
Abstract
Acinic cell carcinoma (AciCC) is a low-grade, slow-growing malignant tumor that commonly originates from the parotid gland and occasionally from the minor gland of the oral cavity, but rarely from the nasal cavity. Here, we present a 57-year-old woman who presented with an 8-month history of obstruction and epistaxis of the right nasal cavity. Rhinoscopy revealed a reddish-gray fleshy mass with tiny blood vessels on the surface blocking the right postnaris. Computed tomography showed a 3 × 2 cm2 well-demarcated tumor filling the right nasal common meatus with a clear boundary. There were no signs of local bone erosion in the bony window. Magnetic resonance imaging revealed abnormal signals in the nasal meatus with iso-intensity in the T1W1 sequence with homogeneous enhancement. We diagnosed it as a right nasal hemangioma, and the patient underwent endoscopic resection. However, histopathological evaluation of the surgical specimen confirmed a primary AciCC. The patient refused further radical surgery and instead underwent adjuvant radiotherapy. There was no clinical evidence of recurrence for 2 years, and the patient has returned for follow-up yearly. We discuss the clinical nature of sinonasal AciCC and the treatment of this rare condition.
Introduction
Acinic cell carcinoma (AciCC) develops mainly in the salivary gland as a painless mass or nodule and usually affects middle-aged adults. The parotid gland is the most commonly affected site, with AciCC accounting for 10% of all parotid malignancies. 1 However, it also occasionally affects the minor salivary glands, oral cavity, sinonasal cavities, and orbit. 2 The development of AciCC in the sinonasal cavity is rare, with approximately 20 cases reported in the English literature.3 -6 Consequently, the clinical behavior, diagnostic features, and prognosis of this tumor remain unclear. We report a case of nasal septal AciCC that was misdiagnosed as a nasal hemangioma to clarify the clinical nature of AciCC and its treatment options.
