
Abstract
Nasal primary tuberculosis (TB) of the upper respiratory tract is rare and barely reported in literature. Herein, we report a complicated case of nasal primary TB with otitis media. The patient visited the ENT clinic due to left-side nasal obstruction accompanied by rhinorrhea, and intermittent headaches. The diagnosis of nasal TB was confirmed with an acid-fast bacterial test and histopathological examination. After 3 months of treatment with anti-TB drugs, patient’s symptoms of nasal obstruction, rhinorrhea, and other symptoms were remarkably relieved. The left ear purulence substantially reduced. The patient recovered well and had no recurrence post half a year of follow-up. Our case emphasizes the importance of accurate diagnosis and initiation of timely treatment. Additionally, when a patient has nasal TB complicated with otitis media, it is important to consider a diagnosis of middle ear TB.
Introduction
The most common site of tuberculosis is the lungs, and the active phase of TB is infectious. TB can simultaneously metastasize in the body leading to extrapulmonary TB, which can occur in almost any part of the body, and is commonly found in the digestive system (intestinal TB), motor system (bone TB), urinary TB, genital TB, lymphatic TB, etc. 1 Nasal primary TB is rare and barely reported in the literature. Patients with nasal TB are predominantly male, and the youngest onset age of the disease is only 5 years, while the oldest is 79 years; hence, nasal TB can occur at any age.2,3 People with low immunity, residing especially in the high incidence areas are vulnerable to primary upper respiratory tuberculosis. 4 Although upper respiratory TB is difficult to establish, the histological and immunohistochemical examination of the lesion is often required to aid diagnosis. The possibility of TB should be considered when pathological results show granulomatous inflammation. This article presents a very rare case of nasal TB.
Case report
A 42-year-old woman visited the ENT clinic because of left-side nasal obstruction accompanied with rhinorrhea, and intermittent headaches. She had undergone endoscopic right-sided sinus fenestration for chronic sinusitis three months ago and recovered well. 2 months before the visit, she presented with left-sided nasal obstruction and rhinorrhea. She was diagnosed with acute sinusitis, and received several courses of anti-infective treatment with no relief of nasal congestion symptoms in another hospital. She had previously denied history of hypertension, diabetes, cardiac disease, AIDS, syphilis, hepatitis, TB, and any contact with a TB patient. On physical examination, the left nasal mucosa showed diffuse edema, and poorly visible nasal structures. After the left nasal mucosa sufficiently contracted, the surrounding mucosa of the middle turbinate was erosive, the surface had white pseudomembranes, and a small amount of bleeding when touched. The surrounding tissues with pseudomembranes were sent for general bacterial culture, concentrated colony acid-fast bacteria detection, and histopathological examination. Additionally, purulent secretions could be seen in the left external auditory canal, and the eardrum was not visible. The patient's temperature fluctuated within the normal range during hospitalization, and vital signs were stable.
