
Abstract
Objective
This study aims to investigate the clinical diagnosis and treatment characteristics of primary laryngeal neuroendocrine carcinoma.
Patients and Methods
A retrospective analysis was performed for the data of 6 patients with primary laryngeal neuroendocrine carcinoma admitted to the Department of Otorhinolaryngology of Dalian Central Hospital from September 2015 to January 2022, all of whom were male patients. And laryngoscopy showed that 4 had a similar appearance to hemangioma, 1 had nodular hyperplasia, and 1 was papilloma-like. The site of onset was located on the laryngeal surface of the epiglottis in 3 cases, situated in the aryepiglottic fold in 2 cases, and the posterior ventricular zone in 1 case. Five patients underwent surgery, including 4 by transoral endoscopic cryogenic plasma radiofrequency mass resection; one underwent a cervical lymph node dissection and supraglottic horizontal hemilaryngectomy. The remaining 1 case was treated in another hospital after the pathological diagnosis was confirmed by biopsy. All patients had no cervical lymph node metastases and were not supplemented with chemoradiotherapy.
Results
The postoperative pathological diagnosis of all 5 patients was neuroendocrine carcinoma. No cancer cells were seen at the margins and base. One patient was lost to follow-up after treatment in another hospitals and the rest were followed up for 6 months to 6 years. One patient had removed laryngeal tumor and epiglottis by a low-temperature plasma radiofrequency ablation, recurrence 1 year after surgery, and no recurrence for 5 years after supraglottic horizontal hemilaryngectomy combined with prophylactic cervical lymph node dissection, no recurrence for the other 4 patients after 6 months to 4 years of follow-up.
Conclusion
The common sites of laryngeal neuroendocrine carcinoma are the laryngeal surface of the epiglottis and the aryepiglottic fold. The appearance of the tumor is mainly similar to that of hemangioma. Moreover, a common pathological classification is atypical carcinoid tumors, where early detection and surgical treatment can achieve a good therapeutic effect.
Introduction
Primary laryngeal neuroendocrine carcinoma is relatively uncommon, and the early stages do not typically present with recognizable clinical symptoms. Patients are vulnerable to getting the wrong diagnosis during their first visit, preventing them from receiving prompt treatment. Most current domestic and international works on laryngeal neuroendocrine cancer have focused on pathological diagnosis and therapy options. There is a lack of a systematic summary of clinical features. In this paper, the clinical information from 6 primary laryngeal neuroendocrine cancer cases is retrospectively analyzed. Based on the literature, we discussed the clinical diagnosis and characteristics of laryngeal neuroendocrine carcinoma treatment.
Patients and Methods
Clinical Data