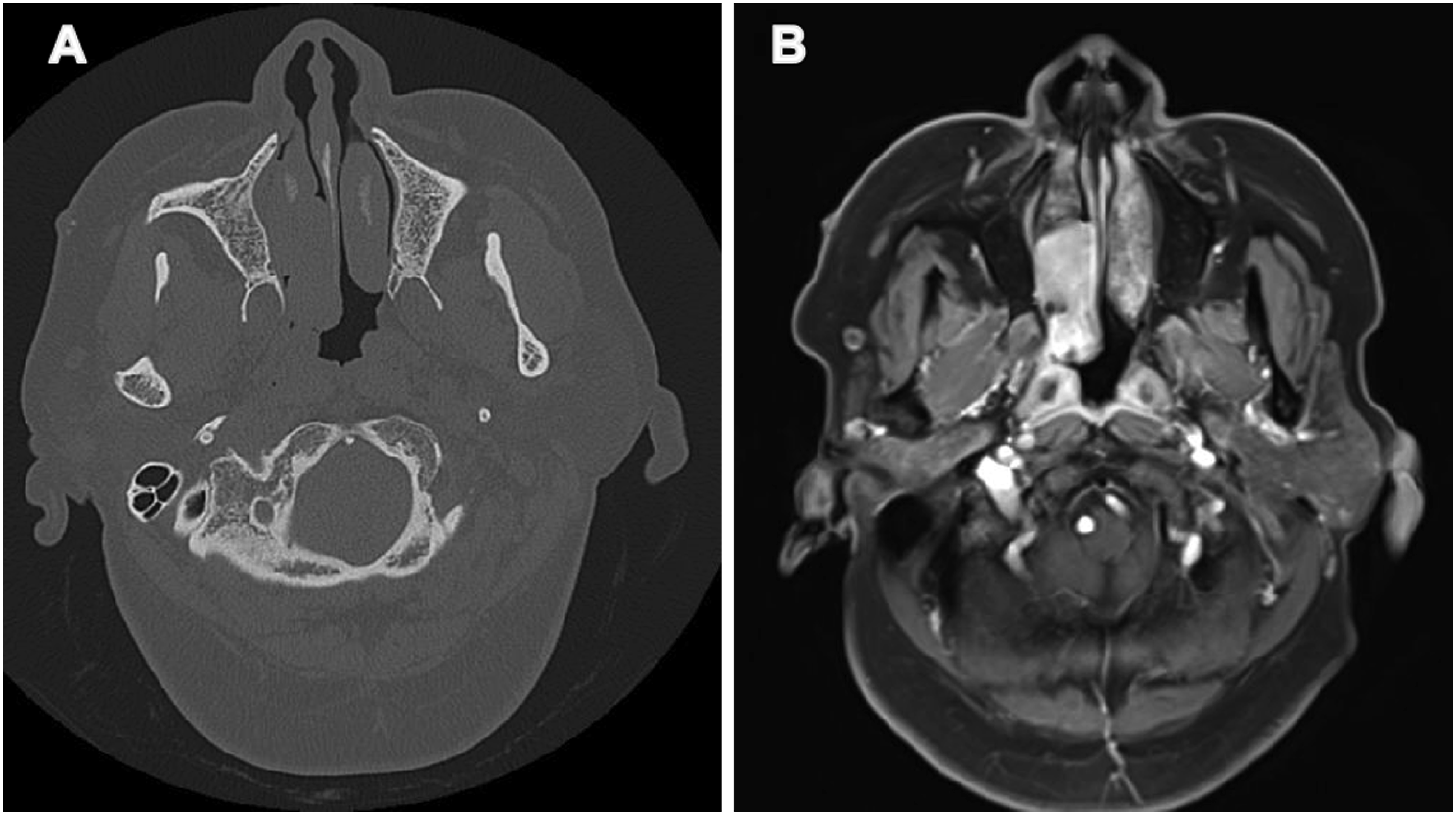
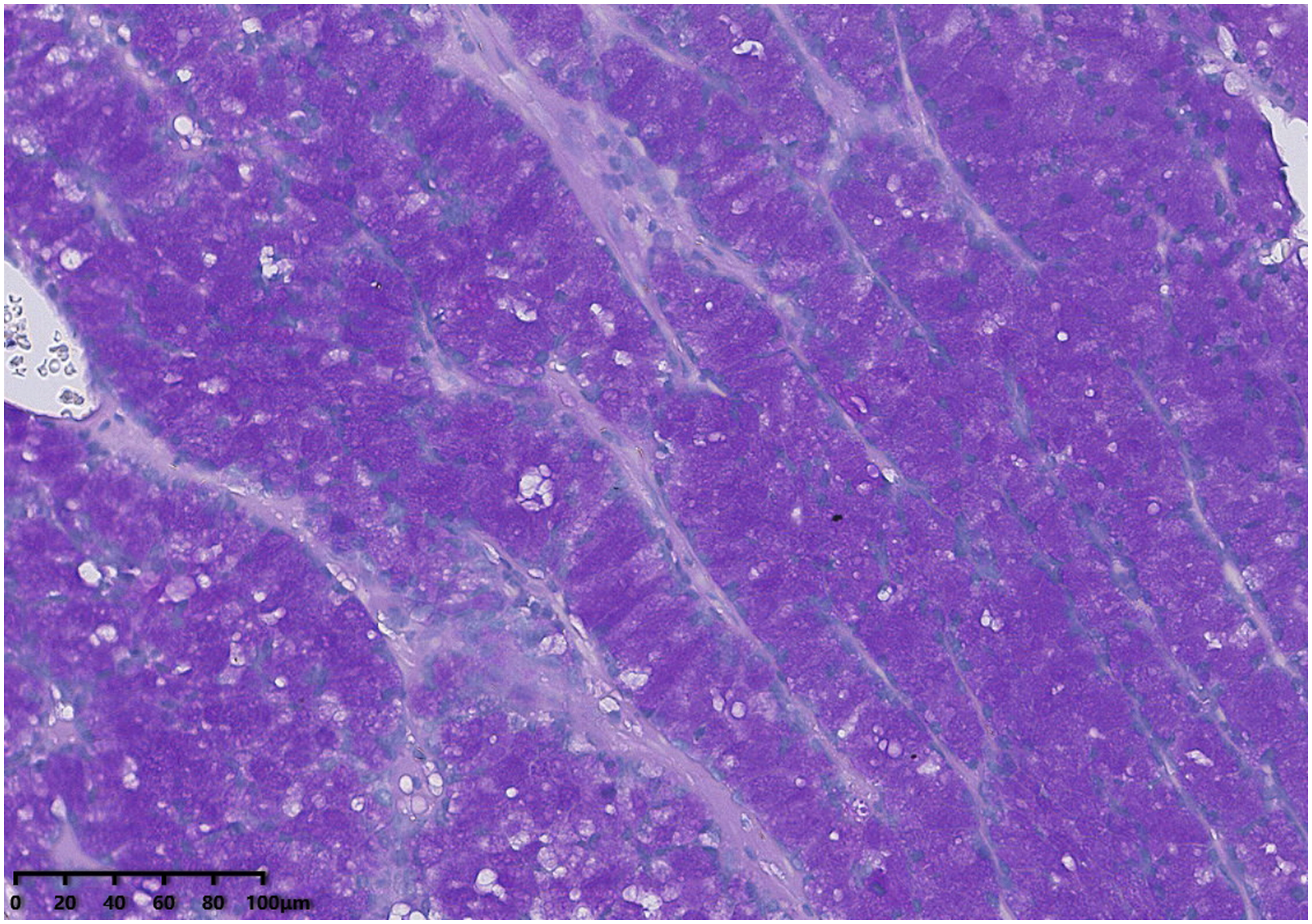
A 57-year-old woman was admitted to the Department of Otolaryngology, Head and Neck Surgery, with an 8-month history of obstruction and epistaxis of the right nasal cavity. She had a 10-year history of hypertension and performed meditation regularly. She stated that the epistaxis had become more severe recently but reported no rhinorrhea or rhinogenic headache. There were no signs of intraorbital or intracranial invasion. Her laboratory parameters were normal. Rhinoscopy revealed that the right nasal cavity was obstructed by a reddish-gray fleshy mass with tiny blood vessels lying on the surface blocking the right postnaris. Computed tomography showed a 3 × 2 cm2 well-demarcated tumor with a clear boundary filling the right nasal common meatus. There were no signs of local bone erosion in the bony window. Magnetic resonance imaging revealed abnormal signals in the nasal meatus with iso-intensity in the T1W1 sequence with homogeneous enhancement. Our initial diagnosis was a right nasal hemangioma, and the patient underwent endoscopic resection. Rhinoscopy revealed that the lesion originated from the middle part of the nasal septum. The turbinates and septal cartilage were not infiltrated. The lesion was removed completely, with no residue in the deeper cartilage and no excessive bleeding. Paraffin section histology revealed a primary AciCC. The tumor cells resembled the polyhedral cells of normal acini and contained abundant, finely granular basophilic cytoplasm. The nuclei were generally small and hyperchromatic. Mitoses were absent. Periodic acid–Schiff diastase-resistant granules were seen.
Immunohistochemical staining was positive for S-100, α-AT, DOG-1, and Ki-67 and negative for CK, P63, and mammaglobin.
The patient refused further surgical treatment but did undergo radiotherapy in the oncology department. There has been no evidence of recurrence for 2 years, and the patient has returned for follow-up yearly.
