
Abstract
Myoepithelial carcinoma of the head and neck is a rare malignant tumor that usually arises from the salivary glands but rarely from the larynx. Here, we describe 11 cases (one treated by us and 10 previously published) of laryngeal myoepithelial carcinoma. Our patient was a 60-year-old male who initially presented with hoarseness and throat pain. The patient had suffered from continuing hoarseness and throat pain for one month before he consulted an otorhinolaryngologist. Computed tomography (CT) scan showed a polypoid tumor involving the right vocal cords. Biopsy was performed, and the disease was pathologically diagnosed as myoepithelial carcinoma of the larynx by hematoxylin-eosin and immunohistochemical staining. The total follow-up period was 15 months. Repeated laryngoscopies or CT scans revealed no recurrence or residual lesion during the post-surgical course.
Introduction
Myoepithelial carcinoma (MEC) can be described as malignant myoepithelioma was first reported by Stromeyer 1 in 1975. It accounts for less than 1% among the salivary glands tumors. MEC arising from the pharynx and larynx is rarer. Ibrahim 2 described the first patient with “MEC of the larynx.” Since then, a limited number of patients with MEC of larynx and pharynx are reported.3 -9 In this study, we describe a case with MEC of laryngeal primary myoepithelial carcinoma and other 10 cases for literature review.2 -9 Clinical data of these 11 cases were analyzed to investigate the biological behavior, diagnosis, treatment, and prognosis of MEC of the larynx.
Case Report
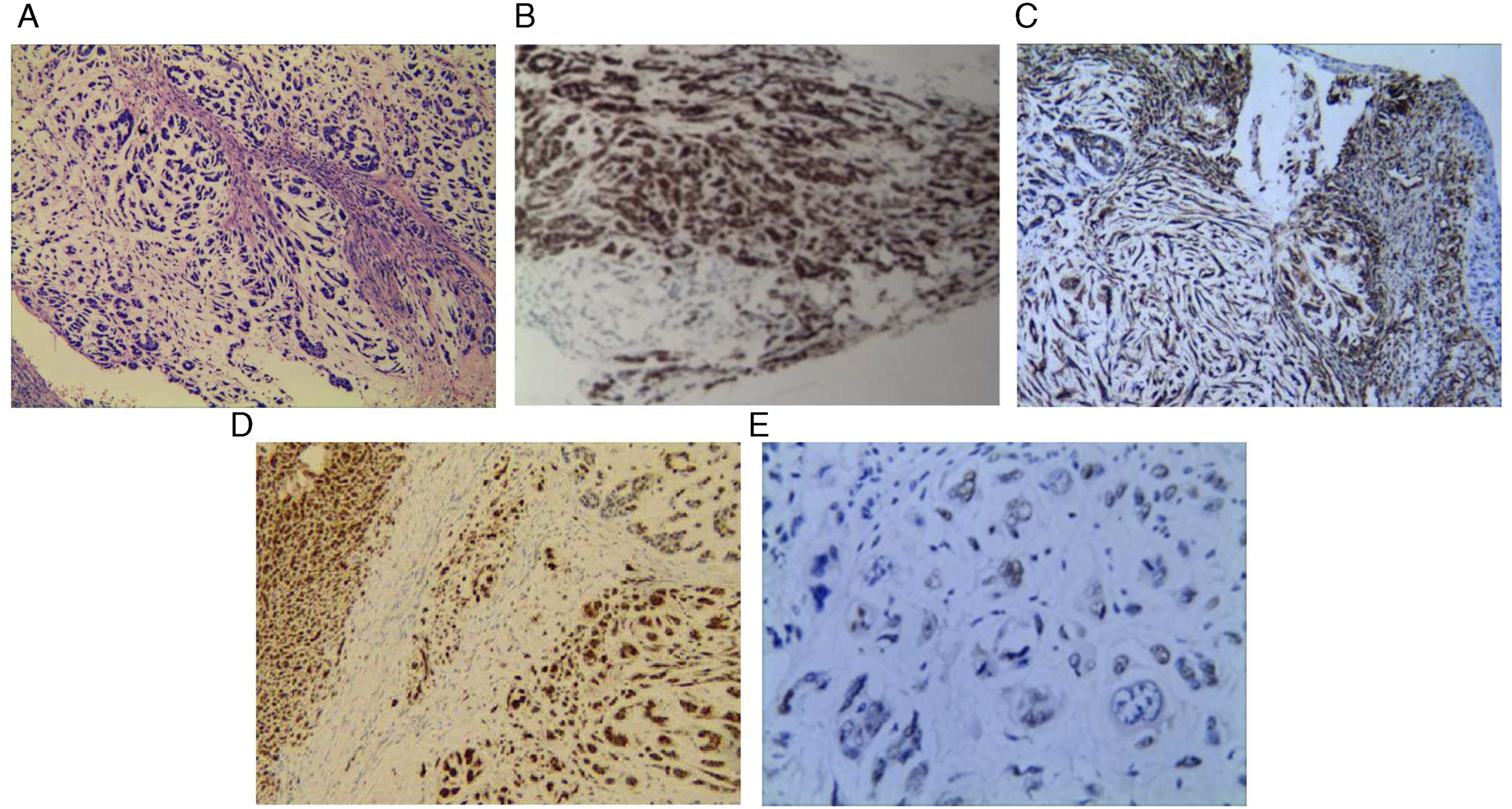
The 60-year-old male patient suffered from hoarseness for six months and throat pain for one month. The patient had smoking history for 15 years with 20 cigarettes or more a day and no previous history of chronic disease. Laryngoscopy showed a cauliflower-like neoplasm at the right ventricle of the larynx (Figure 1A). Computed tomography (CT) of the neck showed irregular soft tissues in the right wall adjacent to the