
Abstract
Background:
Acinic cell carcinoma (AciCC) is a relatively rare malignancy of the salivary glands, predominantly affecting the parotid gland. Recent studies report that the local recurrence rate for AciCC ranges from 5% to 17%, while metastasis occurs in 2% to 12% of cases. Most recurrences or metastases are observed within the first 5 years following initial therapy. However, late recurrences or metastases occurring more than 10 years have been reported in rare cases.
Methods:
This study presents 13 cases of AciCC in which patients experienced recurrence or metastasis 10 to 45 years after initial treatment. The case series includes 6 patients identified from our database and 7 cases from a literature review.
Results:
In this small series, late recurrence or metastasis appeared more common in female patients. Four patients experienced recurrence confined to the tumor bed, with or without regional lymph node involvement. Seven patients developed distant metastases, while 2 experienced both local and distant diseases. The lungs, bones, and skin were the most common sites of distant metastases. Management predominantly involved surgical resection of the recurrence, often followed by radiation therapy. Two patients also received chemotherapy for distant metastases. Follow-up data were available for 11 patients: 2 succumbed to the disease, 1 died of an unrelated condition, and 8 remained alive.
Conclusions:
Diagnosing late-onset recurrence or metastasis of AciCC poses a unique challenge, as the primary tumor may have occurred decades earlier. Further research is needed to deepen our understanding of the clinical course and adjust clinical follow-up strategy.
Introduction
Acinic cell carcinoma (AciCC) of the salivary gland is a relatively rare malignant epithelial neoplasm, accounting for about 10% to 15% of salivary gland malignancies and 2% to 6% of all salivary gland neoplasms.1,2 It arises primarily from acinar cells and exhibits serous acinar differentiation. About 85% to 90% of AciCC affects the parotid gland with rare occurrence in the submandibular gland, 2 intraoral sites, 3 sinonasal tract, 4 and larynx. 5 Clinically, most patients present with a slow-growing, painless mass, although high-grade transformation may result in a rapidly growing tumor fixed to adjacent structures, causing facial nerve paralysis. Histologically, AciCC demonstrates a diverse array of patterns, including solid, microcystic, and papillary-cystic structures, 6 with tumor cells characterized by cytoplasmic zymogen secretory granules. Diagnosis of cases with unusual morphology or high-grade transformation may require immunohistochemical staining sometimes molecular studies. Treatment typically involves surgical excision, supplemented with adjuvant radiotherapy7,8 based on stage and risk factors. Prognosis is generally favorable for early-stage cases but may worsen with high-grade transformations or advanced disease.1,7
The local recurrence rate for AciCC varies widely, from 5% to 60%. Reports from the 1970s to 1990s commonly cited rates of 30% to 50%,7,9,10 likely due to the management of some tumors with enucleation. More recent studies have reported local recurrence rates ranging from 5% to 17%, with metastasis affecting 2% to 12% of patients.11 -16 Although recurrences typically occur within the first 5 years postsurgery, rare cases of delayed recurrence or metastases have been reported more than 10 years after initial treatment.7,9,17 Many of these cases were reported in cases series from 1970s to 1990s. The clinical and pathological features of these cases are often poorly documented or entirely absent, making it challenging to evaluate the pathological characteristics associated with this rare behavior. In this study, we present 6 cases of AciCC with local recurrence and/or metastasis occurring over 10 years after primary treatment. Clinicoradiologic and pathological findings from these patients are summarized. Additionally, we conducted a literature review to analyze and summarize case reports documenting similar phenomena.
Methods
This study was approved by our Institutional Review Board (protocol number 23429). We conducted a search in our database for all AciCC cases with late-onset recurrence or metastasis, covering the period from January 2000 to December 2024. This search yielded 6 cases, which are summarized in Table 1. Late recurrence was defined as disease recurrence occurring more than 10 years after the initial diagnosis. Recurrence included local relapse at the tumor site, metastasis to regional lymph nodes, or distant organ involvement. Only cases with pathologically confirmed recurrences were included in the analysis. Data on clinical presentation, pathological features, and radiologic findings were collected.
Clinical and Pathological Information of All Cases From Our Institute.