A retrospective analysis was performed on six patients with primary laryngeal neuroendocrine carcinoma in Dalian, China, admitted to the Department of Otorhinolaryngology of Dalian Central Hospital from September 2015 to January 2022, with limited laryngeal lesions and no lymph node metastasis. Complete tests are conducted to rule out other lesions. All patients were male, with an average age of 65 ± 7 years, had a history of perennial smoking, and had no common chronic diseases. Four patients complained of throat discomfort, one of which was accompanied by choking on drinking water and dyspnea after activity. The remaining two patients had a sore throat with mild hoarseness. The morphological manifestations of laryngoscopy were 1 case of smooth purple mass-like new organisms on the surface of the right aryepiglottic fold (Figure 1). One instance of a papillomato-like mass that was slightly rough and protruded from the right aryepiglottic fold (Figure 2). One instance was of a smooth hemangiomatous mass on the left ventricular band’s posterior surface (Figure 3). One instance was of dark red, slightly bumpy mass on the left surface of the epiglottis (Figure 4). In addition, one instance was of slightly rough, dark red mass on the epiglottis’ middle surface (Figure 5). One instance was of large and rough laryngeal surface of the epiglottis with dark red and gray-white mixed nodular hyperplasia (Figure 6). All masses range in diameter from 5 mm to 35 mm. Patients in Figures 1 and 3 were diagnosed with hemangiomas and were not examined pathologically. The remaining 4 patients were all biopsied and pathologically examined before surgery. The pathological diagnosis was all neuroendocrine carcinoma. Smooth surface purple clump-like mass. Unsmooth and reddish like a papilloma-like mass. The surface is slightly unsmooth, and the dark red mass. Slightly unsmooth surface, dark red larger mass. The surface is slightly unsmooth, and the dark red mass. The surface is not smooth, and nodular hyperplasia of mass.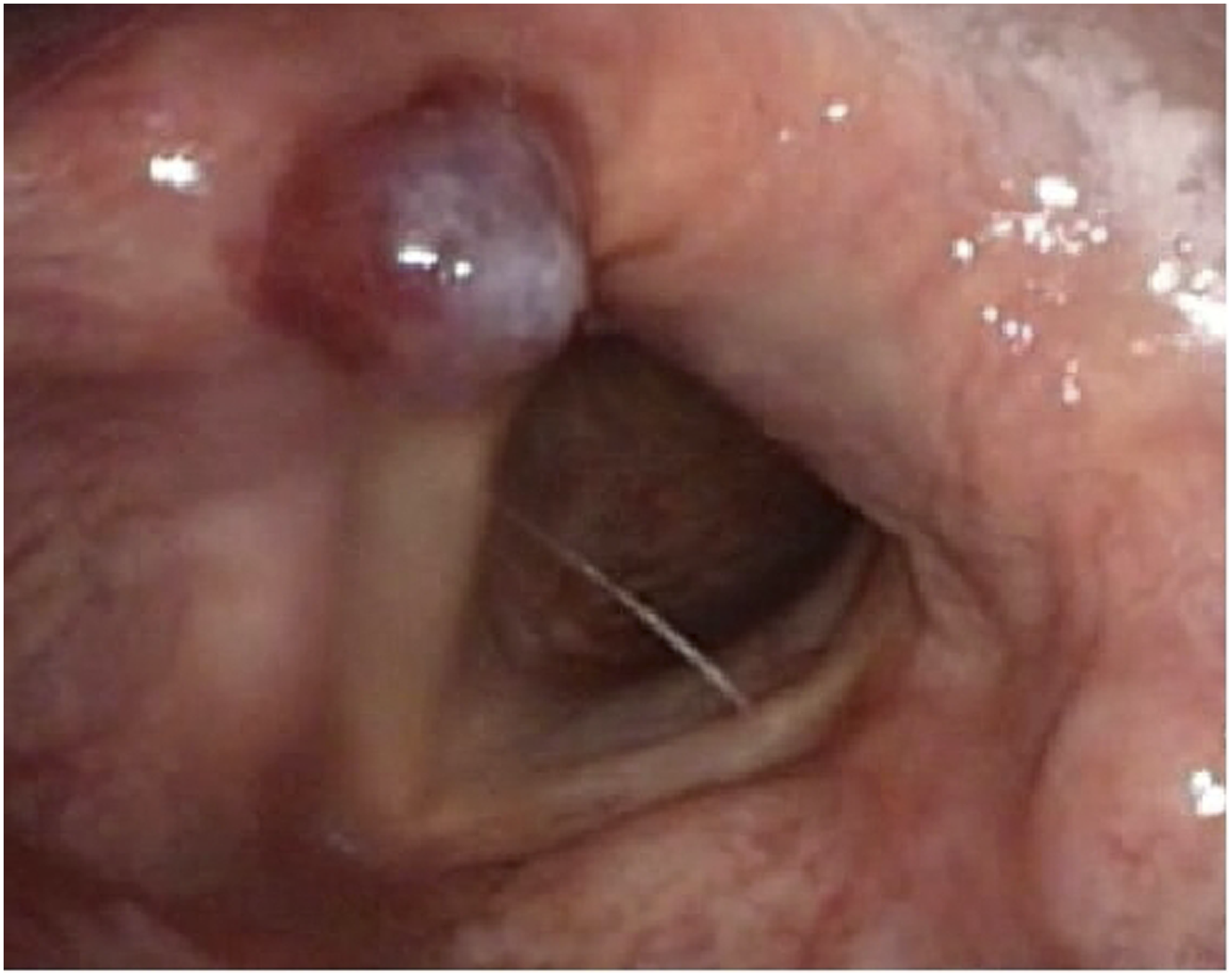





Surgical Technique
In Figure 4, the patient was diagnosed with high-moderately differentiated neuroendocrine carcinoma before surgery and treated in another hospital. The remaining five patients underwent surgery. Among them, the patients in Figure 6 underwent supraglottic horizontal hemilaryngectomy combined with prophylactic cervical lymph node dissection, and the other 4 underwent transoral endoscopic low-temperature plasma radiofrequency mass resection. The range of more than 5 mm from the edge of the mass during surgery was the safety edge for mass resection, and all were sent for postoperative pathological diagnosis. Lymph nodes in neck dissection had no metastases. All patients underwent abdominal CT, ultrasound, and lung CT without abnormalities to rule out gastrointestinal and respiratory tract tumors without adjuvant radiation therapy.