On admission, electronic laryngoscopy and otoscopy revealed swelling and erosion of the left-side nasal mucosa, postoperative changes in the right nasal sinus (Figure 1A-C), no abnormalities in larynx (Figure 1D and E), and purulent otitis media on the left side (Figure 1F). Electronic fiber layrngoscopy before treatment. A–B: The left nasal cavity. D–E: The layrngeal. F: The left ear.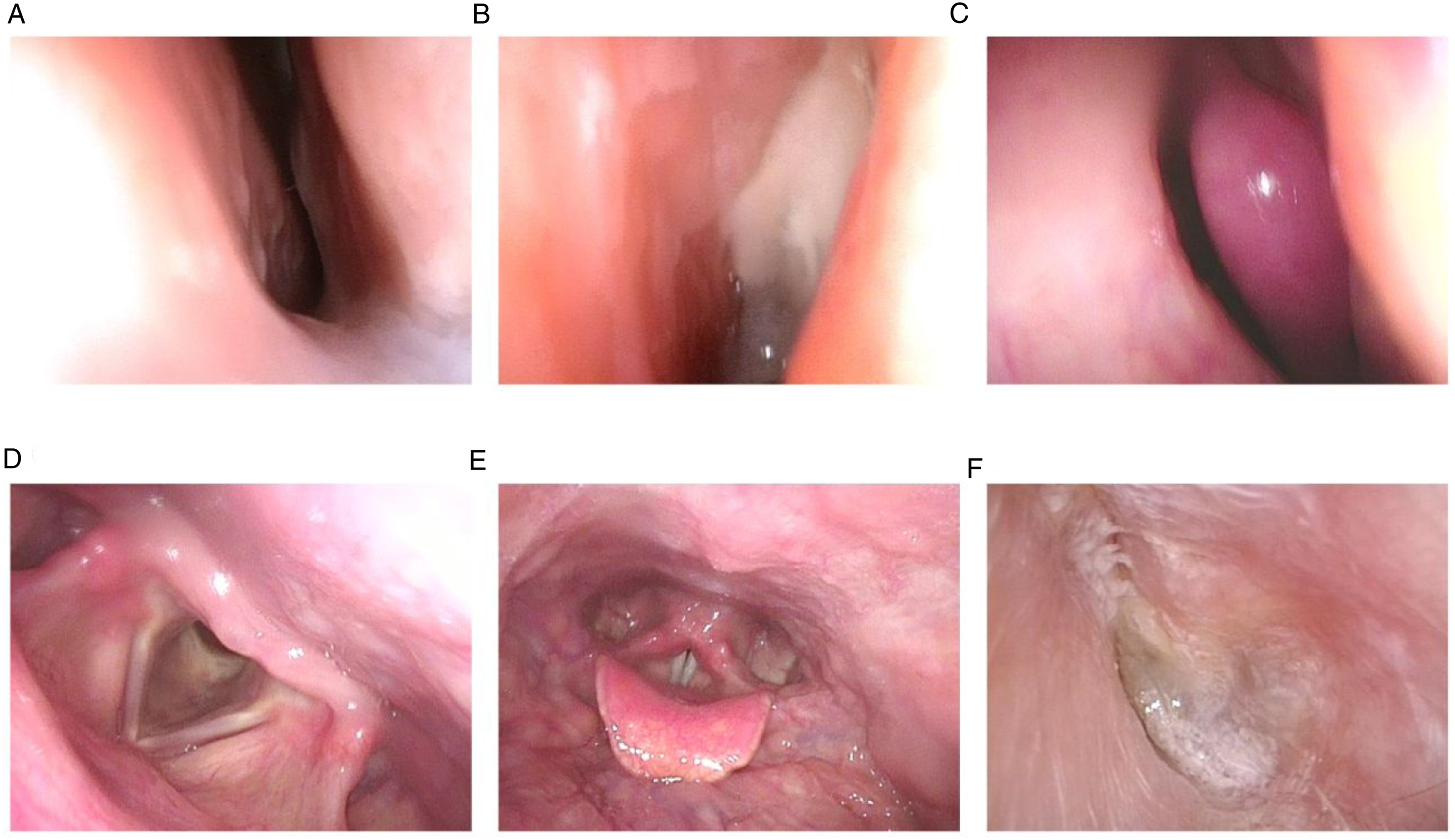
Computed tomography (CT) of the paranasal sinuses revealed extensive thickening of the left maxillary and ethmoid sinus mucosa and hypertrophy of the inferior turbinate (Figure 2). Paranasal sinus CT scan before treatment. A–B: Axial CT scan of the paranasal sinus. C: Coronal CT scan of the paranasal sinus.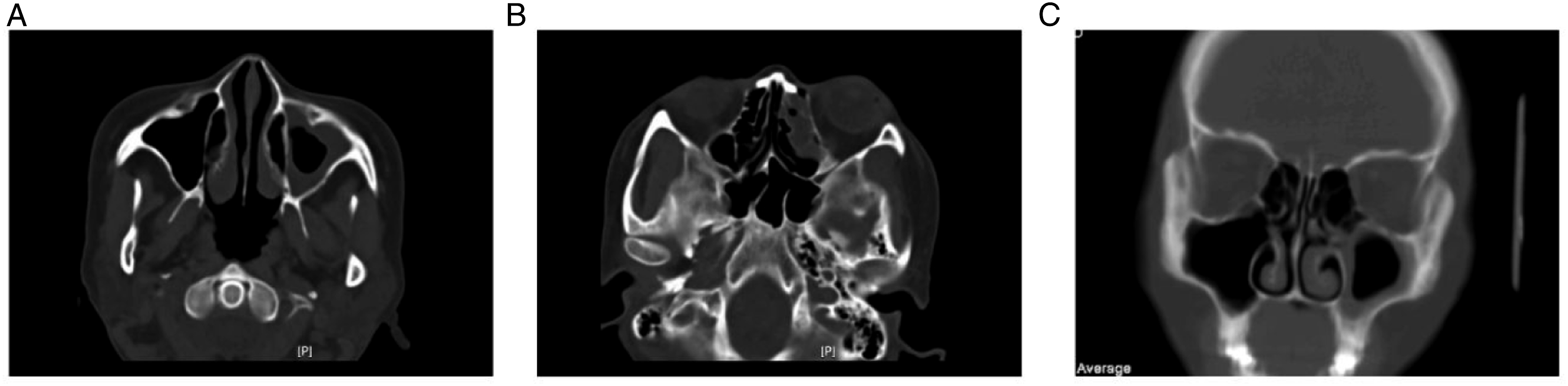
