
Abstract
Introduction:
Head and Neck Cancer Awareness and Screening Programs (HNCASP) are popular community outreach events hosted by academic and community otolaryngology departments. However, long-term follow-up of participants is lacking.
Patients and Methods:
Participants of a HNCASP held at an academic cancer center prospectively filled out demographic and risk factor surveys followed by HNC screening examination. A phone interview was conducted for participants between 2012 and 2016 with suspicious findings to assess outcomes.
Results:
Participants were largely Caucasian, female, and had health insurance, reflecting the setting at an academic medical center. Despite this, there were 156 (16.8%) positive screenings; 47 of these completed follow up interviews. Twelve (1.1% of all participants) cancer cases were confirmed.
Discussion:
A significant proportion of HNCASP participants benefited from this screening opportunity. Education regarding HNC is the primary benefit and motivational factor for attendance of HNCASPs, although a significant subset of patients was identified that needed follow-up, and several cancers were detected.
Introduction
Cancer of the head and neck accounts for approximately 3% of all malignancies with about 53 000 cancers of the head and neck diagnosed in the US annually.1,2 Furthermore, the burden of head and neck cancer in the United States tends to weigh more heavily on those who face socioeconomic adversity. 3 Traditional risk factors for head and neck cancer include male gender, age greater than 50, tobacco use, alcohol consumption, sun exposure, and family history. Over the past 10 to 15 years, the incidence of head and neck cancer in the age-group younger than 50 years old has sharply increased. The rise in this cancer has been epidemiologically linked to human papilloma virus (HPV) infection of the oropharynx.4-7 Despite the availability of the HPV vaccine, the incidence of HPV-related oropharyngeal cancer continues to rise and is now equal to or has surpassed the incidence of HPV-related cervical cancer. 8 Despite these numbers, head and neck cancers generally do not receive the same level of public attention as other malignancies.
Cancer awareness and screening programs are a popular means of promoting cancer education and performing outreach to the community at large. Head and neck cancer does not always receive the same level of attention as other cancers in the lay press and popular consciousness; thus, Head and Neck Cancer Awareness and Screening Programs (HNCASP) have gained popularity as a relatively straightforward and low-cost means to educate the general population regarding this disease. Education is particularly important for HNC, given the prominent psychological and emotional aspects of this disease.9-14 Patients diagnosed with HNC tend to suffer substantially more psychiatric comorbidity when compared to cancers of other body regions. This is generally believed to be a result of the potentially devastating consequences of HNC progression and treatment sequelae upon the patient’s face and multiple bodily functions such as respiration, swallowing, and speech. Importantly, these psychological aspects can lead to the delay of diagnosis and treatment, subsequently lowering the chances of a favorable outcome.15,16 Thus, it is important to understand the factors which motivate one to seek or delay care concerning potential HNC.
Several other institutions that have sponsored HNCASP events have retrospectively shared their experiences17-25 screening the general public, underserved populations, and even participants of NASCAR sporting events. However, there is a significant gap in our knowledge regarding the utility of these programs in identifying pathology and the long-term follow-up that participants may receive. Furthermore, psychological factors surrounding patient willingness to seek care have been characterized in the clinical setting, they have yet to be explored in the context of HNCASP events. With this in mind, we conducted a study of participants at our institutional HNCASP, that for nearly 10 years has focused on education, cancer awareness, and providing an entry point into the healthcare system for patients with head and neck concerns. Over the course of 5 years, surveys were collected from participants regarding demographics, cancer risk factors, concerning symptoms, and motivations for attending the HNCASP. As a follow-up, phone interviews were conducted with participants with positive screening findings to determine the outcomes of the positive finding, if further medical evaluation had been performed, diagnosis, and treatment.
Patients and Methods
A retrospective review of prospectively collected data was performed regarding the HNCASP. This HNCASP was initiated in 2008 and provided a free day of screening for head and neck cancer to the local community annually. Beginning in 2013, a standardized intake survey was given to all participants in the HNCASP, collecting demographic data, medical history and risk factor assessment, and motivation for seeking screening. These responses, along with screening results, were collated into a single database over the years 2013 to 2016. This study was approved by our institutional review board.