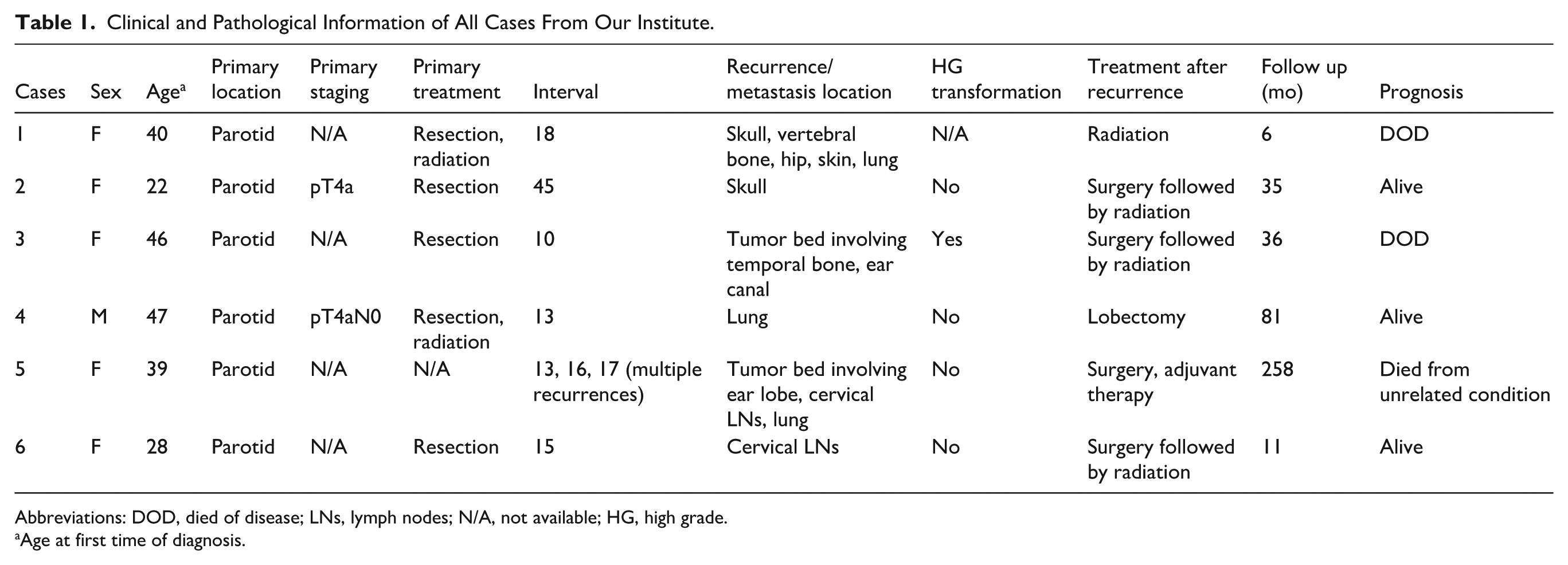
Abbreviations: DOD, died of disease; LNs, lymph nodes; N/A, not available; HG, high grade.
Age at first time of diagnosis.
Additionally, we performed a literature search using the keywords: “acinic cell carcinoma,” “delayed or late recurrence,” and “metastasis” to identify relevant case reports. This search identified 7 cases, which are summarized in Table 2. Cases from large series that lacked detailed clinical and/or pathological information were excluded from the review.
Summary of Case Reports on Late Recurrence/Metastasis of Acinic Cell Carcinoma.