B-ultrasound of both parotid and cervical lymph nodes revealed several lymph nodes in areas I and II of the left neck showing regular morphology with poorly defined hilar structures, measuring approximately 1.6 × 0.7 cm and located in the angle of the mandible, while no obvious lymph nodes were found on the right side. Chest CT showed no significant abnormalities, nodular lesions, or pulmonary infiltrates (Figure 3). Chest CT scan on admission.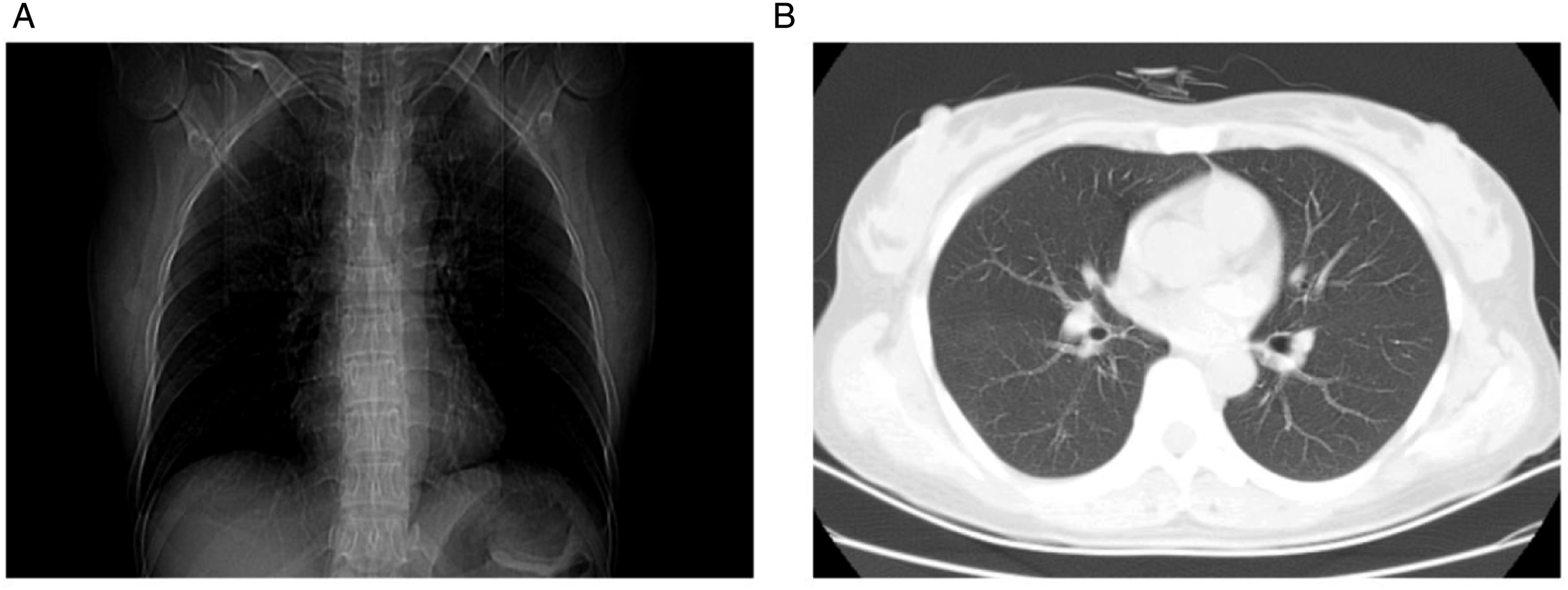
A concentrated colony of acid-fast bacteria test detected acid-fast bacilli (++). Histopathology showed epithelioid cell granulomas in the lamina propria (Figure 4A-C), and acid-fast staining was positive (Figure 4D-F). Given the results, we finally