
Abstract
External auditory canal adenoid cystic carcinoma (EAC) is rare and is associated with nonspecific clinical manifestations such as early ear pain. We report a patient with advanced lung metastases from adenoid cystic carcinoma (ACC) of the EAC, which is difficult to diagnose. Under general anesthesia, lengthened right temporal bone resection, parotidectomy, facial nerve resection, cervical lymph node dissection (I-III), partial mandibular resection, tumor resection in the inferior temporal fossa and lateral femoral flap repair were performed, followed by regular radiotherapy and chemotherapy. During 2 years of postsurgical follow-up, there was no recurrence. The combination of early detection, resection, postoperative radiotherapy, and chemotherapy can result in a good therapeutic effect.
Keywords
Background
Adenoid cystic carcinoma (ACC) of the external auditory canal (EAC) is a rare tumor in clinical practice. Primary cancer of the EAC is rare, with squamous cell carcinoma accounting for the majority of cases (80%) and ACC accounting for 5%.1,2 The clinical symptoms of EAC cancer can be nonspecific, usually manifesting as hearing loss, EAC masses, otorrhea, and earache. Early intermittent earache is the most common type of complaint in patients with EAC cancer. 3 Therefore, it is easy to misdiagnose and confuse chronic otitis media, otitis externa, and benign EAC tumors. 4 External auditory canal cancer is characterized by slow growth, a high rate of local recurrence, and distant metastases, primarily to the lung and bone. 5 In this article, we report a case of advanced ACC of the EAC with lung metastases in terms of clinical manifestations, surgical methods, and postoperative recovery and describe our experience in diagnosing and treating ACC of the EAC.
Case Description
A 61-year-old male patient complained of intermittent right ear pain for more than 3 years. He was found to have had a mass in the right EAC for more than 1 year and to have experienced right facial paralysis for more than half a year. The mass in the right ear gradually grew, and his hearing in the right ear progressively worsened.
