
Abstract
Parathyroid cysts (PC) are infrequently encountered and characterize less than 1% of all head and neck masses. When present, PCs may present as a palpable neck mass and lead to hypercalcemia and rarely respiratory depression. Furthermore, the diagnostics of PCs is difficult as they can masquerade as a thyroid or mediastinal mass given their proximity. PCs are theorized to be a progression of parathyroid adenomas and often routine surgical excision is sufficient for cure. To our knowledge, there is no documented report of a patient with an infected parathyroid cyst that led to severe dyspnea. This case describes our experience of a patient with an infected parathyroid cyst presenting as hypercalcemia and airway obstruction.
Introduction
Parathyroid cysts (PC) are rare pathologies representing 0.5–1% of parathyroid lesions and less than 1% of neck masses. 1 Clinical presentation of PCs may range extensively from asymptomatic neck masses, various levels of hyperparathyroidism and respiratory depression.2-4 PCs can be divided into two categories based on function: non-functional parathyroid cysts (NPCs) and functional parathyroid cysts (FPCs). It is estimated that 10–30% of PCs are functional, resulting in elevated parathyroid hormone (PTH) levels and hypercalcemia and are believed to be the result of pre-existing parathyroid adenomas that have undergone cystic degeneration. 4 In addition to hypercalcemia, parathyroid cysts may also present as a palpable neck mass that falsely mimics thyroid nodules. Ultrasound and fine-needle aspiration (FNA) biopsy have shown to be the primary diagnostic tools for preoperative diagnosis.2,4 While there is existing literature on the diagnosis and clinical course of patients with PC, there are no reports of a ruptured and infected PC that led to severe airway obstruction. This case aims to educate providers if they encounter a similar presentation in the future.
Case Presentation
A 59-year-old female patient with a past medical history of type II diabetes mellitus, transient ischemic attack and hypertension presented to an outside hospital emergency department with fever, non-pulsatile neck swelling and pain, ear drainage, hoarse voice, and severe shortness of breath. She was intubated due to respiratory depression and underwent needle aspiration of the neck mass which retrieved 300cc purulent fluid which was positive for Escherichia Coli. The patient was subsequently started on intravenous aztreonam and clindamycin and transferred to a tertiary care hospital where a contrasted computed tomography (CT) scan of the neck was performed. Imaging findings displayed large, multicystic, left anterolateral, thyroid masses measuring 4.7cm by 6.4cm with surrounding prevertebral inflammatory changes suggestive of a cystic lesion such as a thyroid cyst or a multinodular goiter (Figure 1). (A–C) CT soft tissue with contrast obtained in the axial plane (A–B) and sagittal plane (C) after aspiration illustrate a large rim-enhancing cystic lesion in the midline and left para midline lower neck suggestive of an infected solid and cystic lesion.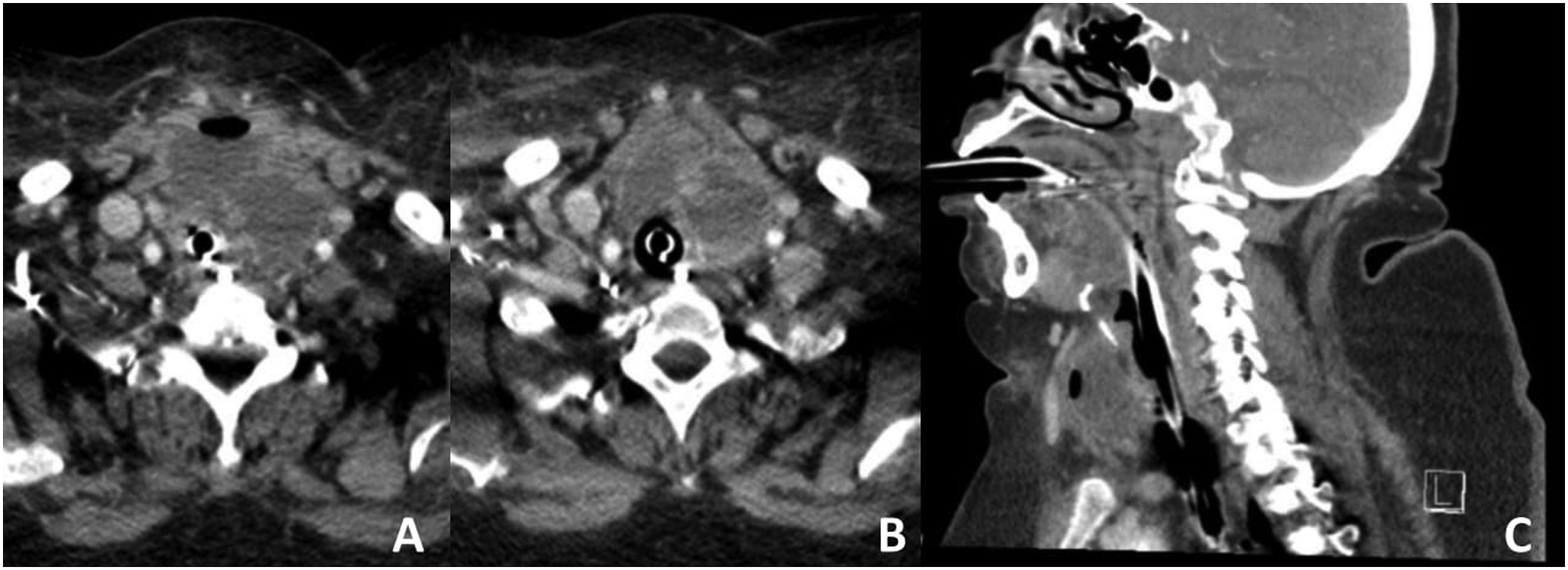