diagnosed the patient with primary nasal TB. A–C: Pathological examination of mucosa in left nasal cavity lesion. D–F: Acid-fast staining of mucosa in left nasal cavity lesion.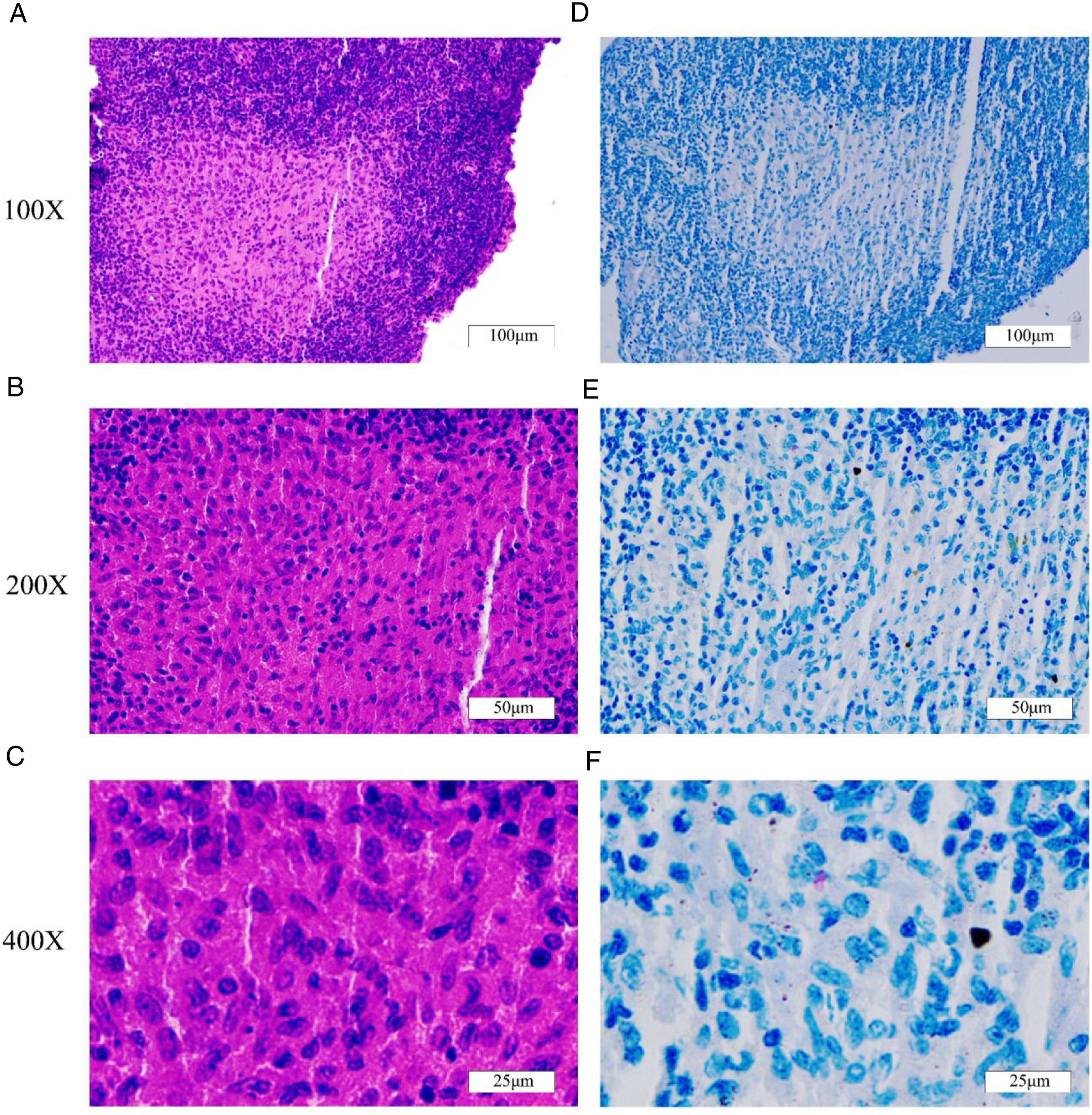
During follow-up, the patient received regular anti-TB treatment at the local infectious disease hospital, the regimen included isoniazid tablets (0.3 g, QID), rifampicin capsules (0.45 g, QID), ethambutol hydrochloride tablets (0.75 g, QID) and pyrazinamide tablets (0.5 g, TID). The proposed treatment course was 3–6 months, and the patient's nasal congestion symptoms relieved after 1 month of treatment. The patient received anti-TB treatment for approximately 3 months, and self-reported nasal obstruction, rhinorrhea, and other symptoms remarkably