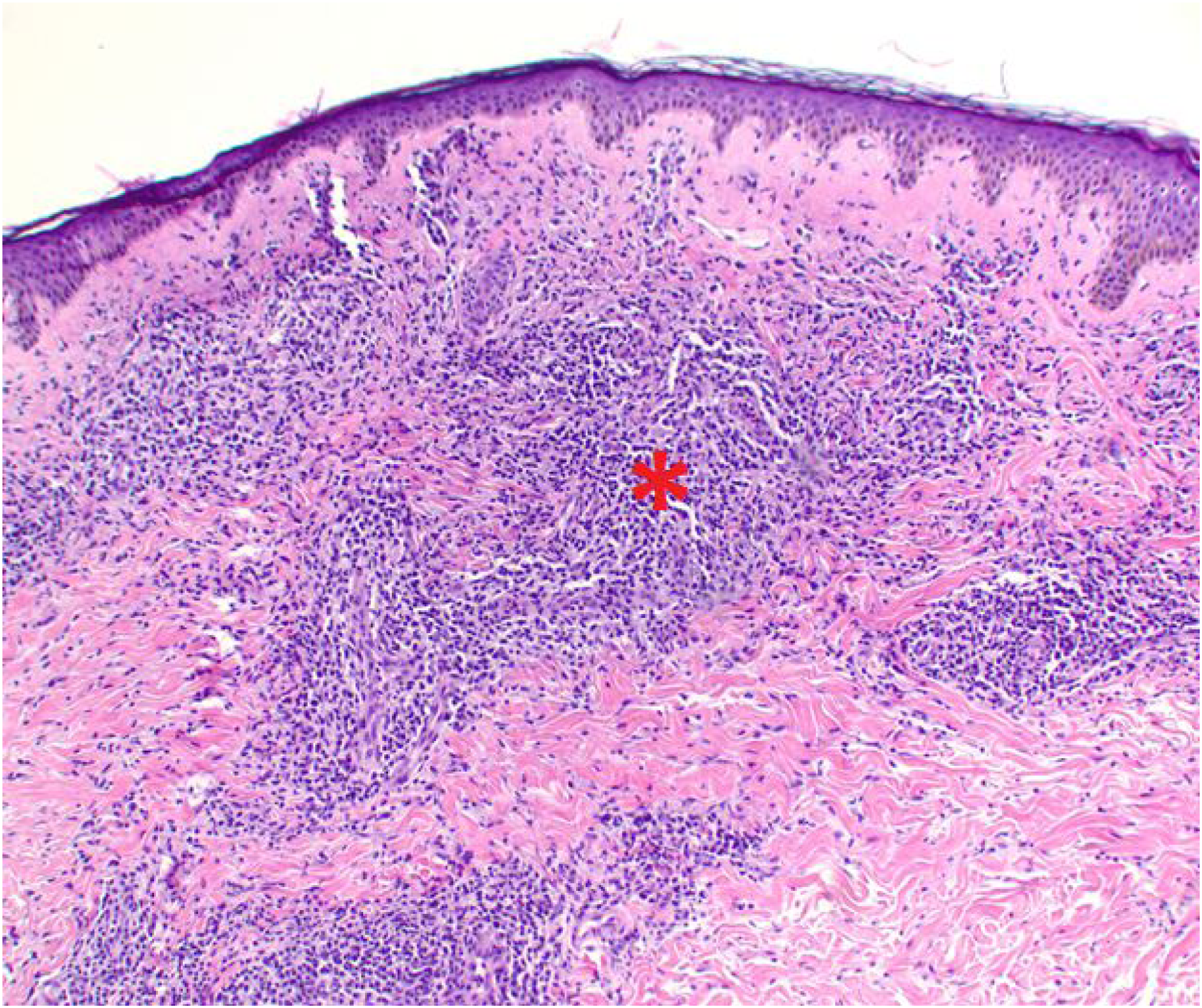
When syphilis is suspected, serology is the crux of diagnosis and has been developed significantly in the past few decades. Initial screening for syphilis has traditionally been non-treponemal testing such as the Venereal Disease Research Laboratory (VDRL) and Rapid Plasma Reagin (RPR) test.6,9,40 These tests detect antibodies to nonspecific treponemal antigens and have a sensitivity of 70–80% as a result specific testing should be followed which include T. pallidum hemagglutination assay (TPHA), fluorescent treponemal antibody absorbed assay (FTA.Abs), and microhemagglutination assay for Treponema pallidum (MHA-TP). 9
The majority of patients in our review were treated with penicillin, which remains the gold standard for the treatment of syphilis. A single injection of 2.4 million units of benzathine benzylpenicillin is the mainstay of treatment for P&S syphilis. 8 In cases of latent syphilis, this is continued weekly for 3 wk. 8 Patients with tertiary and neurosyphilis require higher doses administered intravenously every 4 h for 2 wk. 8 Those with penicillin sensitivities can be treated with doxycycline, tetracycline, or ceftriaxone. 8
Limitations
This review was limited by the inclusion of a large number of case reports and case series, which are likely to be susceptible to publication bias. Despite this, the incidence of each stage of syphilis, as well as presenting lesions, were generally consistent with prior published epidemiological reports. Notably, our data did report a low number of patients coinfected with HIV, at 10.3% compared to the CDCs reported rate of 38.5%. 159 This is likely due to the general lack of case reports of this patient population and/or misdiagnosis of these patients as their presenting clinical pictures may be inconsistent with syphilis. 133
Conclusion
Syphilis is an age-old disease that has historically been referred to as the “great imitator” due to its nonspecific systemic symptoms and signs. The disease can present itself during each stage in variable ways within the head and neck, which can be the only area of manifestation in certain situations. Ulcers within the oral cavity or oropharynx raise suspicion for malignancy but are simultaneously the most common mucosal presentation of primary and secondary syphilis. An understanding of how syphilis can affect the head and neck is crucial not only to otolaryngologists, but also to primary care physicians. Awareness of the lesions and their associated stage may help physicians maintain a higher index of suspicion, which is a prudent given the recent resurgence of syphilis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
No original data were generated for this review. All data are publicly available from the cited studies included in this review and are available from the corresponding author on reasonable request.