glottis (Figure 1B). Biopsy was performed, and the disease was pathologically diagnosed as myoepithelial carcinoma by histopathology and immunohistochemical staining as follows (Figure 2): S100(+), EMA(+), Vim(+), CK(–), P63(+,less), P40(–), CK5/6(–), SMa(–), Des(–), Myo-D1(–), and Ki67(+,30%). Preoperative neck ultrasonography showed multiple lymph nodes at the bilateral neck (diameter < 1 cm). Liver ultrasonography and chest film showed no abnormalities. The patient underwent tracheotomy under general anesthesia + right partial laryngectomy + laryngoplasty, and received radiotherapy (60Gy) at postoperative 10d. The tracheal tube was smoothly removed after one month. The patient underwent laryngoscopy, ultrasonography and CT at 15-month follow-up, all of which showed no tumor recurrence and metastasis. (A) Laryngoscopy revealed 3 cm × 2 cm cauliflower-like neoplasm (arrow) in the right ventricle of the larynx, which involved the right vocal cord but not the left vocal cord and anterior commissure, while bilateral vocal cords showed normal movement. (B) Laryngeal CT showed irregular soft tissues (asterisk) in the right wall adjacent to the glottis, which protruded towards the pharyngeal cavity. Spindle tumor cells arranged in bundles or micro-cysts with visible mitotic in microscopic evaluation (H&E, ×200) (A) and positive immune staining with EMA (İHC, ×200) (B), S100 (İHC, ×200) (C), Vim (İHC, ×200) (D), and P63 (İHC, ×400) (E).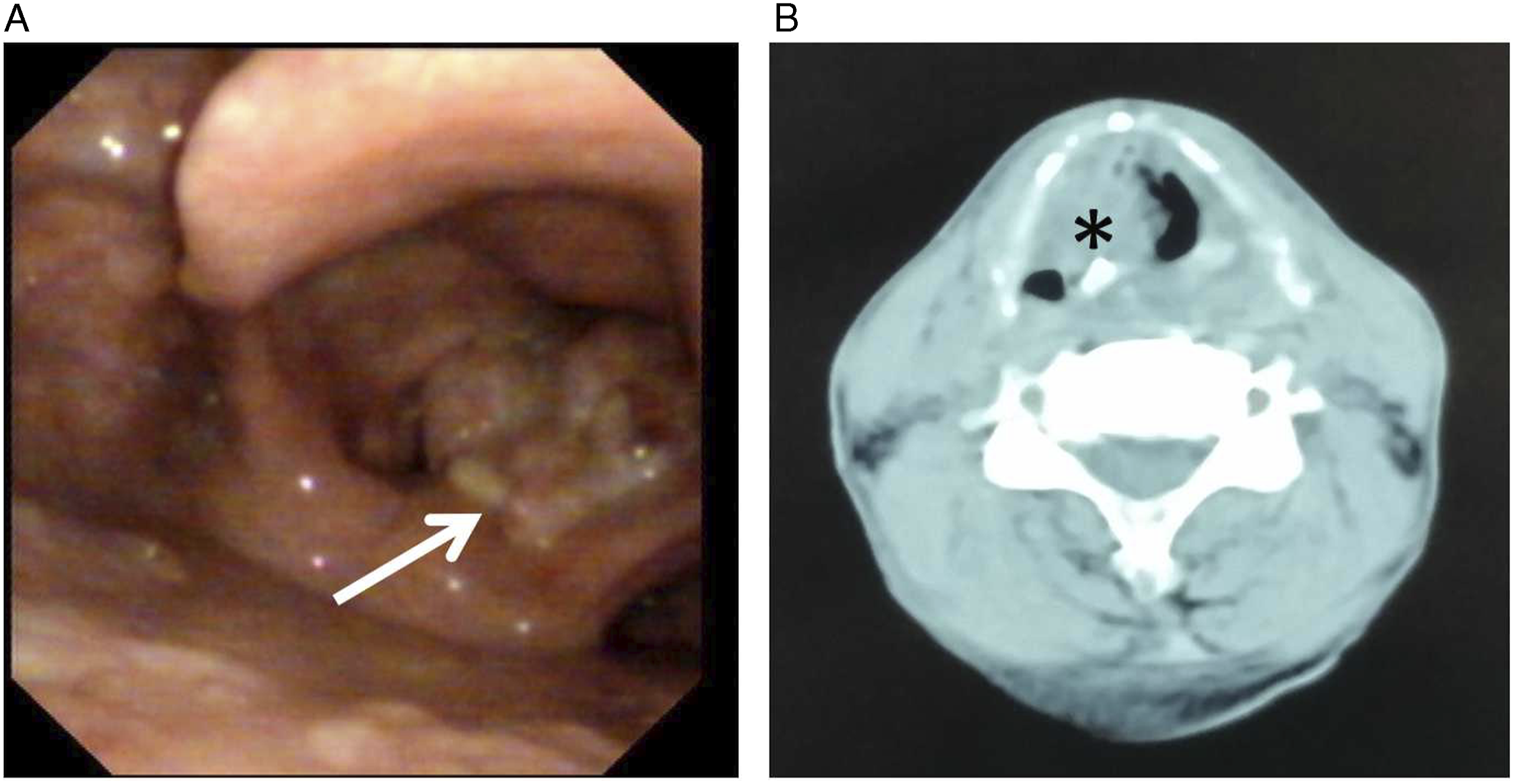
Discussion
Over review of 11 patients with myoepithelial carcinoma of larynx and pharynx.
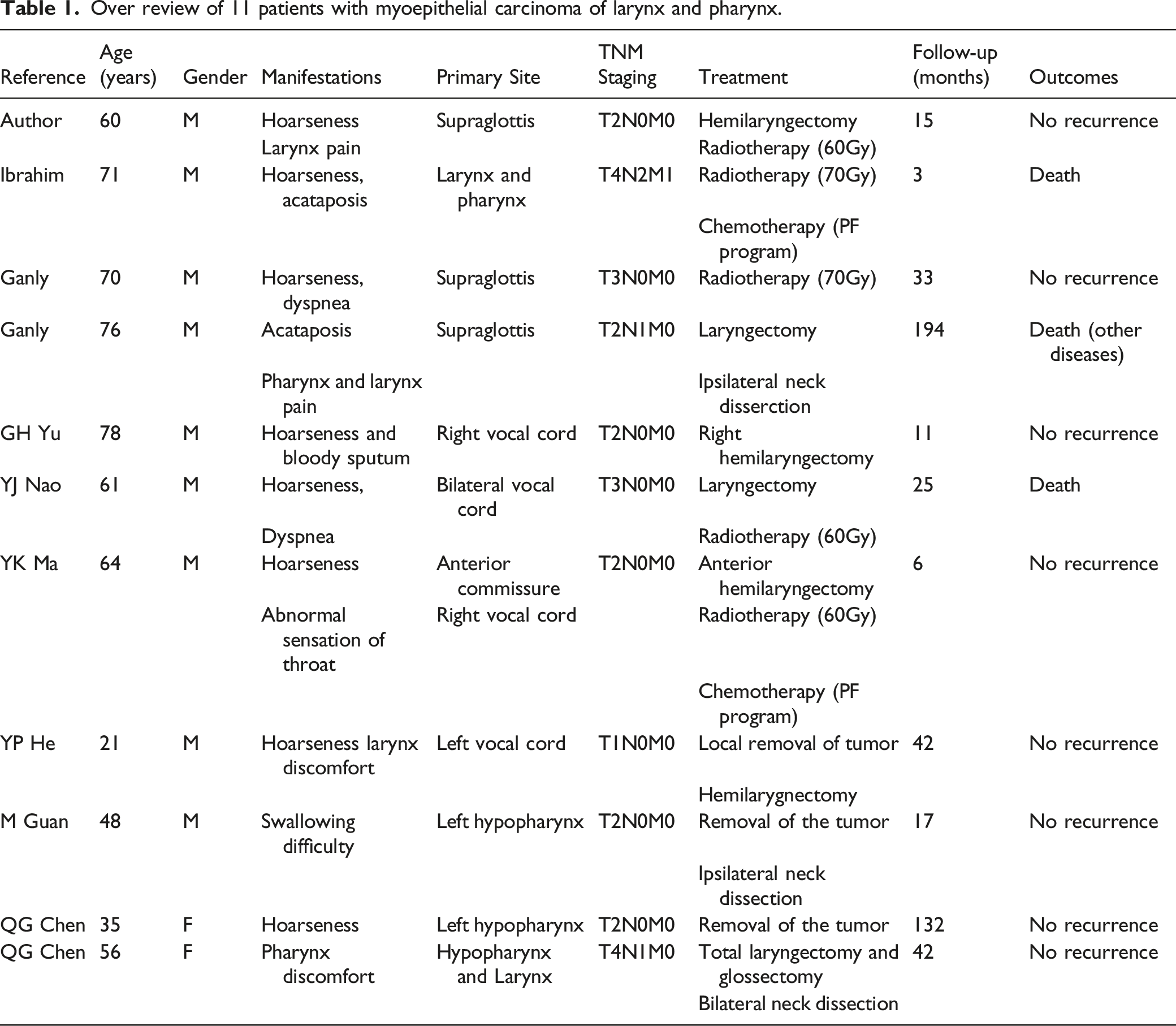
Among the cases, MEC of the larynx and pharynx seemed more prevalent in male (9 of 11, 81.8%). The age ranged from 21 to 78 years, patients over 60-year-old would be at higher risk (7 of 11, 63.6%). The primary site originated from the superior glottis, vocal cords, hypopharynx, hypopharynx involving larynx, and larynx involving pharynx in case 4, 3, 2, 1, and 1, respectively. The symptoms mainly manifested as hoarseness as well as pharyngeal and laryngeal discomfort at the early stage. Besides, hoarseness, acataposis, and dyspnea would occur at the late stage. Three cases were accompanied by lymphatic metastasis and one by distant metastasis (hepatic metastasis).