Participants who received a positive screen for head and neck pathology and were instructed to follow-up for further medical assessment were contacted by phone in late 2016. Participants were asked about their ability to seek care, diagnosis obtained, treatment received, and resolution of their concern. Participation in this telephone survey was entirely voluntary (Figure 1). Data were analyzed using SPSS version 24. Descriptive statistics were performed for all variables.
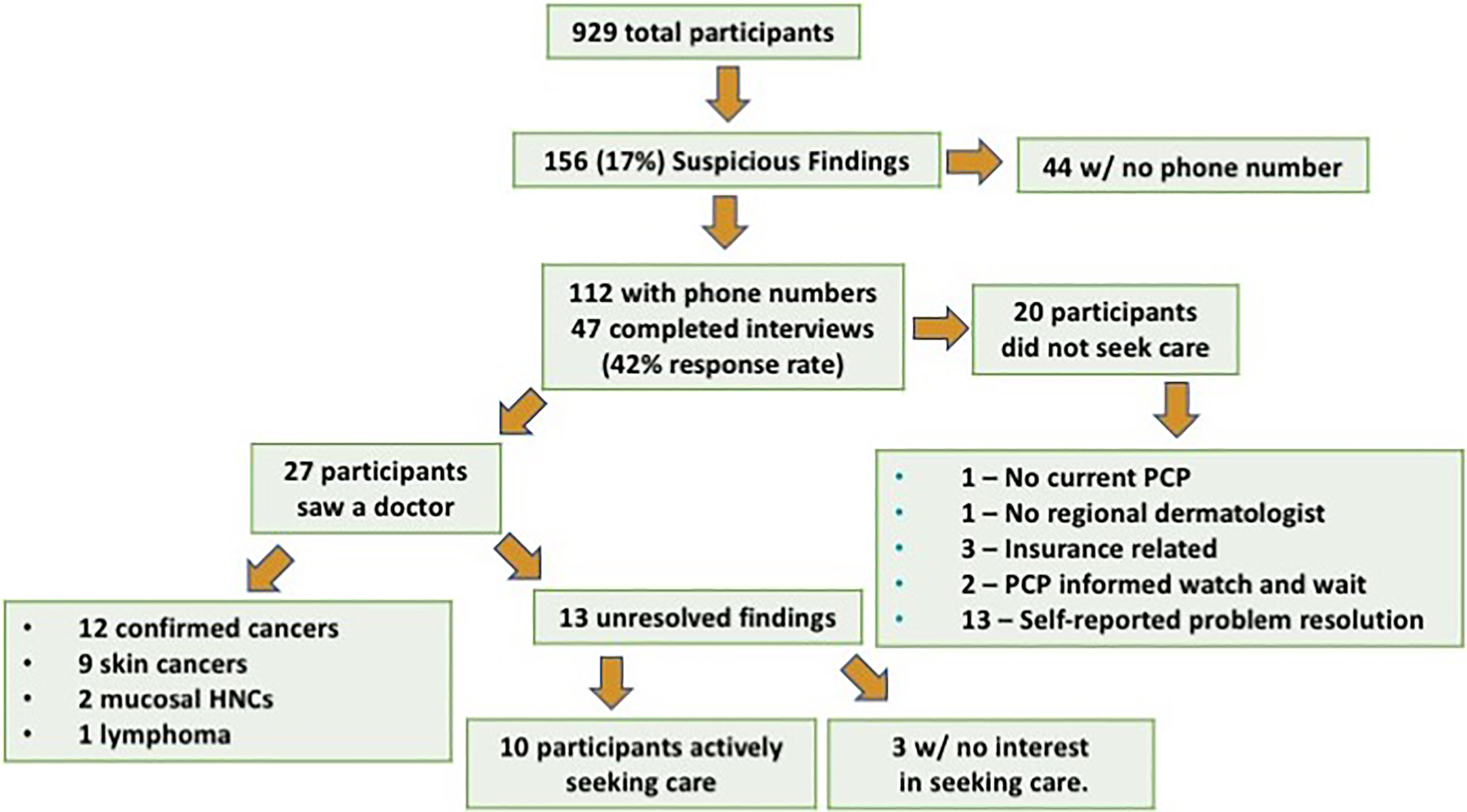
Study design and outcomes summary.