Discussion
Acinic cell carcinoma is a low-grade, slow-growing malignant tumor that commonly originates from the parotid gland and occasionally from the minor gland of the oral cavity, but rarely from the nasal cavity. 2 The etiology and pathogenesis of sinonasal AciCC remain unclear. This is the third report in the English literature of an AciCC of the nasal septum. In our case, the tumor showed obvious uniform enhancement on CT and MRI. Since the patient had multiple episodes of epistaxis and no invasive signs on imaging, we misdiagnosed it as a nasal hemangioma preoperatively, partly because such tumors derived from the salivary glands or at an early stage may not show the characteristic bone destruction. Nasal hemangiomas consist mostly of a capillary plexus or blood sinusoids of different sizes, and most lesions show uneven enhancement or irregular progressive enhancement on MRI, in contrast to our case. 7
Sinonasal AciCC has low malignancy with 5- and 10-year overall survival (OS) rates of 84.3% and 72.2%, respectively.
8
Radical surgical excision has been the primary treatment for all AciCC cases. The only controversy is whether postoperative radiation should be administered. In the Surveillance, Epidemiology, and End Results database, Biron et al. found that surgery alone or surgery with postoperative radiotherapy had no significant effect on survival.
6
Kshirsagar et al used the National Cancer Database to investigate patient factors associated with survival outcomes. Their results suggested that older age and primary sphenoid sinus disease are associated with a worse OS, and adjuvant radiation had no apparent survival benefit, probably due to the small sample size.
8
Treatment recommendations remain difficult. Yoshihara et al reported one case that was initially diagnosed as parotid cancer that responded well to radiotherapy and systemic chemotherapy.
