
Abstract
Combined the big data from Chinese researches and our clinical experiences, we drew a concise “distributed map” of intractable epistaxis showing the concealed bleeding regions and offending vessels clearly (Figure 1). The bleeding site was located accurately according to the “distributed map,” and bleeding was stopped via bipolar radiofrequency ablation under nasal endoscope without nasal packing, followed by five classic cases (Figure 2). It is our recommended precise mode of diagnosis and treatment of refractory epistaxis.
Significance statement
Epistaxis is a frequently encountered otolaryngologic emergency, occurring in up to 60% of the general population, with one in ten of those affected seeking for medical attention.
1
In this paper, we focus on the intractable epistaxis, which refers to a large amount of blood gushing out from the front nose or oropharynx, but routine anterior rhinoscopy or nasal endoscopy can't identify the bleeding site, and even if nasal packing and transcatheter arterial embolization (TAE) is effective. Combined the big data from the databases including the China National Knowledge Internet and WANFAN MED ONLINE from 2009 to 2019 as well as our clinical experiences, finally, we drew a concise “distributed map” of intractable epistaxis showing the basis of the concealed bleeding areas and offending artery clearly. Figure 1 shows that frequency of bleeding regions appeared as follows: the vault of inferior nasal meatus in 3843 cases (31.58%), the olfactory cleft in 3606 cases (29.63%), the posterior areas of middle meatus in 1398 cases (11.49%), the districts of deviation of nasal septum (Little’s area) in 1094 cases (8.99%), the front of the nasal cavity in 775 cases (6.37%), and the others or uncertain in 1453 cases (11.94%) Finally, we drew an updated version “distributed map” of epistaxis on the basis of the hidden bleeding points and feeding artery based on our previous reports
2
(Figure 1). The distributed map and relevant offending vessels of concealed epistaxis.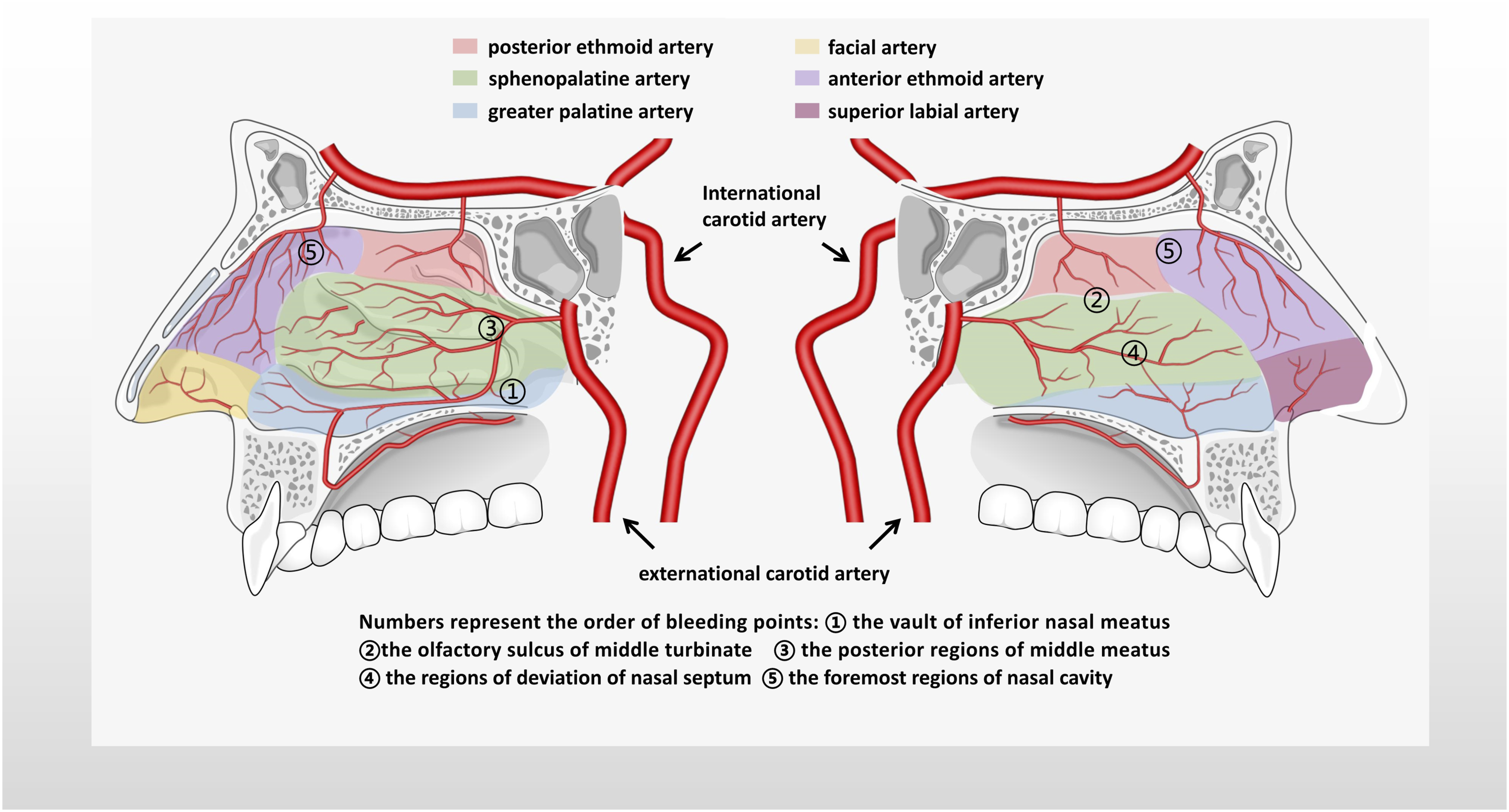