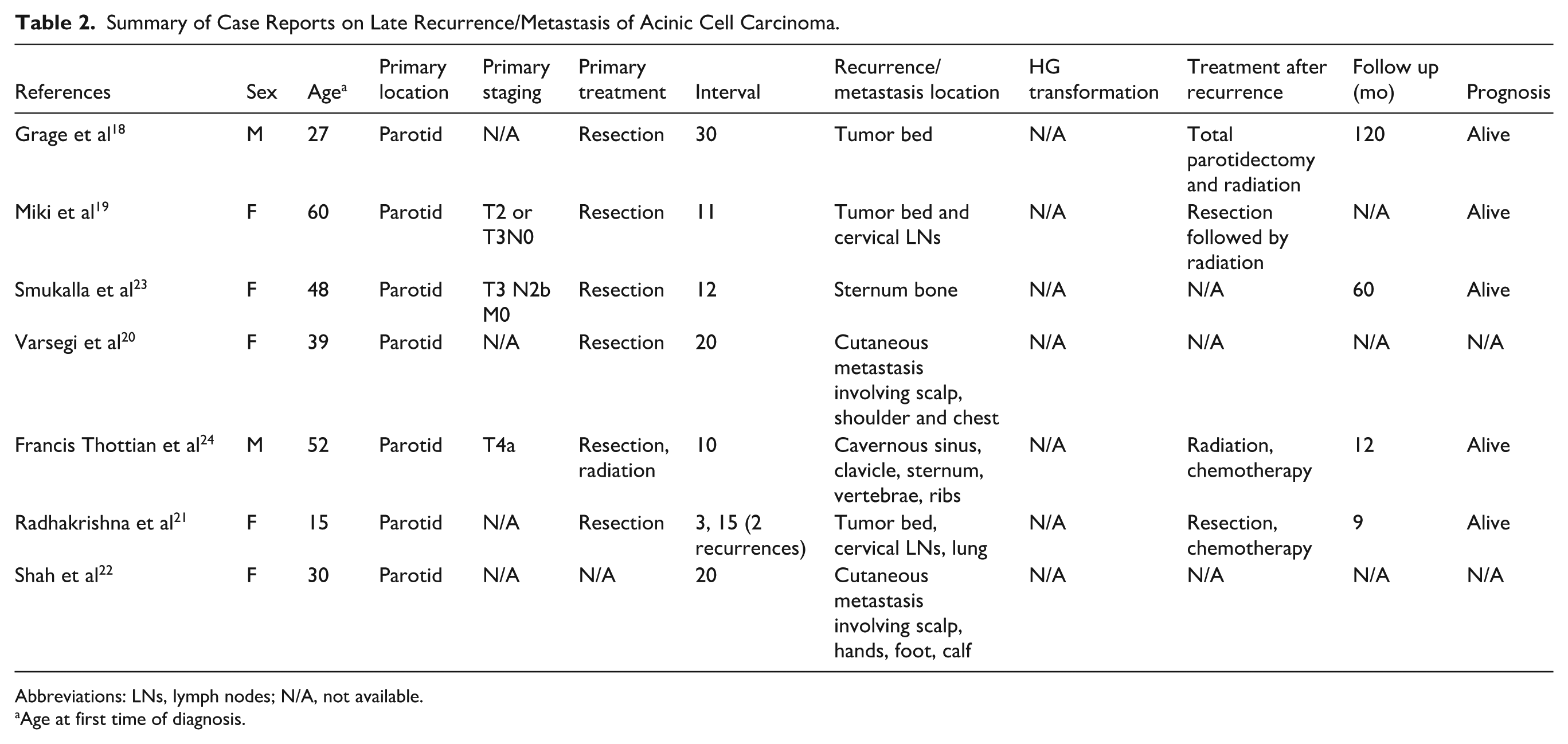
Abbreviations: LNs, lymph nodes; N/A, not available.
Age at first time of diagnosis.
Results
Cases From Our Database
A total of 6 patients were identified, consisting of 5 females and 1 male. At the time of their initial diagnosis, the patients’ ages ranged from 22 to 47 years (Table 1). All primary tumors were located in the parotid gland. Primary tumor staging was available for 2 patients, both of whom had facial nerve involvement (T4a). Two patients underwent radiation therapy following primary tumor resection. The interval between the primary diagnosis and the first recurrence ranged from 10 to 45 years. One patient experienced 3 recurrences at intervals of 13, 16, and 17 years.
Two patients developed recurrence in the prior tumor bed along with regional cervical lymph node metastases. Three patients presented with distant metastases alone, occurring after an interval of 10 years. The final patient experienced both regional recurrence and distant metastases. The most common site of distant metastasis was the lung (3 patients), followed by bone (2 patients) and skin (1 patient). Figure 1A shows an magnetic resonance imaging (MRI) from patient 2, demonstrating a 3.6 cm expansile and lytic mass involving the right frontal calvarium. For patient 4, computed tomography (CT) and positron emission tomography (PET-CT) imaging revealed a 1.5 cm nodule in the inferior medial aspect of the right upper lobe with mild-to-moderate FDG uptake (Figure 1B and C).