Enhanced CT of the temporal bone and enhanced MRI of the head (Figure 1) showed a dense shadow in the right temporal subcutis, EAC, middle ear tympanic chamber and soft tissue of the mastoid process involving the internal carotid artery, the right parotid gland, the temporalis muscle and possibly the facial nerve. Brain MRI showed abnormal signals in the right temporal and preauricular subcutaneous tissue, external auditory canal, and middle ear tympanic chambers (A, B; white arrows). Multiple nodules with increased metabolism in both lungs with possible metastases (C; white arrows).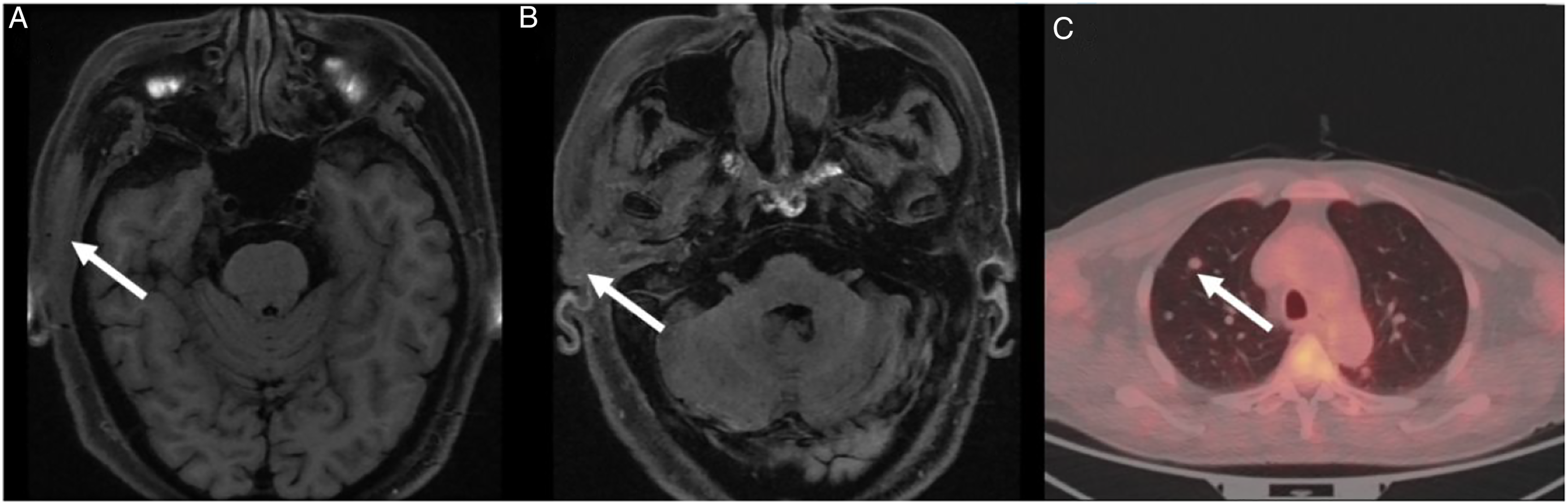
Positron emission tomography-computed tomography (PET-CT) showed that there were multiple nodules in both lungs, the largest being approximately 8.9 mm in diameter, and metastases were suspected (Figure 1). Local biopsy pathological puncture reported “basal cell carcinoma.” Positron emission tomography-computed tomography revealed lesions with increased metabolism in the right temporal bone, soft tissues of the ear and the EAC that were considered malignant; multiple metastases in the right cervical lymph nodes and in the lungs bilaterally were suspected. Our team decided that a diagnosis and treatment plan should be formulated after evaluation of a second pathological biopsy. The pathological report of the second biopsy indicated a diagnosis of “ACC” (Figure 2). No family history or other relevant medical history was reported. Pathology images of the patient. (A and B) Representative area of the tumor showing adenoid cystic carcinoma (hematoxylin–eosin stain, ×40 and ×100). (C) Immunohistochemistry for CD117. CD117 positivity was localized on the cell membrane of glandular epithelial cells.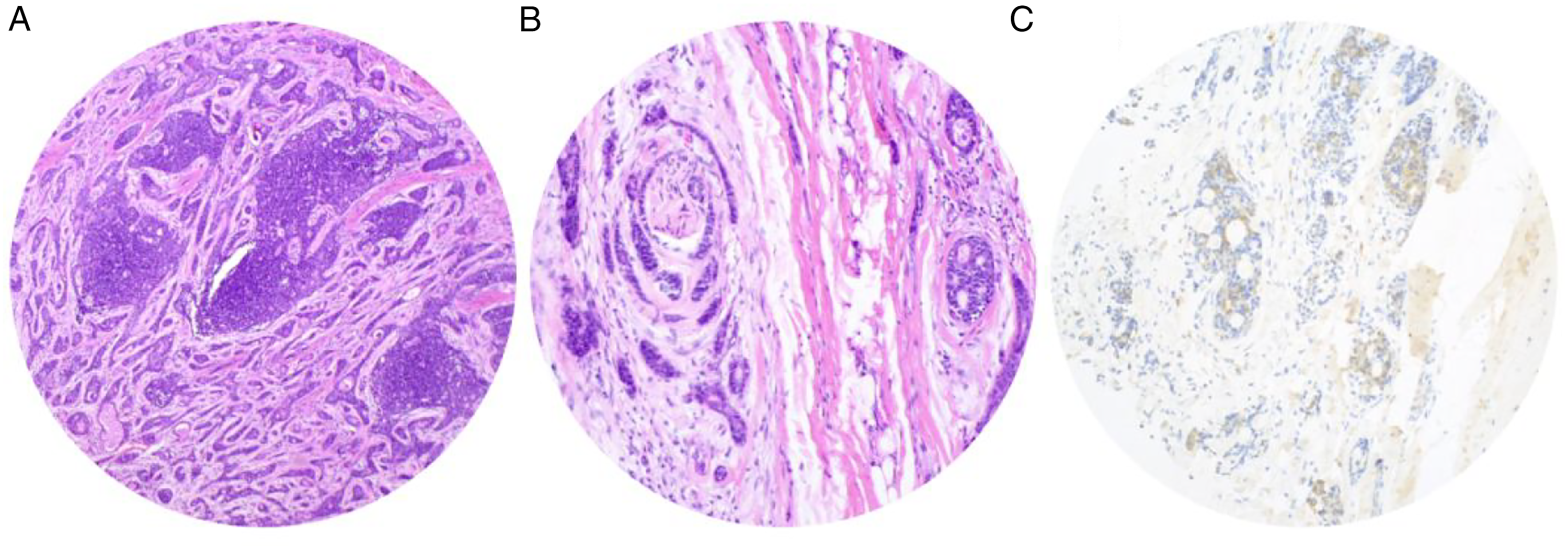
Under general anesthesia, lengthened right temporal bone resection, parotidectomy, facial nerve resection, cervical lymph node dissection (I-III), partial mandibular resection, tumor resection in the inferior temporal fossa and lateral femoral flap repair were performed. During the operation, it was found that the tumor partially invaded the lateral wall of the mandibular joint capsule at the mouth of the EAC and entered the infratemporal fossa, the superior pole of the parotid gland and the main trunk of the facial nerve as well as the anterior and upper part of the temporal muscle. Intraoperative pathological margins were negative, postoperative pathology was consistent with ACC, and lymph nodes showed chronic inflammation.