Results
Demographics and Risk Factors of Participants
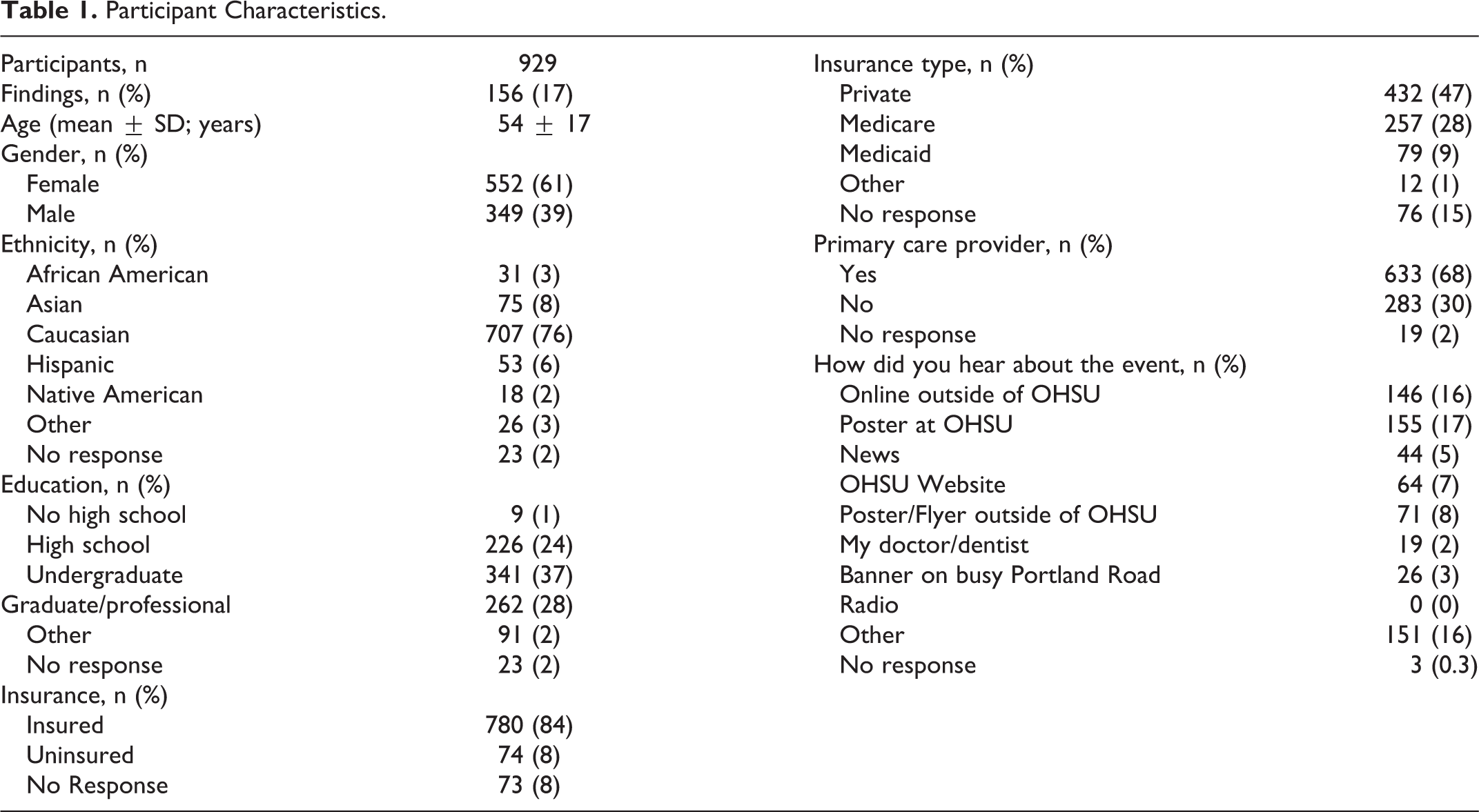
Of all, 929 participants attended HNCASP between 2013 and 2016. Demographic information for participants is shown in Table 1. Significantly, a majority of patients were Caucasian, had a college education or greater, had medical insurance, and had a primary care physician.
Participant Characteristics.