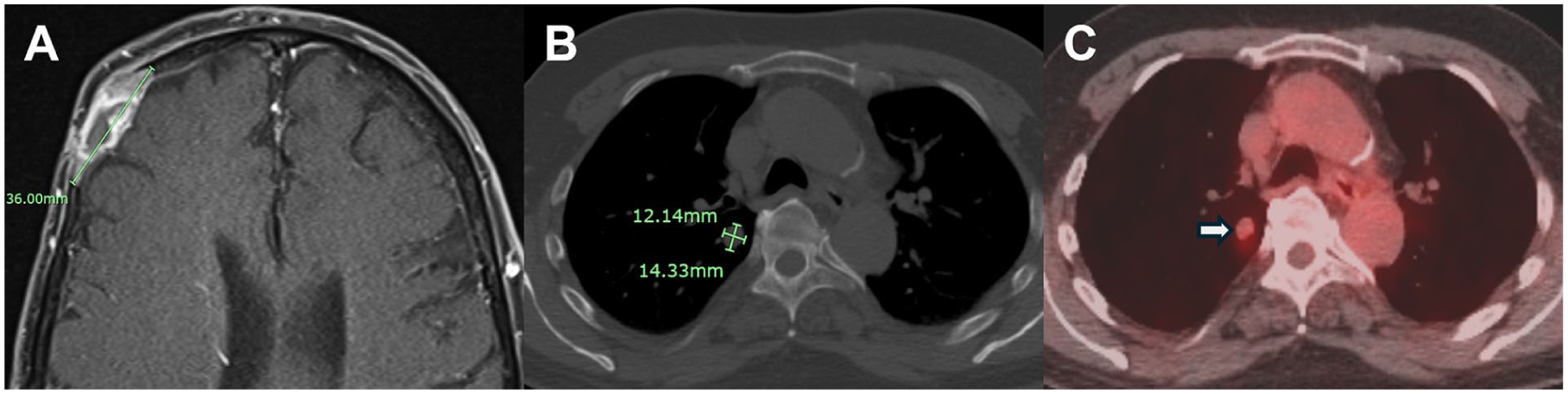
Radiologic findings for patient 2 and 4. (A) MRI demonstrated an expansile and lytic mass measuring up to 3.6 cm involving the right frontal calvarium. (B, C) CT revealed a 1.5 cm nodule in inferior medial aspect of right upper lobe with mild to moderate increased FDG uptake.
Histology from recurrence/metastasis was available in 5 of the 6 cases. The remaining case was an external consultation, and the slides were no longer accessible. All recurrences were confirmed by biopsies: 4 through fine-needle aspiration (FNA), and 2 by core biopsies. On FNA smears, AciCC demonstrated loosely cohesive tumor cells with round nuclei and pale cytoplasm (Figure 2A and B). Intracytoplasmic basophilic zymogen granules were typically absent on cell blocks but were highlighted by periodic acid-Schiff with diastase (PASD) resistance staining (Figure 2C). These granules were more distinctly visualized in H&E-stained sections from formalin-fixed paraffin-embedded blocks (Figure 2D). DOG1 immunohistochemistry served as a marker for AciCC, showing a mixed pattern of apical membranous, cytoplasmic, or complete membranous staining (Figure 2F). High-grade transformation was observed in 1 case (patient 3). Histology revealed solid sheets of tumor cells with necrosis and increased mitotic figures. Basophilic zymogen granules were poorly appreciated (Figure 2G–I).
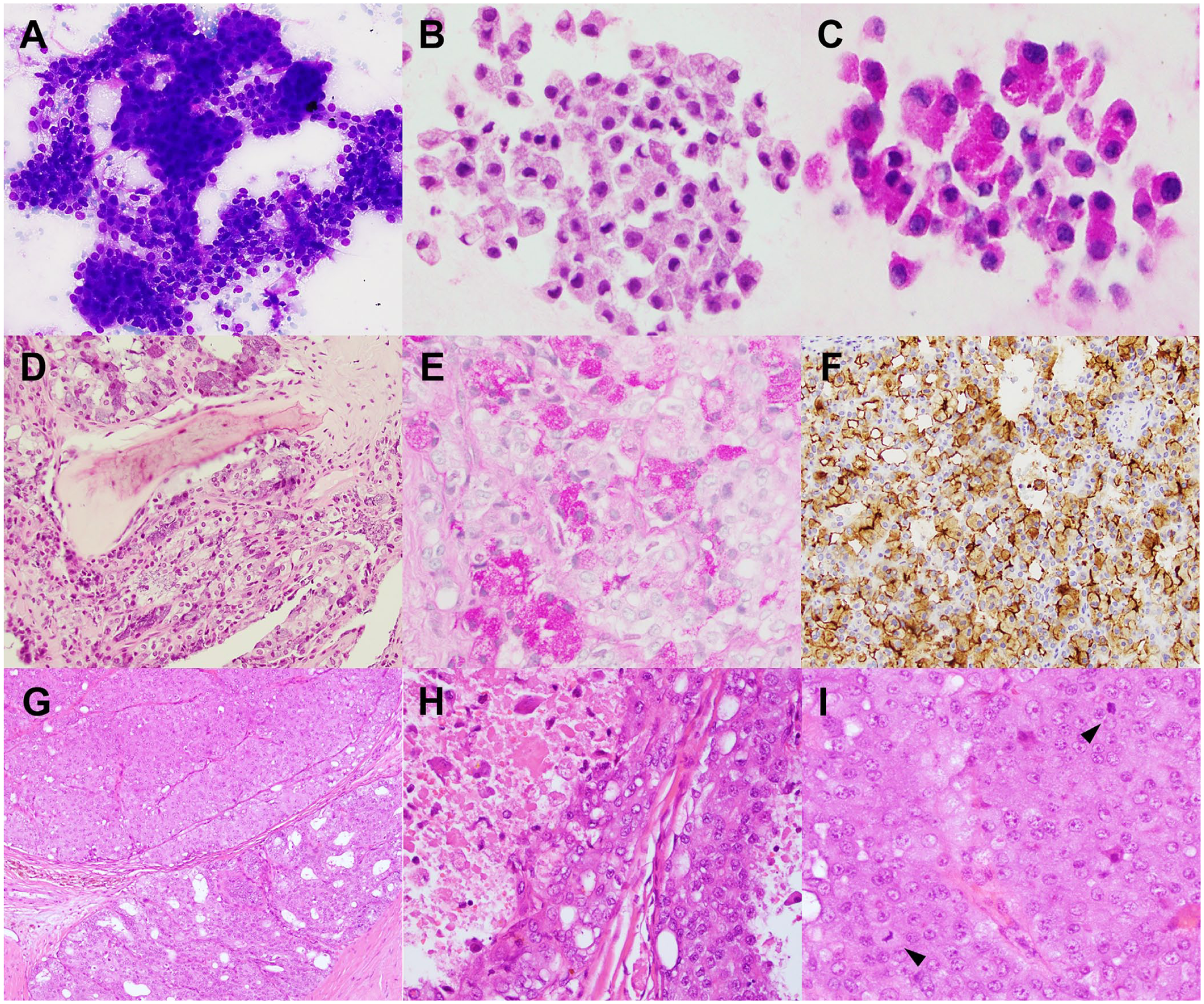
Histology and cytomorphology for patients 2 and 3. (A, B) Fine needle aspiration from the parotidectomy tumor bed showed clusters of tumor cells with round nuclei and pale cytoplasm. (C) PASD staining highlights intracytoplasmic zymogen granules. (D, E) Recurrent acinic cell carcinoma involving skull bone demonstrated basophilic intracytoplasmic zymogen granules on H&E section (D) and