In addition, we summarized the optimal diagnosis and treatment of refractory epistaxis. The bleeding site was located accurately with the help of the “distributed map” and nasal endoscope, and then, bleeding was stopped via bipolar radiofrequency ablation without nasal packing, followed by five classic cases (Figure 2). They were referred by the lower-level hospital and were received and cured in our hospital. All of them were elderly patients with recurrent epistaxis. After repeated anterior and posterior nasal packing and even interventional embolization via external carotid artery and internal maxillary artery, both patients failed to stop bleeding in the county-level hospital, with a total cost of more than 30,000. At that time, the patient presented with a painful and anemic appearance because of anterior and posterior nasal packing. However, we quickly located the bleeding point under the guidance of our epistaxis map (Figure 1). Pictures of nasal endoscope of epistaxis in five cases (A1-C1. The left/right olfactory cleft is the bleeding point; D1-E1. The left/right the vault of inferior nasal meatus is the bleeding point; A2-E2. Stop bleeding effectively by bipolar radiofrequency under nasal endoscope).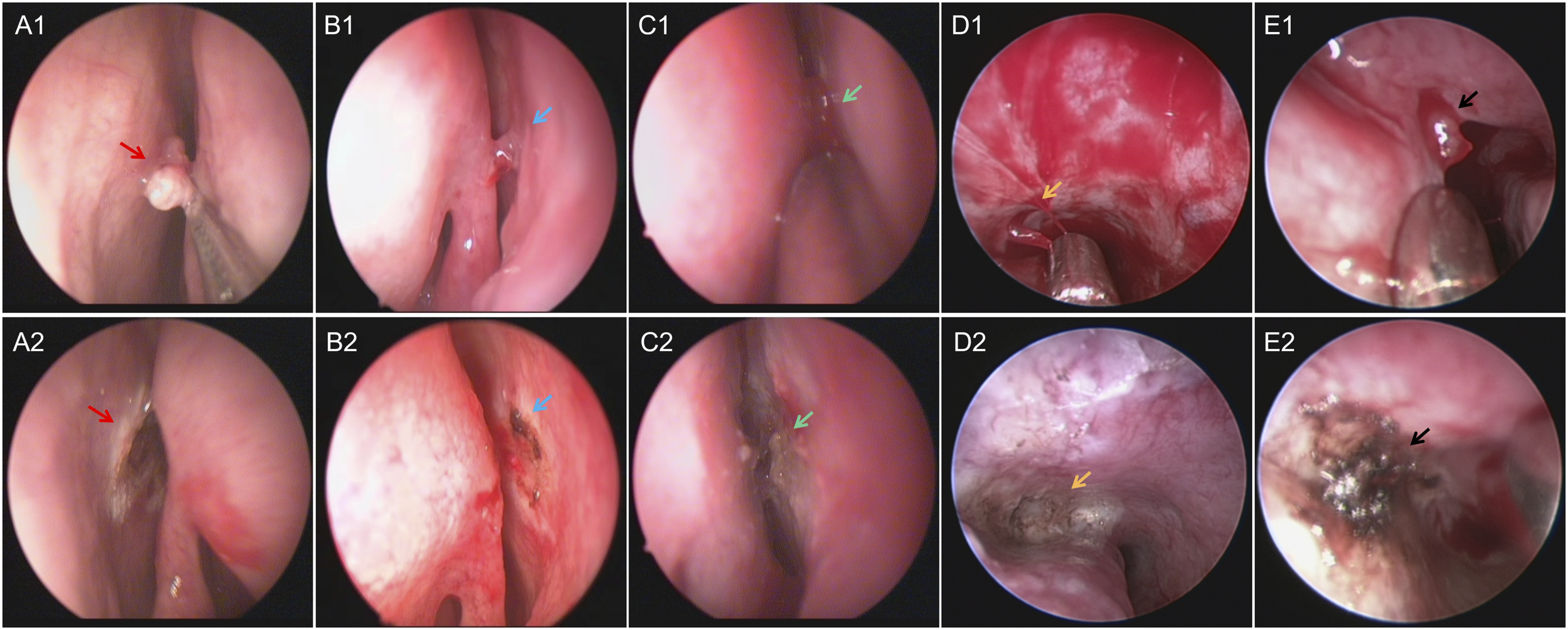
For epistaxis, nasal packing is still a common treatment in ENT emergency, especially in county hospitals. However, it not only brings great pain to patients but also has poor hemostatic effect, as well as serious complications such as nasal mucosal injury, nasal septum perforation, nasal alar injury, and so on. 3 Therefore, in accordance with Nikolaou G, 4 we strongly suggest that in the era of nasal endoscope and precision medicine, we should optimize the mode of diagnosis and treatment of epistaxis and focus on searching for bleeding sites in concealed areas based on the map. We search for bleeding sites under nasal endoscope and stop bleeding, so as to avoid nasal packing as far as possible and improve the quality of life of patients on the basis of improving the level of diagnosis and treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No. 82000957) and the Third Affiliated Hospital of Sun Yat-Sen University, Clinical Research Program (No. QHJH201901).