Most participants reported significant sun exposure (Table 2). The most common risk factor was regular alcohol use (2+ drinks/day, 58%), although current and former tobacco use was frequently reported. Self-reported radiation exposure (23%) was quite high; however, many of these responses included narratives such as “have received X-rays at the doctor’s office.” Notably, 15% of participants reported themselves or a current/recent partner being HPV-positive.
Participant Reported Risk Factors.
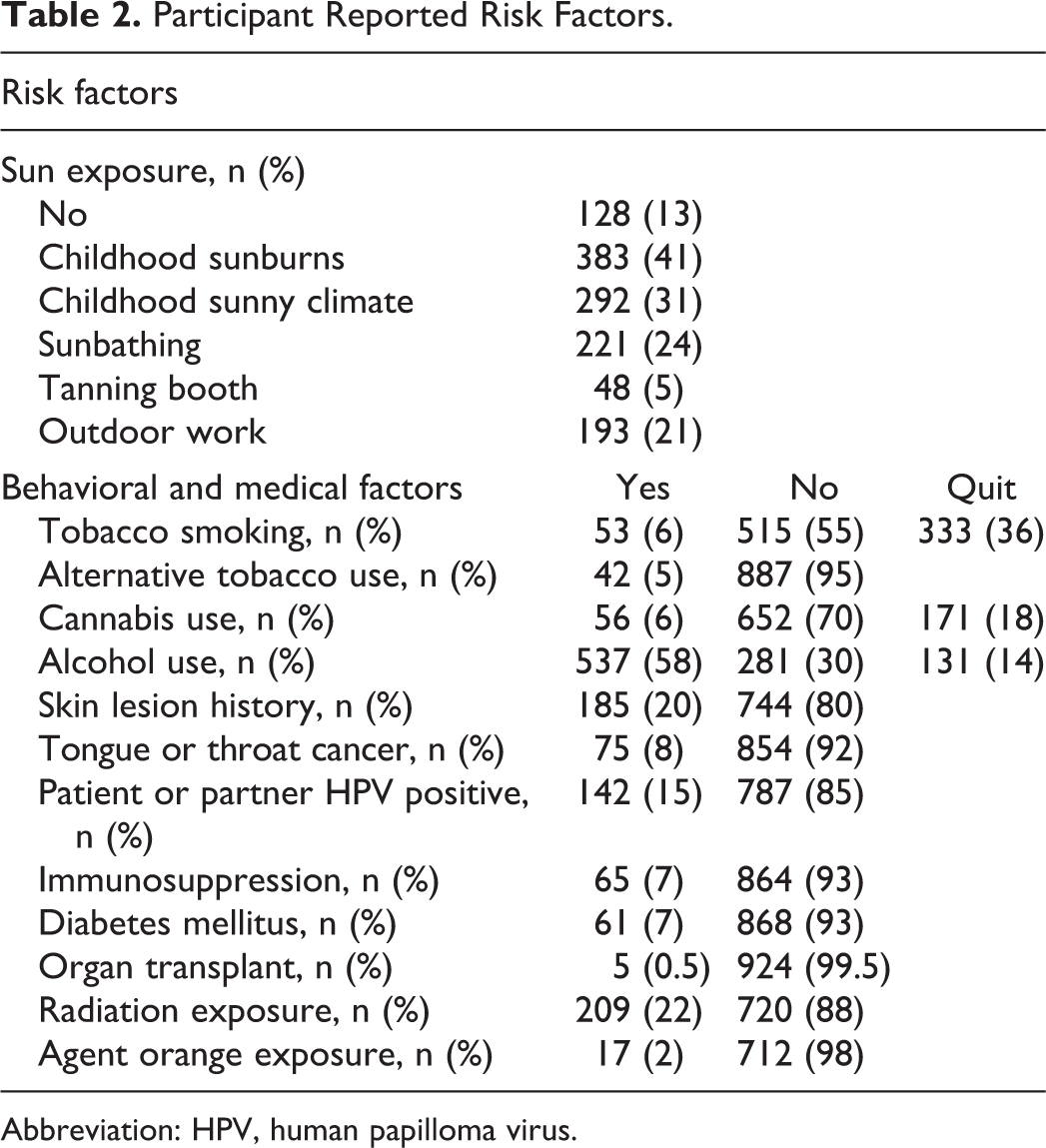
Abbreviation: HPV, human papilloma virus.