reduced. In addition, the left ear purulence was substantially reduced. Follow-up electronic laryngoscopy showed bilateral smooth and normal colored nasal mucosa. The right nasal sinus showed postoperative changes (Figure 5A-C), and the larynx appeared normal (Figure 5D and E). Electronic otoscopy revealed no purulent discharge from the left ear, marginal perforation of the tonus of the tympanic membrane, and intratympanic dryness (Figure 5F). Electronic fiber laryngoscopy after treatment. A–B: The left nasal cavity. C: The right nasal cavity. D–E: The laryngeal. F: The left ear.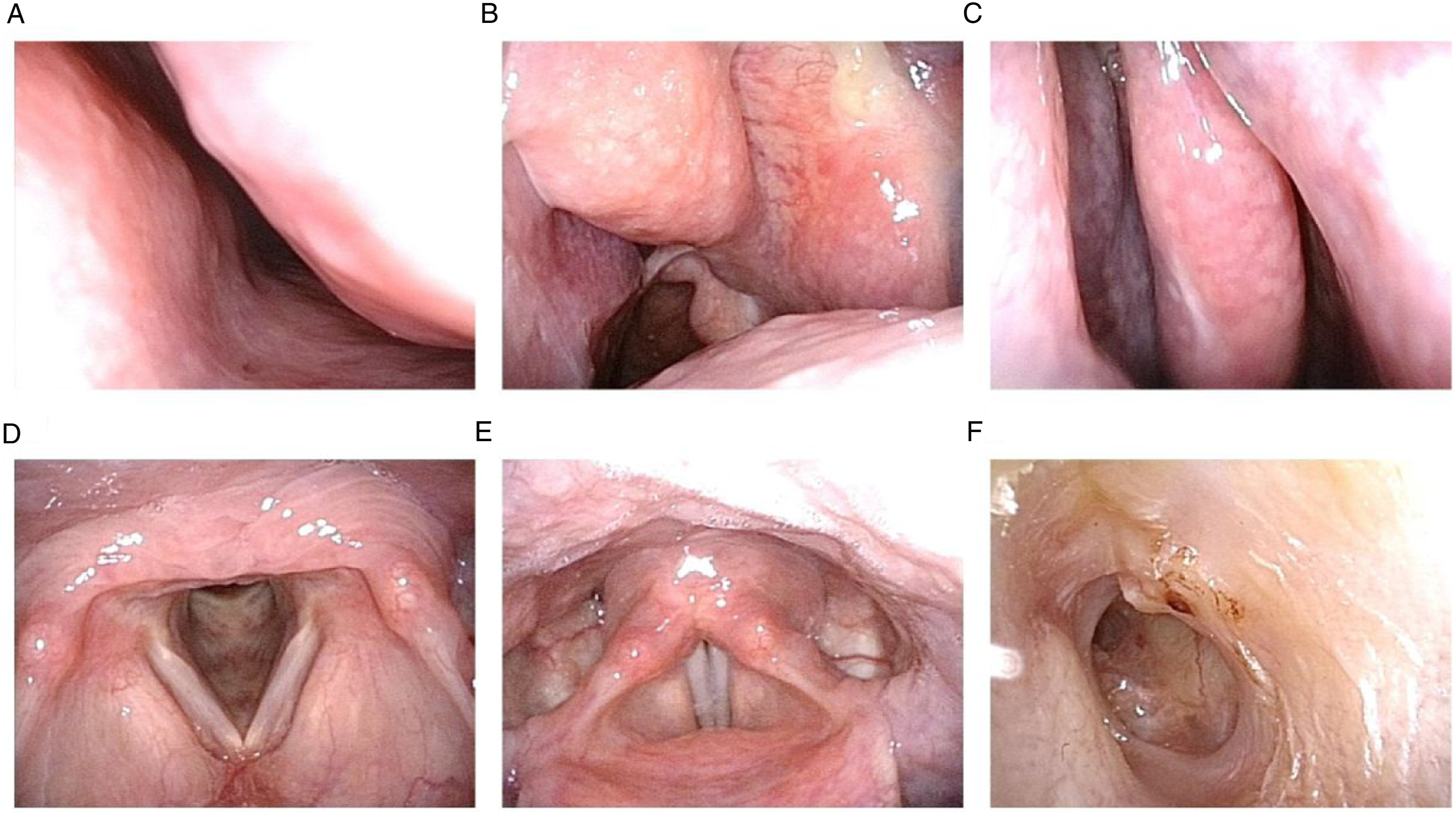
B-ultrasound of the bilateral parotid and cervical lymph nodes showed no significant enlargement of lymph nodes in areas I and II