Results
All 5 cases of postoperative pathology reported laryngeal neuroendocrine carcinoma. The degree of differentiation was 3 cases of moderately differentiated type, 1 case of high-differentiated type, and 1 case of high-moderately differentiated type. No cancer cells were seen at the margins and base. Regular follow-up was followed up for six months to six years. In Figure 5, the patient underwent transoral endoscopic low-temperature plasma radiofrequency epiglottis and mass resection, which recurred 12 months after surgery, followed up for 5 years after supraglottic horizontal hemilaryngectomy combined with prophylactic cervical lymph node dissection, and no tumor recurrence. In Figure 4, the patient was lost to follow-up after treatment in another hospital. The remaining 4 patients were followed up for 6 months to 4 years, and there were no tumor recurrences.
Discussion
Neuroendocrine carcinoma is a type of cancer produced by neuroendocrine cells that spread throughout the body and can secrete many peptide hormones, resulting in various clinical symptoms. It is called the term “carcinoid syndrome.” The prevalence of neuroendocrine carcinoma diagnoses has steadily increased in recent years due to technological advancements in medicine. The most frequent primary sites are the gastrointestinal tract and the lungs. The disease is exceptionally malignant and quickly metastasizes. The metastatic potential varies depending on the primary site. However, liver metastasis is more common. As a result, monitoring liver metastasis is helpful for initial diagnosis and treatment. 1 Patients with head and neck neuroendocrine carcinoma have a higher survival rate than those whose lesions come from other sites. However, it is somewhat lower than that of patients with laryngeal squamous cell carcinoma. 2
The clinical incidence of primary laryngeal neuroendocrine carcinoma is extremely low, accounting for less than 1% of all laryngeal tumors, where the patients are mostly men aged 43∼72. The most critical recognized risk factor is smoking. 3 All six patients in this paper were male, all with a history of smoking for many years. The gold standard for diagnosis is pathology. The commonly used markers include epithelial-derived markers such as cytokeratin, carcinoembryonic antigen, epithelial cell membrane antigen, and neuroendocrine tumor common markers such as NSE, CgA, and Syn. In 2017, the WHO divided laryngeal neuroendocrine carcinoma into the following types according to histological morphology: typical carcinoid (highly differentiated type), atypical carcinoid (moderately differentiated type), small cell neuroendocrine carcinoma (poorly differentiated type), large cell neuroendocrine carcinoma (poorly differentiated type),2,3 among which atypical carcinoid is a more common and aggressive malignant tumor. 3 Among the 6 patients in this group, 3 were pathologically classified as moderately differentiated type, 2 were high-moderately differentiated type, and 1 was a highly differentiated type, all without lymph node metastasis. The larynx is the most common site of head and neck neuroendocrine carcinoma. It is mainly caused by abnormal neuroendocrine and glandular epithelial differentiation in the laryngeal mucosa. 2 Strosberg et al found in the study that the moderately differentiated type is more prone to lymph node metastasis and has a high mortality rate. 4 Hence, how to diagnose and treat the disease in the early stage to avoid misdiagnosis and missed diagnosis is a key concern for clinicians. In recent years, the diagnostic research of laryngeal neuroendocrine carcinoma has mostly tended to be molecular. Feola et al found the importance of elevated serum calcitonin in diagnosing and treating this disease. 5 Yuan et al pointed out that when the insulinoma-associated protein 1 is strong, it has high sensitivity and specificity for diagnosing laryngeal neuroendocrine carcinoma, and its sensitivity is higher than that of Syn, CHG, and CD56. 6 In recent years, most of the literature on laryngeal neuroendocrine carcinoma at home and abroad has been reported individually. Most of them are mainly based on pathological diagnosis and treatment methods. There is a lack of a systematic summary of the clinical characteristics of the disease. Based on the literature reports and the cases in this paper, there are no typical clinical symptoms in the early onset, and hoarseness, breathing, or swallowing disorders may occur when the disease progresses to a certain extent. In this paper, 6 patients mainly showed pharyngeal discomfort or sore throat and mild hoarseness, and 1 patient with a large mass was accompanied by choking on eating and difficulty breathing after activity. Hence, the early symptoms were not significantly specific. Most atypical carcinoid appearances on laryngoscopy are hemangiomatoid masses. For example, Hu et al found a dark red oval new organism with a smooth surface and a size of about 1.8 cm × 1.4 cm on the left side of