Motivational Factors for Attendance
Five motivational factors and a free-response line for attendance of HNCASP were presented to participants at the end of the intake forms and participants could check as many options as they saw fit; these results are shown in Table 3. Desire to learn more about HNC (46%) was the most popular reason for attending the event followed by symptoms related to the head and neck region (30%). Most participants did not utilize the free-response option.
Motivational Factors for Attending HNCASP.
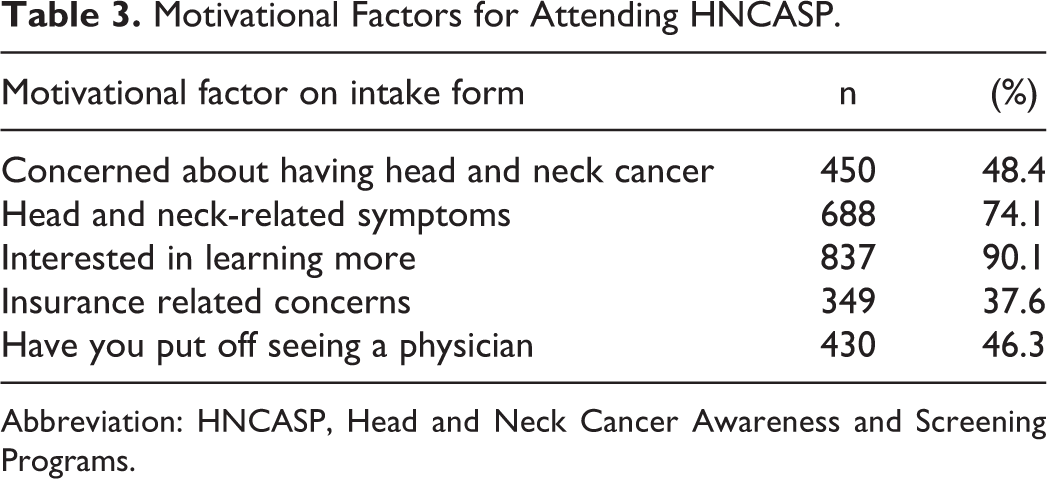
Abbreviation: HNCASP, Head and Neck Cancer Awareness and Screening Programs.
Participant Outcomes
Overall, 17% of patients had a positive screening examination and were recommended to seek follow-up care (Figure 1). Forty-seven of these patients were able to be contacted by phone to assess long-term follow-up. Of those that did not seek further care, a majority reported resolution of their symptoms as the reason for avoiding follow-up; the remaining participants noted a variety of obstacles to seeking care that prevented follow-up. The majority of patients referred for follow-up did seek care with a specialist, and a total of 12 cancer cases were identified, representing 26% of participants that were contacted regarding follow-up, and 1.3% of all participants in the HNCASP. These cancers included 5 basal cell carcinomas, 3 cutaneous squamous cell carcinomas, 2 mucosal squamous cell carcinomas, 1 melanoma, and 1 lymphoma.
Discussion
The debate over the efficacy of HNCASP’s nationally and worldwide remains unresolved with no solid evidence that these events either improve or degrade health outcomes for HNCs. Indeed, earlier detection of cancers improves outcomes; however, screening the general population for low-incidence disease inevitably generates false-positive results, leading to excessive testing, increased medical costs, and undue stress for patients. Beyond the simple service of screening for cancers, HNCASPs also fulfill an educational and awareness role; thus, their impact likely extends beyond the basic numbers of patients screened or cancers identified. Previously, there has not been significant study of the motivations of participants to seek out screening or the long-term outcomes of those who receive a positive screening test at a HNCASP. In this study, we assessed the demographics, motivations, and outcomes for participants of a HNCASP over several years.
Analysis of the demographics of our HNCASP participants demonstrated that participants were generally female, Caucasian, highly educated, and had health insurance and a primary care physician. While the racial mix of participants is likely most reflective of the local demographics, the remaining demographic profile of participants mirrors the findings of previous results of a HNCASP at another tertiary care academic institution. 26 This likely due to the location of the HNCASP on the campus of an academic center. Many of the participants in the HNCASP were employees of the medical center, as the screening event was most convenient for them to attend. This finding was further borne out in the analysis of self-reported risk factors. A significant percentage of participants reported a history of sun exposure and alcohol use, while tobacco use was significantly lower than that typically seen in patients with head and neck cancer. Interestingly, 15% participants reported that either they or their partners were HPV+; knowledge of risk factor is likely not present in the general populations but would not be unexpected in the relatively medically savvy employees of a medical center.