Currently, MEC is typically treated by surgery. The resection range should be expanded as much as possible after considering local anatomy and function. There should be sufficient secure boundary, and intraoperative frozen sectioning should be performed, if necessary, to determine the secure edge for tumor incision. In this study, 9 out of 11 patients (81.8%) underwent surgery, different operational treatments are described in Table 1, of which two cases were preoperatively confirmed with lymphatic metastasis and underwent functional neck dissection, one case underwent preventive neck dissection because the disease was located at hypopharynx, while the other cases did not receive preventive neck dissection and did not suffer from lymphatic metastasis during the postoperative follow-up. Thus, we believe that preventive neck dissection is unnecessary in patients with CN0 MEC of the pharynx and larynx.
Among all 11 patients, two patients did not accept operation, one of which suffering from distant metastasis at admission was given radio-chemotherapy and died after 3 months, another was given radiotherapy alone because of his refusal to surgery and did not show recurrence after 33 months. Moreover, three cases received postoperative radiotherapy, of which one died during a 25-month follow-up due to recurrence, and other two did not show recurrence during the follow-up. Thus, we believe that radiotherapy has a definite curative effect on MEC of the pharynx and larynx, and the necessity of postoperative radiotherapy should be determined according to the tumor staging.
Since MEC of the pharynx and larynx is very rare, its biological behavior remains unknown. In this study, 8 out of 11 patients (72.7%) did not show recurrence while three cases were reported died during follow-up (one with distant metastasis at admission died after diagnosis for 3 months, one died because of cardiovascular disease after 194-month follow-up and one died postoperatively of recurrence after 25 months). Therefore, MEC of the pharynx and larynx may not be highly malignant.
MEC has a high blood metastasis rate, which was reported to be 26.3–47%. 11 Thus, patients with MEC of the head and neck generally undergo preoperative chest film, liver B-ultrasound, and nuclear bone scan, if necessary, to exclude the possibility of distant metastasis.
Conclusion
MEC of the pharynx and larynx is a rare malignant tumor without characteristic manifestations due to diverse cellular morphologies. Its pathological features are not directly associated with the outcomes, leading to numerous controversies in diagnosis and treatment. We believe that surgical resection is the main treatment method for such invasive diseases with high recurrence and metastatic potential. For most cases, we should strive to achieve extensive resection with clean margin, which is closely associated with prognosis and survival rate of the disease. Meanwhile, we should determine the necessity for auxiliary radiotherapy and chemotherapy according to tumor staging and clean margin. Although this is a retrospective analysis of a small sample size, we believe that it can enrich the knowledge of MEC of the pharynx and larynx.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by a grant from the Youth Medical Talent Training Program of Pudong Health Bureau of Shanghai (PWRq2020-50), the Natural Science Fund Project of Anhui University (KJ2020A0590), the Talent Training Program of Pudong New Area Gongli Hospital (GLRq2020-01).
Informed consent
This is a retrospective case report. Approval for the release of data for this project was conducted according to the World Medical Association Declaration of Helsinki and granted by the First Affiliated Hospital of Bengbu Medical College. This patient provided written informed consent.