the patient's epiglottis laryngeal surface, with a broad base. 2 Two of the 6 patients in this group had tumors that closely resembled hemangiomas in appearance, as shown in Figures 1 and 3. Both cases were admitted to the hospital with “laryngeal hemangioma” to avoid bleeding, the pathological examination was not performed, and surgical treatment was carried out directly. In patients with Figures 4 and 5, the masses were located on the laryngeal surface of the epiglottis, and the appearances were also dark red, similar to the hemangioma, but slightly not smooth. Two patients’ pathological diagnosis was confirmed to be a high-middle-differentiated neuroendocrine carcinoma before surgery. The patient’s tumor (Figure 6) is large, dark red and gray-white mixed nodular hyperplasia, which does not exclude the early onset of the disease and is also a near-hemangiomatous appearance. Therefore, the appearance of laryngeal neuroendocrine carcinoma is suspected of being a hemangioma, and it needs to be differentiated from laryngeal hemangioma. Laryngeal hemangiomas are divided into capillary and cavernous hemangiomas, according to pathology, and the former is more common. Capillary hemangiomas are small and pedicle, bright red or dark red, round or oval, mulberry-like, and easy to bleed. Cavernous hemangiomas are soft and spongy with a broad base, and the tumor tends to be blue or hemorrhagic polyps.7,8 Laryngeal hemangiomas in adults do not resolve spontaneously but grow slowly in their natural history, 9 could occur at any age, and generally do not interfere with life. Moderately differentiated and poorly differentiated laryngeal neuroendocrine carcinomas are easily metastasized through lymph nodes. Suppose they cannot be diagnosed and treated in time. In that case, they are likely to have a considerable impact on the prognosis of patients. 2 There have also been reports of laryngeal neuroendocrine tumors as polypoid in appearance. 10 The appearance of cases in Figure 2 of this group is light red and slightly unsmooth polypoid mass, similar to the appearance reported in the literature. The literature has reported that tumor onset sites are more common in the epiglottis laryngeal surface and aryepiglottic fold. 4 Three cases in this group were located on the epiglottis’s laryngeal surface, two in the aryepiglottic fold, and one behind the left ventricular belt, indicating that laryngeal neuroendocrine carcinoma can occur in any area of the larynx. However, it is more common in the laryngeal surface of the epiglottis and aryepiglottic fold.
The treatment options and prognosis of different pathological types of laryngeal neuroendocrine carcinoma are different. 11 The metastasis of well-differentiated neuroendocrine carcinomas is rare. In addition, the treatment method of local resection is preferred without adding radiotherapy and chemotherapy. The 5-year survival rate after surgery is extremely high. Poorly differentiated neuroendocrine carcinoma tends to occur lymph node metastasis in the early stage and has a poor prognosis. Although the literature shows that radical chemoradiotherapy has not been considered an effective treatment regimen, 12 the combination chemoradiotherapy regimen is still the best choice. Atypical carcinoid tumors often have lymph node metastasis at diagnosis. Although cervical lymph node metastasis sometimes does not occur, it may be that micrometastases in the early stage of the lesion are not detected in time due to limitations of imaging examination. Cervical lymph node dissection and radical resection are required to improve survival. There is still controversy about whether combination chemoradiotherapy can improve the treatment effect. 12 In recent years, there have been different reports on the treatment options for high or moderately differentiated laryngeal neuroendocrine carcinoma, such as partial laryngectomy or total resection,1,13 supraglottic laryngectomy by transoral CO2 LASER,1,13 and low-temperature plasma radiofrequency laryngeal mass resection.2,13
Moreover, there is no unified treatment guidelines. 14 The treatment plan can be formulated according to the treatment principles of laryngeal squamous cell carcinoma. For patients with limited early lesions and good exposure, it is appropriate to remove the tumor by transoral CO2 LASER or low-temperature plasma radiofrequency ablation, which can achieve the same therapeutic effect as open surgery to remove the mass altogether and improve the patient’s quality of life; for patients with extensive tumor invasion and difficulty undergoing minimally invasive transoral surgery, a partial or total laryngectomy and cervical lymph node dissection via a traditional external incision are required. In this group, patients in Figure 6 underwent supraglottic horizontal hemilaryngectomy combined with prophylactic cervical lymph node dissection due to a large mass on the laryngeal surface of the epiglottis, and there was no recurrence at the current follow-up