A significant gap in the literature remains regarding the long-term outcomes and follow-up of participants in HNCASPs. While occasionally a diagnosis, or strongly suspected cancer, may be identified at a HNCASP; however, unless the participant returns to the same institution for follow-up and biopsy confirmation, it is quite difficult to determine the overall efficacy of a screening program. Thus, to our knowledge, the telephone follow-up survey conducted in this project is the first data to assess the outcomes of positive screens at a HNCASP. As expected from a telephone follow-up survey, a large number of participants could not be reached or declined to participate. Of all, 57% of those that responded followed up with a physician regarding the findings of their screening, and of these, 12 confirmed cancer were identified. Several other participants were still in the process of evaluation for their screening findings. Thus, the number of cancers identified (1.3% of participants) is likely a significant underestimate of the true number of cancers identified by screening. However, only a few patients with positive screening findings reported not seeking further care due to barriers to medical care access; if screening occurred in a population with different socioeconomic demographics, it is quite likely that far more participants would not receive follow-up.
Even with these caveats, a 1.3% cancer detection rate is comparable to other widespread cancer detection strategies, which are often much more intensive and costly. Colon cancer screening is routinely performed using either colonoscopy or fecal immunochemical testing (FIT). Colorectal cancer detection rates for colonoscopy have been reported between 0.4% and 6.9%,27-29 while FIT cancer detection rates of 0.7% and 0.8%27,28 have been reported. Colon adenoma detection rates are somewhat higher for both tests, although colonoscopy appears superior for this. Similarly, mammography has been shown to have a 2.6% to 5.4%30,31 rate of breast cancer detection. For prostate cancer, the cumulative cancer detection rate over 4 years of prostate-specific antigen testing is 8.2%. 32 Thus, the 1.3% cancer detection rate for HNCASP is in line with other cancer screening procedures, although is much less invasive or costly for participants.
It is important to recognize that there are other, less tangible benefits to a HNCASP. In this study, insurance or care-related concerns were relatively low, with 37.6% of patients noting this as a reason for screening. A far greater percentage of participants (91.1%) noted a desire to learn more about head and neck cancer as a motivating factor for HNCASP attendance. While these relative percentages may vary if the HNCASP were held among a different demographic of participants (eg, in a rural setting or urban underserved area), they do highlight the important role that HNCASP may fill regarding education and improving awareness of head and neck cancer.
This study does have significant limitations that should be acknowledged. As a retrospective review, there is inherent potential for bias with any missing information. Furthermore, telephone surveys typically have low response rates, and a number of participants with positive screening results could not be contacted, which may further bias the results. Finally, the setting and nature of this HNCASP may limit its generalizability to other settings. As noted previously, this event was held on the campus of an academic medical center and served a demographic that trended toward more educated patients with less tobacco use and better access to medical care. Moving the HNCASP to a relatively underserved area would likely significantly increase the cancer rate, but many more patients with significant barrier to care or inability to follow-up may be expected.
Despite these limitations, this study does indicate the value of HNCASPs. The rate of cancer detection is comparable to other, more widespread cancer screening procedures, thus the (relatively small) costs of this and other HNCASP appear justified purely based on potential improvements in oncologic outcome based on earlier cancer detection. However, HNCASP also provide a valuable method for community outreach and education and may have an impact beyond only the number of participants screened on any given day. Future research is needed to better understand the utility of HNCASP in early cancer detection and long-term oncologic outcomes and to determine ways to maximize the educational and community-building aspects of these programs.
Footnotes
Authors’ Note
This project was presented as and oral presentation at AAO-HNSF meeting 2017 in Chicago, Illinois.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: OHSU’s Head and Neck Cancer Screening Program is funded by OHSU’s department of Otolaryngology—Head & Neck Surgery and a supplemental grant from The Oregon Association of Otolaryngology.