The patient’s tumor had encroached on the osseous EAC, facial nerve and parotid gland with presumed clinical staging of PT4aN0M1 according to the University of Pittsburgh’s TNM staging system for EAC cancer. 6 Considering that the patient had advanced adenoid cystadenocarcinoma of the EAC with lung metastasis, radiotherapy was helpful to control local lesions, while systemic chemotherapy controlled the lesions and prolonged the patient’s survival. Postoperative radiotherapy was given 35 times with a total dose of 70 Gy. Two courses of CAP chemotherapy (cyclophosphamide, doxorubicin, and cisplatin) were administered regularly afterward, and the cervicothoracic enhancement CT examination performed 2 years after the operation revealed that there were postoperative changes in the right EAC and multiple metastases in both lungs; the metastases exhibited a maximum diameter of approximately 16.4*15.8 mm, indicating that they were larger than before. The patient died 2 years after surgery from metastatic cancer of the lung.
Discussion
Only 10–15% of tumors are located in the EAC, and they are mainly squamous cell carcinoma. 7 In addition to squamous cell carcinoma, the differential diagnosis includes basal cell carcinoma, adenocarcinoma, ACC, melanoma, and EAC sarcoma. 8 The sources of these tumors have yet to be fully elucidated.
Adenoid cystadenocarcinoma of the EAC develops slowly. Fliss et al 9 suggested that as ACC tends to involve the perineural system early on, otalgia is one of the most common symptoms. This is consistent with the findings in this case, where the initial symptom was ear pain, followed by evidence of a mass in the ear, hearing loss, and facial paralysis. Because these symptoms are not specific, it is important to note when they are chronic, recurring, or exacerbating or when an ear mass shows progressive growth.
Adenoid cystic carcinoma of the EAC must be diagnosed early to improve survival rates. Unfortunately, the misdiagnosis rate is relatively high. Due to the absence of typical symptoms, ACC of the EAC can present with atypical symptoms such as earache, otorrhea, and hearing loss. It is also noteworthy that although a biopsy must be performed for suspected cases, physicians are not aware of this need.
Since there are few cases of ACC of the EAC and little literature on ACC management in the EAC, the management of ACC is primarily based on the surgeon’s experience. A complete cure for the tumor is needed, and it can be achieved through a variety of surgical techniques, including local EAC resection, en bloc EAC resection, and excision. The patient's imaging showed that the parotid gland, internal carotid artery, and facial nerve had invaded important structures, and the final pathological report was adenoid cystadenocarcinoma. The patient was found to have lung metastases, and multiple pathological biopsies were performed; however, complete surgical resection was performed, followed by radiotherapy and chemotherapy. There was no local recurrence in the 2-year follow-up after surgery, indicating that the surgical resection was complete and that the local recurrence rate was low.
Regarding patient treatment in the present study, the recommendations found in representative literature, including case series, were followed in large part. Early extended resection has been recommended by some authors. 1 To remove related cartilage, the mastoid process, and the middle ear, a large-area total resection of the EAC is recommended for ACC of the EAC. A subtotal or total resection of the temporal bone can be performed if preoperative examinations reveal that tumor has invaded the temporal bone or affected the facial nerve. The parotid gland can be completely removed if it has been significantly invaded. 10 According to some authors, 6 patients with T1 and T2 stages should undergo lateral resection of the temporal bone, and those with T3 and T4 stages should undergo subtotal resection of the temporal bone and infratemporal fossa. According to Moffat et al, 11 radiotherapy can destroy subclinical tumor foci and increase surgical success. Radiotherapy may be particularly effective for advanced tumors when it is difficult to achieve safe margins. Silverman et al 12 suggested that patients with advanced clinical disease require postoperative radiotherapy, while patients with negative first surgical margins and lower clinical stage do not require radiotherapy.
Conclusion
Early detection of symptoms, especially earache symptoms, necessary otoscopy and imaging examinations, and timely biopsy are key to reducing the misdiagnosis rate. Adenoid cystic carcinoma in the EAC is easily misdiagnosed; in this case, the patient’s condition was difficult to diagnose even with advanced pulmonary metastases, so it is important to be aware of the possibility of ACC in patients with similar symptoms. In addition, ACC is painful; surgery improves end-of-life treatment and resolves associated pain while not definitively prolonging survival.
Footnotes
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Multidisciplinary Cooperative Diagnosis and Treatment Capacity Building Project for Major Diseases (Z155080000004).
Ethical Statement
This study was approved by the Ethics Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, and the requirement for informed consent from the patient was waived. A patient’s anonymity is preserved in the manuscript.
Data Availability Statement
The data used to support the findings of the study are included within the article.