PASD staining (E). (F) Tumor cells were positive for DOG1. (G–I) Histology of acinic cell carcinoma with high-grade transformation for patient 3. Tumor cells formed solid nests or microcysts (G) with areas of necrosis (H), and increased mitotic activity (I, arrowhead). PASD, periodic acid-Schiff with diastase.
For the treatment of recurrent or metastatic disease, 4 patients underwent surgery followed by radiation and/or chemotherapy. One patient received palliative radiation due to widespread disease, while another underwent a lung lobectomy but declined postsurgical adjuvant therapy. During follow-up, 2 patients died of disease 6 or 36 months after recurrence. Three patients remained alive, with follow-up durations ranging from 11 to 81 months. One patient died of an unrelated condition.
Literature Review
A literature search using the keywords “late,” “recurrence,” “metastasis,” and “acinic cell carcinoma” identified 7 patients, comprising 5 females and 2 male (Table 2).18 -24 The age at the initial diagnosis ranged from 15 to 60 years, with all primary tumors located in the parotid gland. Pathological or clinical staging information was available for 3 patients.19,23,24 The interval to late recurrence varied from 11 to 30 years. One patient experienced 2 recurrences, 21 with the first occurring 3 years after surgery. Two patients had recurrences confined to the tumor bed, with or without regional lymph node metastases.18,19 Four patients developed distant metastases, 2 involving bone23,24 and 2 presenting with widespread cutaneous metastases affecting multiple sites.20,22 One patient experienced both regional recurrence and distant lung metastasis. 21 Follow-up information was available for 5 patients,18,19,21,23,24 all of whom were alive, with follow-up durations ranging from 9 to 120 months.