of the left neck. Sinus CT showed less left-sided sinus inflammation than before (Figure 6). Paranasal sinus CT scan after treatment. A–B: Axial CT scan of the paranasal sinus. C: Coronal CT scan of the paranasal sinus.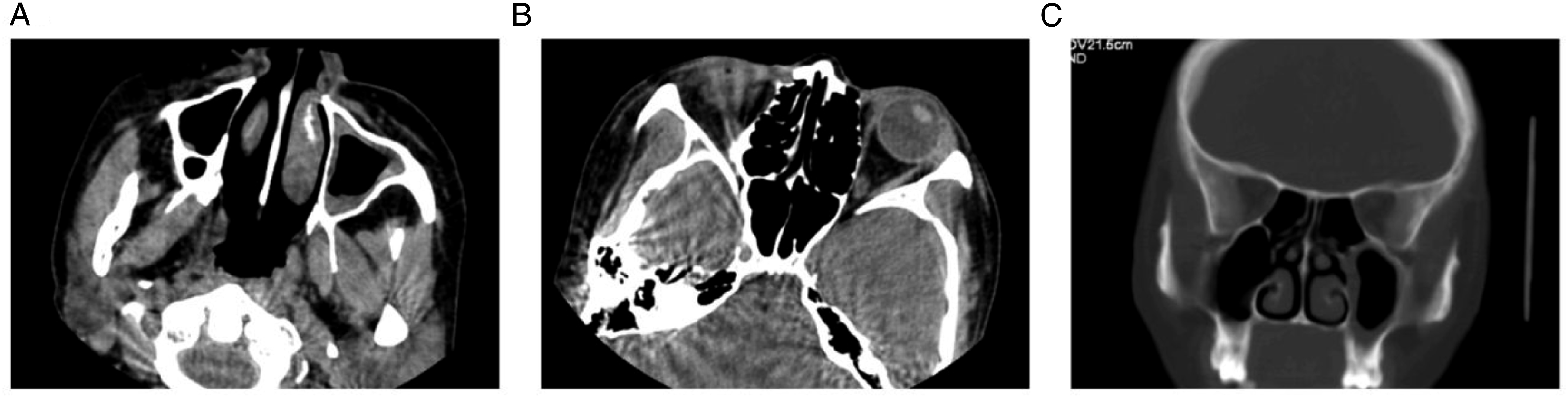
Colony acid-fast bacteria test of nasal secretions was negative. Pathological examination revealed multiple foci of lymphocyte infiltration in the mucosal tissue of the left nasal cavity, and the formation of follicle-like structures in some areas, consistent with chronic inflammation. Acid-fast staining was negative. Based on these results and the effectiveness of anti-TB drug treatment, we recommended infectious disease hospital visits, suspension of oral anti-TB drugs, and regular follow-up.