for 10 months. The four cases were treated with transoral endoscopic low-temperature plasma radiofrequency laryngeal mass resection, which preserved the laryngeal function and ensured the patients’ quality of life after surgery. One of them, shown in Figure 5, underwent a supraglottic laryngectomy with cervical lymph node dissection a second time. After five years of postoperative follow-up, there has been no recurrence. The recurrence may be due to the short range of plasma radiofrequency to the local resection of the epiglottis. In Figure 4, after the patient's diagnosis, the patient was treated in another hospital for loss to follow-up. Because the postoperative pathology of all surgical patients is moderately differentiated or high-moderately differentiated, the degree of malignancy is relatively low, the tumor margin is clean, there is no lymph node metastasis, and radiotherapy is not supplemented. Mesolella et al found 1 case of small cell neuroendocrine carcinoma combined with Lambert-Eaton myasthenic syndrome in clinical diagnosis and treatment, which is an extremely rare neurological paraneoplastic syndrome accompanied by lymph node metastasis. 14 The patient underwent a total laryngectomy with a radically modified neck dissection on the left side with the sacrifice of the internal jugular vein and spinal nerve. The effect of postoperative radiotherapy and chemotherapy for treatment is good. It is proposed that paraneoplastic syndrome is very rare, although not directly related to the tumor or its metastasis. However, it can indicate the existence of cancer or clinical manifestations in its evolution. Early combination therapy is required to improve the quality of life of patients. Presently, the mechanisms of distant metastasis, local recurrence, and prognostic factors are unclear.14,15
In summary, through the diagnosis and treatment analysis of 6 cases combined with literature reports, this paper preliminarily summarizes the clinical diagnosis and treatment characteristics of laryngeal neuroendocrine carcinoma as follows: (1) It is more common in men over 40 years old. The history of smoking for many years is a significant risk factor for disease; (2) the early clinical manifestations are non-specific, most of which were complaints of sore throat, pharyngeal discomfort and mild hoarseness; (3) the onset site is more familiar with the epiglottis laryngeal surface and aryepiglottic fold; (4) The morphological manifestations of the masses are primarily hemangiomatoid-like. A small number are tumor-like or polyp-like; (5) immunohistochemical pathological examination is required for diagnosis. The pathological type is more common as atypical carcinoid; (6) early detection, transoral laser or low-temperature plasma radiofrequency tumor resection can achieve good treatment effect and improve the quality of life of patients; (7) once diagnosed, it is appropriate to improve the necessary examinations, be alert to whether there are the same tumors in the gastrointestinal tract and lungs, and pay attention to whether there is liver metastasis. In short, due to the low incidence of the disease, the number of cases diagnosed and treated, and the follow-up time of individual cases is still short, the above characteristics are only for reference. It is necessary to continue to improve through more case treatment and experience summaries in the future.
Footnotes
Authors’ Note
Clinical diagnosis and treatment of primary laryngeal neuroendocrine carcinoma. First of all, we want to apologize for the first author of the article’s lack of information. The first author belongs to both 1Dalian municipal Central Hospital and 2Dalian Medical University. The first author is a graduate student. Dalian municipal Central Hospital is affiliated to Dalian Medical University and is responsible for managing postgraduate research and study. Since Dalian Central Hospital is the source of all patient data in this work, it is important to modify the first author’s unit information to 1Dalian municipal Central Hospital and 2Dalian Medical University in order to maintain academic rigor and comply with hospital rules and regulations.
Acknowledgments
We appreciate the teachers at Dalian Central Hospital’s medical records department who offered retrieval services at the beginning of the work. In addition, we are especially grateful to Dr Fumei Ma for providing guidance in the details of the article to make the article more professional and accurate.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We would like to start by apologizing for our error; this was the first time, my student, Yu Wang, had completed it independently, and throughout the submission procedure, she had broken SAGE policy and hampered your job. We are very sorry about that.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This is an observational study. The Research Ethics Committee of Dalian Municipal Central Hospital has confirmed that ethical approval is unnecessary.