Discussion
Late on-set of recurrent or metastasis of AciCC is a rare phenomenon, with the exact percentage of cases remaining unknown. In a study by Ellis et al 25 involving 294 cases, 82% of recurrence and metastasis occurred within the 5 years of initial therapy. Batsakis et al 26 reviewed 35 patients with AciCC, 55% (16/29) experienced local recurrence. Of these, 14 cases reoccurred within the first 5 years, while 2 patients had recurrence between 5 and 9 years post-treatment. No recurrence was observed beyond 10 years in this series. In another study involving 37 cases, 17 all 11 patients with local recurrence occurred with the first 6 years. Among 9 cases of distant metastasis, 3 were reported more than 10 years after the initial therapy. Based on these findings, the estimated rate of late recurrence or metastasis in AciCC is likely between 5% and 10%.
In our cases and literature review, late recurrence or metastasis was more common in females, with a female-to-male ratio of 3.33. This is notably higher than the reported female-to-male ratio for AciCC in large-scale demographic studies, which ranges from 1.4 to 1.6. However, given the limited number of cases, this finding requires confirmation through larger-scale investigations. The patient’s age ranged widely from 16 to 60 years, and all primary tumors were located in parotid gland. Although detailed pathological information for most primary tumors was unavailable due to the remote initial presentation, 4 cases were pathologically staged as III or IV, with facial nerve involvement in 3 patients. Two other patients received radiation following primary tumor resection. These findings suggest that locally advanced disease may have a higher likelihood of developing late recurrence or metastasis. The association between high-grade transformation and late recurrence remains unclear, as detailed pathological characteristics of the initial tumor are unavailable for most cases. In our series, only 1 case exhibited high-grade transformation.
The interval from initial treatment to late recurrence ranged from 10 to 45 years, highlighting the need for prolonged follow-up in patients with AciCC. In this small series, 4 patients experienced recurrence confined to tumor bed, with or without regional lymph nodes metastasis. Seven patients developed distant metastasis, and 2 patients experienced both. The most common sites of distant metastasis were the lungs, bones, and skin. Most cases were managed with surgical resection of the recurrence, followed by radiation therapy. Two patients also received chemotherapy for distant metastases. Follow-up information was available in 11 patients: 2 died from the disease, 1 died from unrelated condition, and 8 were still alive.
When AciCC recurs or metastasizes after more than 10 years, the diagnosis can be challenging due to the relative rarity of this tumor and the possibility that patient may not recall the details of their primary malignancy, which occurred in the distant past. Immunohistochemical staining such as DOG1, Sox10 and the relatively new nuclear marker NR4A3 are valuable tools for aiding diagnosis. 6 PASD staining, which highlights intracytoplasmic granules, can also be helpful in cell block preparation, especially when zymogen granules are poorly visualized due to fixation medium used for cytology specimens. While molecular studies are not typically required for diagnosis, they can be useful in differentiating AciCC from secretory carcinoma in cases where immunostains are inconclusive. Translocation involving NR4A3 have been identified in 86% of AciCC, 27 whereas ~90% of secretory carcinomas harbor a chromosomal rearrangement, t(12;15)(p13;q25), resulting in an ETV6::NTRK3 fusion. 28
In a study by Chen et al 29 involving 145 patients treated for localized salivary gland carcinoma, 19% of those initially disease-free experienced a recurrence. The estimated 10 and 15 year cumulative probabilities of late recurrence were 13% and 18%, respectively. Adenoid cystic carcinoma had the highest rate of late recurrence (26%), followed by mixed malignant tumor—now termed carcinoma ex pleomorphic adenoma (25%), mucoepidermoid carcinoma (17%), adenocarcinoma (10%), and AciCC (8%). Earlier studies from the 1970s9,30 reported that the cure rate for AciCC declined from 76% to 78% at 5 years to 44% to 55% at 15 years, suggesting a prolonged clinical course and that late recurrence may contribute to decreased long-term survival. These findings support the need for lifelong follow-up in this patient population.
Conclusions
In this study, we reported 6 cases of late on-set recurrence or metastasis of AciCC and reviewed previously reported cases in the literature. Awareness of this phenomenon is crucial to avoid potential diagnostic errors. However, the study is limited by the small case volume and the lack of original pathological information for most patients, which make it challenging to pinpoint pathological features associated with late recurrence. We hope this study encourages further documentation in the literature to better identify patients at risk for late recurrence and emphasize the importance of prolonged follow-up.
Footnotes
Author Contributions
Design, data analysis, manuscript draft, table, and figures: C.B., T.H.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Indiana University Medical Student Program for Research and Scholarship (IMPRS) for C.B.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated in this study are available from the corresponding author upon reasonable request.