
Abstract
Introduction
Nasal packs (NPs) are commonly used in nasal surgical procedures. 1 However, despite their benefits, NPs also contribute to postoperative morbidity in patients, causing pain, respiratory complications, and adverse cardiovascular changes. 2 On the contrary, transseptal suturing septoplasty (TSS) has been shown to reduce these adverse effects, improving patient satisfaction. TSS also positively affects patients’ quality of life. 3
As individuals age, an increase in surgical morbidity and mortality is often expected due to changes in their cardiovascular and respiratory systems. 4 Using nasal packing further increases the risk of cardiovascular and respiratory complications in elderly patients.1-4 This study aimed to evaluate the impact of TSS on elderly patients as a means of reducing these risks. The objective was to assess the effects of TSS on the elderly population and determine if it is a safer alternative to nasal packing.
Materials and Methods
Elderly patients who received septoplasty were prospectively divided into 2 groups. Nasal obstructions in these patients were evaluated based on standardized cosmesis and health nasal outcomes. The Turkish version of Standardized Nasal Cosmesis and Health Outcomes–Obstruction (SCHNOS-O) was adopted by Gode et al 5 to evaluate nasal and respiratory functional outcomes in Turkish-speaking patients. 5 The University Ethics Committee for Clinical Research approved the study protocol (project no.: KA 22/13).
This study excluded patients who had previously undergone surgeries or additional surgical procedures along with septoplasty, such as rhinoplasty or concha surgery. All patients who were included in the study provided informed consent.
Surgical Procedure
Cottle’s technique was used to perform septoplasty in patients under general anesthesia. Before incisions were made, the submucoperichondrial planes were bilaterally infiltrated with Lidocaine HCl 1% and 1/100,000 epinephrine. The NPs (Merocel Standard Nasal Dressing; Medtronic Xomed, Inc) were placed bilaterally in the nasal cavities of Group 1 patients. For Group 2 patients, horizontal transseptal mattress sutures were placed in the nasal septum using 4/0 polyglactin 910 (Rapid Vicryl; Ethicon Inc).
All patients received prophylactic antibiotics (cefazolin sodium 1 g intramuscular preoperatively) and 3 × 500 mg of paracetamol orally in the postoperative period. The NPs were removed within 24 hours.
Later, patients’ oxygen saturation (OS) levels were monitored with a pulse oximeter for 24 hours in all cases.
Antihistamines, nasal steroids, or decongestants were not allowed for 1 month after the operation. Patients’ postoperative pain was determined using the visual analog scale (VAS). The postoperative nasal openings of the patients were rescored after 1 month. The preoperative and postoperative SCHNOS-O scales, VAS scores, and OSs were compared.
SPSS software was used for the statistical analysis (Statistical Package for the Social Sciences, version 17.0; SSPS Inc). Comparisons of the SCHNOS-O scale, VAS score, and OS level were made using the Wilcoxon signed rank test. A P value of less than 0.05 was deemed to be statistically significant.
Results
The study involved 26 patients ranging from 65 to 74 years, with an average age of 66. Patients were divided into 2 groups, each consisting of 13 individuals. The demographic characteristics of both groups were comparable, with a similar distribution of ages and sex.
The Levene test was used to determine the homogeneity of the groups and the results, as shown in Table 1, indicated that the groups were consistent in terms of their sample variance.
Patient Demographic Data.