Discussion
TB is a specific infectious disease that occurs after infection with Mycobacterium tuberculosis, and its most common site of infection is the lung. Primary nasal TB is rare with no more than 50 cases reported in the literature worldwide.5 -7 The main symptom is nasal obstruction, which is rarely accompanied by rhinorrhea, hyposmia, and cervical lymphadenopathy. Most patients with primary nasal TB are infected due to low immune resistance; there are literature reports of patients with immunodeficiencies who have been infected with TB. 4
In upper respiratory tract infections, the symptoms of TB are atypical, as the patients generally do not present with low fever, night sweats, and other typical symptoms of TB; most patients will first experience symptoms of nasal obstruction, and when the lesions involve the nasal septum, they may present with nasal septal perforation. 8 Vocal cord and laryngeal lesions can occur when the lesion invades the hypopharynx. TB sometimes can invade the sinuses, mainly because tuberculosis bacilli can degrade the bone. In known case reports of nasal TB, with an average age of approximately 35 years, nasal TB infections can present at various sites in the nasal cavity.9,10 The disease progresses slowly, and generally difficult to diagnose; thus, it is often mistaken for other infections. In this case, the patient's clinical symptoms were similar to previous cases of nasal TB, which were dominated by nasal obstruction and extensive edema of the nasal mucosa; however, the site of onset was dominated by the middle turbinate, and CT showed mucosal thickening of the left maxillary and ethmoid sinus, which suggested that the lesion invaded the maxillary and ethmoid sinus. Previous cases of sinus lesions are rarely reported.
In the laboratory examination of TB, it is necessary to perform the PPD test, erythrocyte sedimentation rate, Mycobacterium tuberculosis antibody test, bacterial culture, concentrated Aggregatibacter acid-fast bacteria test, and T-SPOT among others. 11 Nasal TB is often characterized by granulomatous inflammation microscopically centered on a granular, bright eosinophilic mass surrounded by numerous epithelioid cells (vesicular nucleus surrounded by chromatin aggregates, visible nucleoli, and abundant eosinophilic cytoplasm). Mega-multinucleated cells with abundant cytoplasm and dark nuclei, a horseshoe-shaped arrangement, and numerous small reactive lymphocytes are observed under the cell membrane. In addition, common eosinophils and rare neutrophils are observed. Routine blood and bacterial cultures were performed and the patient showed no abnormalities; the T-SPOT test result was negative, but the concentrated colony acid-fast bacteria test result reported a critical value. The T-SPOT test often appears positive in the confirmation of pulmonary TB, but these are sometimes false-positive results. The disease microscopically shows a typical TB granuloma morphology, and a large number of scattered TB bacilli visible at the granuloma site in the acid-fast staining. Routine testing for rare nasal-specific infectious diseases, such as nasal TB, typically yields negative results; however, the concentrated Aggregatibacter acid-fast bacteria test of secretions is highly sensitive, and can be the first choice in the laboratory examination; additionally, acid-fast staining of tissues demonstrates the infiltration of acid-fast bacilli, which can be an important basis for diagnosis.