Upon transfer, her labs were significant for an ionized calcium level of 1.36, a calcium level of 9.9 (albumin correction to 11.3), and a PTH level of 455.8. These findings were highly suspicious of undiagnosed primary hyperparathyroidism. A total thyroidectomy along with excision of the attached cysts was performed for which an intraoperative frozen section of the excised specimen exhibited a ruptured infected cyst with the presence of parathyroid cells. Additionally, further exploration showed the left superior parathyroid was slightly enlarged and hypercellular which was removed. During the procedure, the left recurrent laryngeal nerve was transecting into the cyst and was clearly affected by the underlying pathological process necessitating sacrifice. Post-operatively, the PTH value dropped to 47.3 immediately and 38.5 the next day. She was extubated uneventfully and tolerated a diet. Her calcium values stabilized post-operatively and she was discharged without issue.
Histopathological analysis showed bilateral atypical parathyroid neoplasms with marked cystic degeneration along with inflammation, granulation tissue, fibrosis and adhesion to the thyroid lobe in the setting of mild chronic lymphocytic thyroiditis (Figure 2). Parafibromin staining was positive. She completed a four-day course of clindamycin and a 7-day course of aztreonam. She was prescribed levothyroxine and vitamin D daily. At follow-up, the patient was doing well without major concerns. She will be scheduled for a thyroplasty in the outpatient setting. (A) Histologic section shows a cystic atypical parathyroid neoplasm with no true epithelial cyst lining (Hematoxylin and Eosin (H&;E) stain; 20x); (B) Section shows parathyroid tissue in the background with focal bands of fibrosis (H&;E, 40x); (C) Section at high power magnification (H&;E; 100x) shows a cyst wall on the right which is composed of granulation tissue with neo-angiogenesis lined by reactive endothelial cells, plump fibroblasts, and mixed acute and chronic inflammatory infiltrate, and parathyroid acini on the left; (D) Immunostain section shows that parathyroid cells are positive for parathyroid hormone stain (brown chromogen; 100x).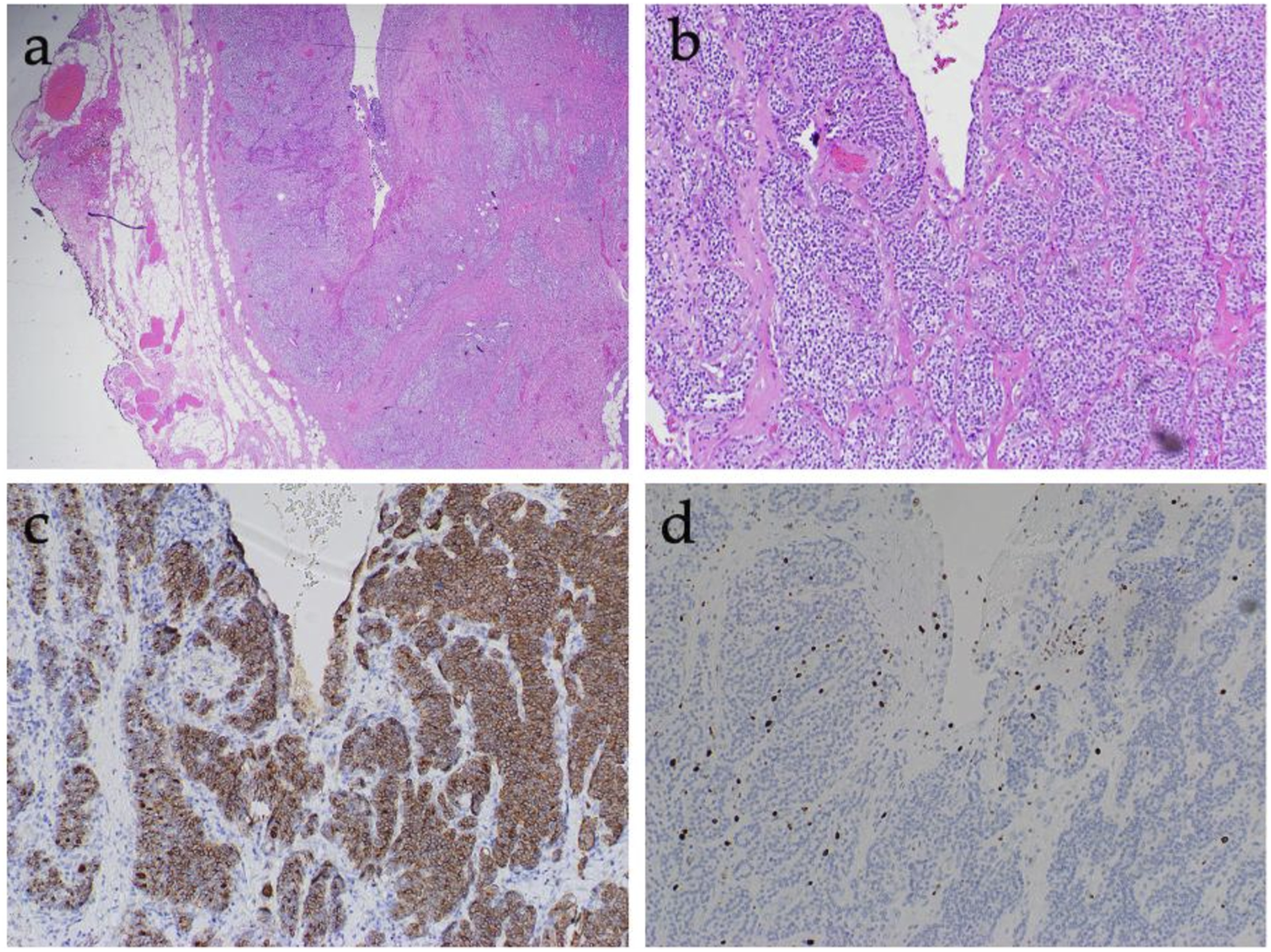
Discussion
Parathyroid cysts are a rare pathology that display a wide range of clinical presentations. If left untreated, PCs have the potential to cause life-threatening episodes of hypercalcemia and may lead to respiratory depression from their compressive effect on the trachea after reaching a large enough size.2-4 This report dictates the first patient with an infected, ruptured PC that necessitated preoperative intubation with definitive excision and adjuvant antibiotics