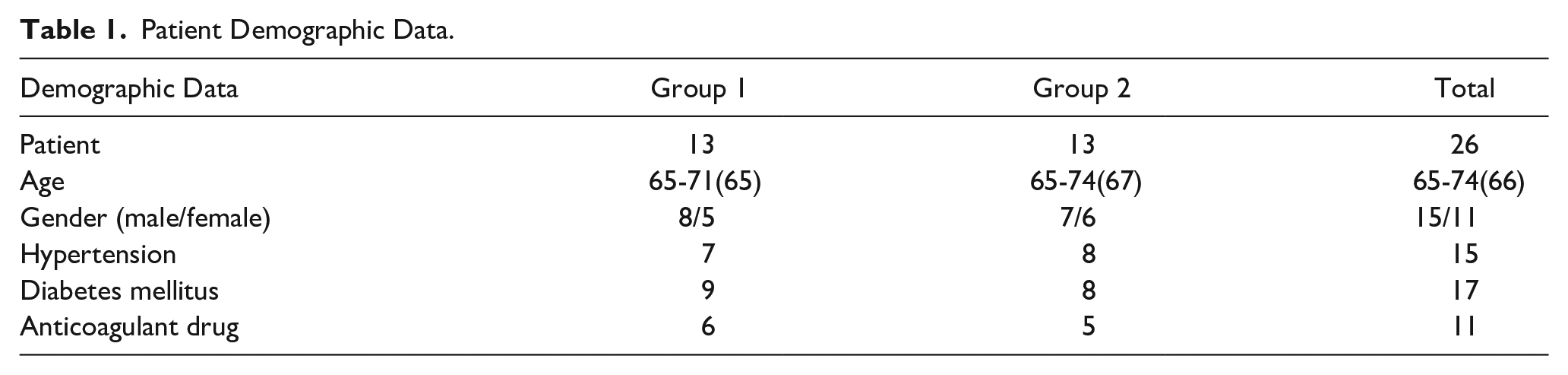
Table 2 shows the variations between the SCHNOS-O scores of the groups. Statistical analysis revealed no significant differences between the 2 groups in terms of postoperative SCHNOS-O scores, as evidenced by a P value greater than .05. However, within each group, there was a statistically significant difference between the preoperative and postoperative SCHNOS-O scores, as indicated by a P value less than .05.
A Comparison of Both Groups in Terms of Their SCHNOS-O Scores.

Abbreviation: SCHNOS-O, Standardized Nasal Cosmesis and Health Outcomes–Obstruction.
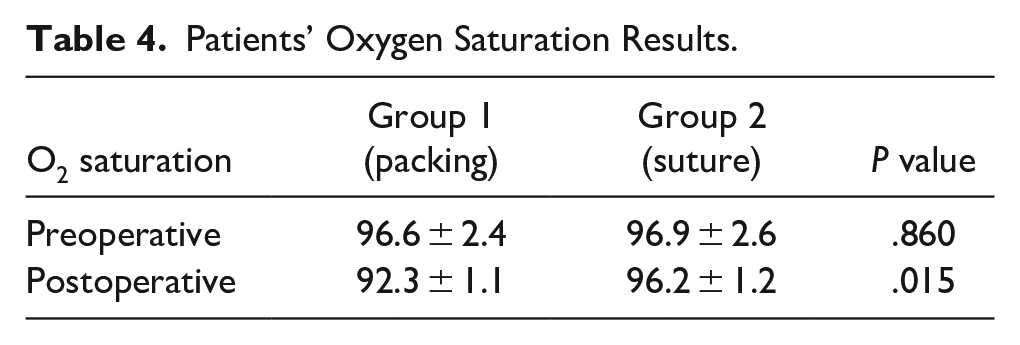
Table 3 compares the postoperative pain results of the patients and Table 4 shows the OS results of the 2 groups. The results showed that in group 1, the mean pain scores were significantly higher (P < .05) than in the other group. In contrast, the mean OS levels were significantly lower (P < .05).
A Comparison of the Patient’s Postoperative Pain Outcomes.
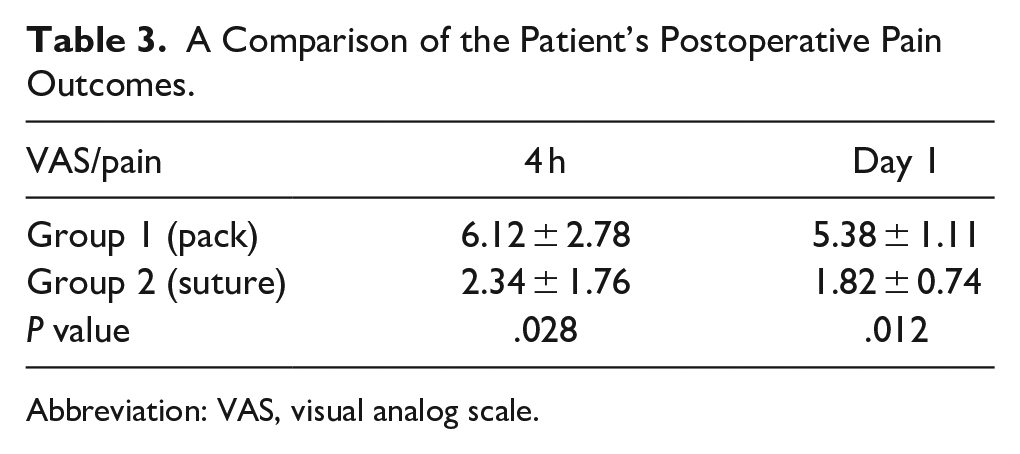
Abbreviation: VAS, visual analog scale.