During the diagnosis and treatment of infectious diseases of the nasal cavity, nasal TB is often ignored because the most common chronic inflammatory diseases of the nasal cavity, such as chronic sinusitis with polyps, have nasal obstruction and rhinorrhea as their main symptoms. In addition, mucosal erosive changes are present in tumors of the nasal cavity, such as lymphoma. Many pathologies that can present with a granulomatous reaction; caused by Mycobacteria or fungi should initially be excluded. This response has been observed in various types of cutaneous lymphomas, and several reports have confirmed the relationship between granulomatous inflammation and cutaneous ENK/T-lymphoma by mimicking infectious panniculitis. 12 In addition, the differential diagnoses of nasal TB include fungal infection, Wegener's granuloma, sarcoidosis, nasal sclerosis, and leprosy. This case showed mucosal lesions, high-grade edema, and granulomatous inflammation of tissues under the microscope that had similarities to the symptoms of other diseases, and was difficult to differentiate. In the process of diagnosis and treatment, we needed to comprehensively analyze the condition, initially screen the suspected case, examine the acid-fast staining of secretions, and perform an immunohistochemical in-depth analysis.
Patient with nasal TB recovered at the 6-month follow-up. 4 Nasal TB lesions have been reported to be more extensive, and when symptoms such as perforation of the nasal septum, sinus invasion, or even vocal cord involvement, such as dysphonia and dysphagia, occur, surgical resection of the diseased tissue is required, along with postoperative anti-TB treatment. 9 Taken together, anti-TB drugs can treat nasal TB with a smaller area of infection, but when the lesion area is larger (involving the sinuses, nasal septum, and even the larynx), it is treated with surgical preemptive anti-TB treatment for >1 month, followed by surgery. Postoperative anti-TB treatment is continued until the disease is cured. In this case study, we found that symptomatic treatment based on a definite diagnosis can achieve good clinical results.
Nasal TB, a rare disease with an atypical clinical manifestation, presents with no systemic symptoms such as cough, night sweats, or mid-afternoon low fever, and non-specific nasal and sinus examination. Moreover, it is difficult to differentiate it from common infectious diseases, and hence, it is easily misdiagnosed. Once the bacteria are demonstrated in culture, a definite diagnosis is achieved, but culture requires a longer time. Concentrated acid-fast bacteria test results (++), pathological examination results showing granulomatous nodules, and positive acid-fast staining of pathological secretions provided a basis for the diagnosis of this patient. When a patient is suspected of having a particular infection, such as nasal TB, histopathological examination of the nasal mucosa and bacteriological examination could help make a rapid and definite diagnosis.
There were also deficiencies in the diagnosis and treatment of this case, as suggested by the patient's double parotid glands and B-ultrasound of cervical lymph nodes; several lymph nodes were found in areas I and II of the left neck. Whether this was a reaction of the lymphatic system caused by nasal TB leading to lymphadenopathy or whether isolated left-sided lymphadenopathy had recently resulted from other causes was unknown, failing to establish a further definitive diagnosis at that time. However, the patient underwent anti-TB therapy for 3 months, and a review of the bilateral parotid glands and cervical lymph node B-ultrasound showed no significantly enlarged lymph nodes in the left neck. We, therefore, suspected the cervical lymphadenopathy to be due to nasal TB. In addition, the patient was admitted to the hospital with more purulent discharge visible in the left external ear canal and was given topical levofloxacin ear drops, but the effect was suboptimal; after anti-TB treatment, there was no purulent discharge from the left ear external ear canal and intratympanic dryness. We concluded that this patient had nasal tuberculosis combined with middle ear TB despite the lack of pathogenic microbiology examination and testing, which was not deeply studied in this case. In future clinical diagnosis and treatment, we should note that, when the patient has nasal TB complicated with otitis media, diagnosis of middle ear TB and relevant examinations should be performed to further confirm this diagnosis.
Footnotes
Author’s note
Li Hou is the corresponding author, and she contributed to the conception of the study. Zhijuan Zhang and Zheng Ma are the co-first authors who contribute to writing this manuscript. Yanrong Li and Jingyuan Wang contribute to collecting images. All authors read and approved the final manuscript. Zhijuan Zhang and Zheng Ma contributed equally to this work.
Declaration of conflict interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The research is approved by the Ethics Committee of the General Hospital of Ningxia Medical University.