9
Based on their experience, considering the unclear resection margins in our case, we recommended that the patient undergo radiotherapy. Currently, our patient has had no recurrence for 2 years. We advocate postoperative radiotherapy for patients with recurrent disease, high-grade pathology, positive margins, and advanced tumors with cervical lymph node metastasis (Figures 1 to 3). Endoscopic appearance of nasal septal acinic cell carcinoma. (A) Noncontrast computed tomography with right nasal mass. (B) Coronal T1-weighted postcontrast MRI. MRI = magnetic resonance imaging. Photomicrographs of histology slides showing well differentiated acinar cells in a solid growth pattern, with infrequent mitoses. The cytoplasm is granular and lightly basophilic; nuclei are eccentrically positioned. (H&E, 200X)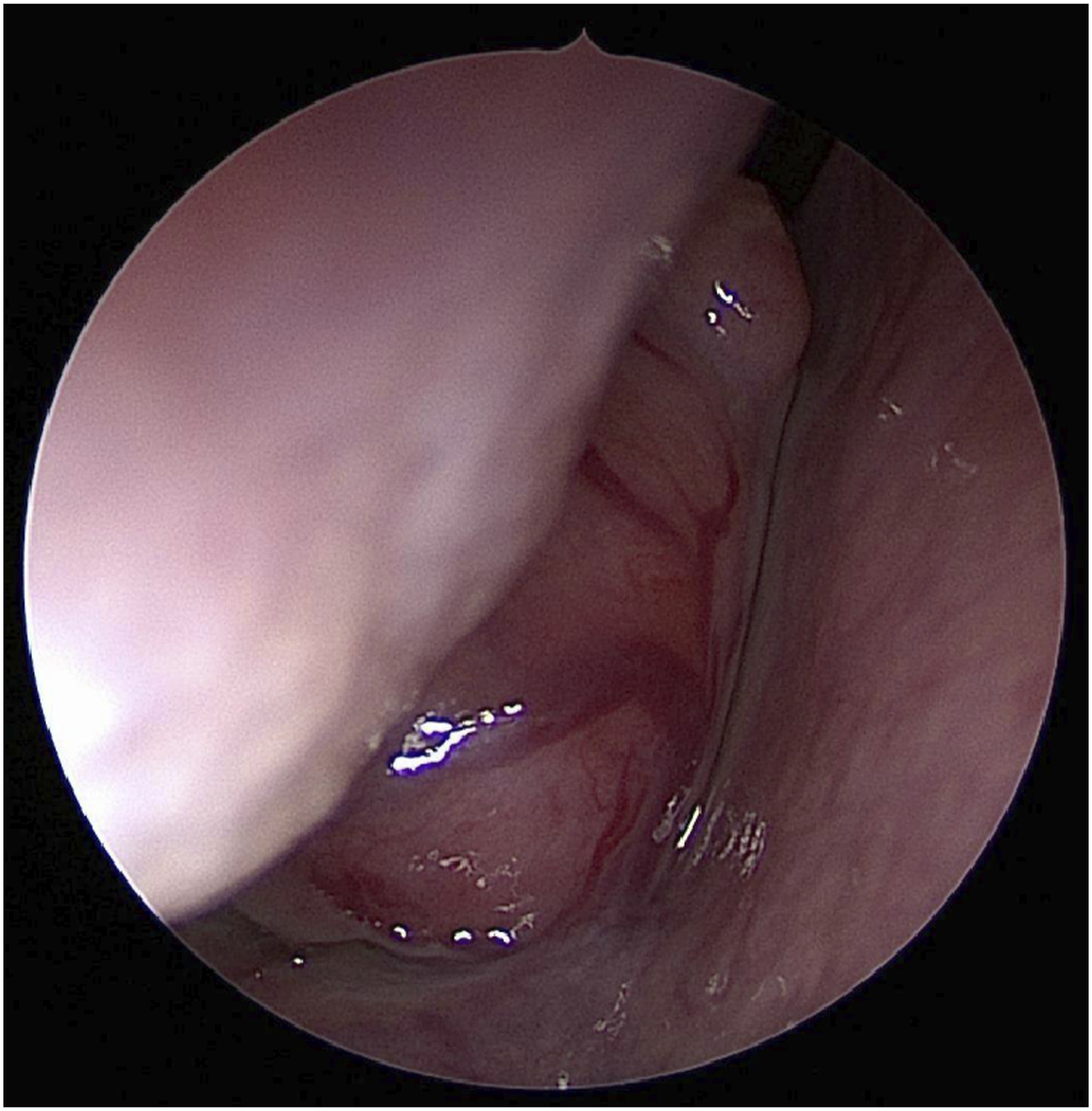
Conclusion
This case report presents a rare nasal septum AciCC, highlighting the imaging findings and immunohistochemical diversity of this uncommon nasal mass. Some unilateral nasal masses with no bone destruction on endoscopic or imaging examinations are still potentially malignant. In suspicious cases, fast-frozen pathology or preoperative biopsy should be considered to avoid misdiagnosis. Pathologists and surgeons should be aware of this salivary gland carcinoma in the sinonasal tract.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by Central Funds Guiding the Local Science and Technology Development (grant number: 20221ZDG020066)
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.