Patients’ Oxygen Saturation Results.
No septal hematoma or major bleeding was observed in the patients in either group.
Discussion
NPs are commonly utilized in nasal surgery to control bleeding, prevent hematomas, secure bone or cartilage grafts, and stabilize the septal flap. However, previous studies have shown that the use of NP negatively affects patients’ quality of life.1,3,6,7 Our study found that patients in the group receiving NP experienced significantly higher postoperative pain scores than those in the group receiving TSS, which is consistent with previous research findings. Therefore, TSS was a more cost-effective and less painful alternative to NPs. 8
The elderly population is prone to a higher rate of surgical morbidity and mortality due to age-related changes in the cardiovascular and respiratory systems and increased rates of diseases such as hypertension and diabetes. The use of NP during nasal surgery in this population exacerbated cardiovascular and respiratory risks and was found to result in low levels of postoperative oxygen saturation in our study. On the other hand, TSS was found to reduce respiratory distress by a factor of 3.6 compared to NP use.9,10 Polysomnographic studies have shown a better apnea-hypopnea index and better OS levels in TSS cases. 11 Therefore, TSS is considered a safer alternative for nasal surgery in the elderly population, as it minimizes the risks associated with the cardiovascular and respiratory systems.
The SCHNOS-O scale is a newly developed, user-friendly tool to measure nasal obstruction based on 4 nasal and respiratory parameters with a maximum score of 20. 12 In our study, we used this scale to assess the effectiveness of TSS and NP in septoplasty. The results indicated that TSS was equally effective as NP in alleviating nasal obstruction measured by the SCHNOS-O scale. Furthermore, the results of the rhinomanometric and spirometric measurements also showed that TSS was more effective and safer than NP. This supports the conclusion that TSS can be a better alternative to septoplasty, especially for patients with nasal obstruction who want to minimize the risk of complications and achieve better postoperative outcomes.9,13
However, the use of anticoagulants is prevalent among elderly patients. This may raise concerns regarding bleeding and hematoma in patients undergoing a TSS procedure. Although minor hemorrhages were observed on the first postoperative day in the group receiving TSS, such occurrences were found to be rare. They did not cause significant problems. Our study did not find severe bleeding problems associated with TSS. It is important to note that similar minor hemorrhages can occur after the removal of a NP.
Although there is conflicting evidence on the efficacy of nasal packing in preventing septal hematomas after septoplasty, our study found no cases of septal hematomas in either the NP or the TSS group.6-10,14 Although the small sample size of our study represents a significant limitation, a meta-analysis of 19 randomized controlled trials comprising 1845 cases indicated that TSS significantly reduced postoperative pain, headaches, and synechia formation compared to traditional nasal packing. 14
Both nasal packing and TSS yield similar results when considering postoperative bleeding, hematoma formation, septal perforation, infection rates, and persistent septal deviation. However, the use of TSS offers many benefits over traditional nasal packing, including reduced pain, headaches, respiratory distress, synechia formation, and improved patient satisfaction and quality of life. Given these advantages, TSS can be considered a suitable alternative to nasal packing in postnasal surgery operations. 14
Conclusions
In conclusion, the results of this study suggest that TSS is an effective, safe, and well-tolerated alternative to NP for elderly patients undergoing nasal surgery. The TSS procedure resulted in significantly lower postoperative pain scores compared to those reported by the patients in the NP-treated group and there were no significant differences in terms of septal hematomas. Using NP in elderly patients increases the risk of cardiovascular and respiratory distress, while TSS was shown to reduce these risks and improve postoperative OS levels. Furthermore, the SCHNOS-O scale and other measurements showed that TSS was as effective as NPs with regard to nasal obstruction and safety. The study had a low number of patients, which limited its findings. However, the results were supported by previous randomized controlled trials and meta-analyses that showed that TSS significantly reduces postoperative pain and improves patient satisfaction and quality of life. Overall, these findings suggest that TSS may be a safe and effective alternative to traditional nasal packing for elderly patients undergoing nasal surgery susceptible to surgical complications.
Footnotes
Acknowledgements
N/A.
Author Contributions
All authors contributed to planning and collecting the data, writing, and editing the manuscript.
Data Availability Statement
All available data were published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The ethical comity approval was obtained from the Baskent University Ethics Committee for Clinical Research (project no.: KA 22/13).
Informed Consent
There is no need for informed consent because the data were evaluated retrospectively.
Trial Registration Number/Date
N/A.
Grant Number
N/A.