Parathyroid cysts represent a diagnostic dilemma due to their masquerading characteristics of a thyroid pathology. A major limitation of radiological imaging is their inability to differentiate PCs from other similarly defined neck lesions. To distinguish PCs, it is imperative to supplement radiological imaging with ultrasound and measurement of cystic-PTH levels via fine-needle aspiration. The most definitive way to confirm their diagnosis is intraoperatively using histopathological examination with immunohistochemical staining.2-5 In our case, the histologic section showed cystic atypical cells along with parathyroid tissue with fibrosis. These are features typically associated with FPCs. It is understood that FPCs arise when degeneration of a true parathyroid adenoma occurs. Our patient was never previously diagnosed with parathyroid adenoma making this an incidental finding. Moreover, positive parafibromin staining has demonstrated to be a confident rule out marker for parathyroid malignancy, with negative parafibromin staining occurring in malignant tumors.6-8 As such, a positive parafibromin stain was obtained for our patient suggesting a benign pathologic process.
Currently, there are no reports detailing the management of infected PCs. After a systematic review of literature, we discovered only a single presentation of a mediastinal PC leading to tracheal obstruction which did not necessitate preoperative intubation and was managed with a simple surgical excision. 4 Furthermore, in 2017, Igarashi et al detailed the treatment of a patient with an infected thyroid cyst. This patient's findings showed similar clinical features consisting of neck swelling and fever; and fine-needle aspiration drew purulent fluid from the cyst which revealed an infection of methicillin-resistant staphylococcus aureus (MSSA). 9 Like our patient, this infection was successfully resolved after intravenous antibiotic treatment along with surgical drainage of the cyst. 9 Surgical management combined with antibiotic treatment remains the mainstay course of action for treating patients with infected parathyroid cysts.
Our report adds to the paucity in literature detailing the possibility for acute airway obstruction and hypercalcemia due to infection and rupture of a parathyroid cyst. It illustrates the importance of early recognition and treatment to decrease the morbidity caused by this extremely rare phenomenon.
Conclusion
This case describes the importance of maintaining an unbiased approach and methodically dealing with cysts within the head and neck region. We share our experience of successfully diagnosing and treating this rare pathology presenting as hypercalcemia and airway obstruction.
Footnotes
Author Contributions
SHAN, PH, DA, and SHSN drafted the manuscript. ETR, KS, and RJK contributed to data acquisition and revised the manuscript. SHAN, PH, DA, and AE edited the manuscript. All authors reviewed and approved the final manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Materials
All data and materials used for this case report are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All clinical specimens were obtained under the approval of the Institutional Review Board. Informed consent was obtained from the subject.
Consent for Publication
Informed consent was obtained from the patient for publication of this case report. A copy is available upon reasonable request.