
Abstract
Ameloblastoma (AM) is a rare epithelium-derived odontogenic tumor, mostly involving the mandible and less often the maxilla. Most AMs are benign and characterized by indolence and local invasiveness, with a high recurrence rate. Herein, we present a case of maxillary AM in a 42-year-old female suffering from left nasal congestion and facial swelling for almost one month after endoscopic surgery at a local hospital. The mass was completely resected by a transnasal functional endoscopic sinus surgery based on radiographic examination. Subsequently, postsurgical histopathological examinations were conducted, and she was diagnosed with a plexiform AM pattern. Immunohistochemical staining revealed that the tumor was positive for PCK, P63, CK5/6, and CK14 but negative for S100, ER, and Ki67. Based on these findings, the patient was diagnosed with maxillary AM.
Introduction
Ameloblastoma (AM) is the most common odontogenic tumor and accounts for 1% of all head and neck tumors. 1 AM is histologically benign and grows slowly with a long disease course. 2 AM mainly occurs in young adults, more commonly in men. Most AMs affect the mandible and rarely the maxilla (less than 20%). 3 A subset of these maxillary AM is thought to originate from the epithelial lining of the sinonasal cavities. 4
Maxillary AM has been reported in early childhood until old age 3 and occurs about ten years later than mandibular AM, thus lacking obvious early symptoms. 5 However, the tumors gradually increase and aggressively extend beyond the maxilla causing various symptoms and leading to diagnosis at an advanced stage.5,6 Compared to the compact mandible bone, the cancellous maxilla bone is easier for the AM to invade adjacent structures, including the nasal cavity, paranasal sinuses, orbits, parapharyngeal tissues, and skull base. 7 To date, there have been few cases of AM, especially maxillary AM, with only very few English articles reporting maxillary AM in Chinese patients.
Case Report
A 42-year-old woman suffering from left nasal congestion and facial swelling for almost one month was admitted to the outpatient clinic in Wuhan Union Hospital in June 2022. The patient reported having just undergone endoscopic surgery at the local hospital and was diagnosed with sinusitis pathologically. The following month, she began to develop facial swelling and left nasal congestion but had no other sinonasal symptoms, such as nasal discharge, headache, and loss of smell. The patient was treated unsuccessfully with antibiotics at the local hospital, so she was admitted to our inpatient department.
Computed tomography (CT) of the paranasal sinuses indicated a space-occupying lesion and bone invasion of the paranasal sinus. The scan detected a slightly dense shadow 26.6 × 41.9 × 43.8 mm in size in the left maxillary sinus, wrapping the bone like an eggshell (Figure 1A). There was a bone invasion in the left maxillary sinus wall, especially in the inferior and lateral wall, as observed in the coronal (Figure 1E) and axial (Figure 1I) CT scan. There were also a few soft tissue density shadows in the left maxillary sinus and some thickened mucosa in the left ethmoid sinus, but the rest of the sinus cavity was clear. Radiological examinations show a space-occupying lesion and bone invasion in the left maxillary sinus. A: Coronal CT scan showing a slightly dense shadow measuring 26.6 × 41.9 × 43.8 mm in the left maxillary sinus and bone defect in the medial wall of the sinus (red arrow). B–D Coronal MRI scans showing the left maxillary sinus completely filled with heterogeneous cysts and solid mass shadows. The lesion was isointense on T1-weighted imaging and slightly hyperintense on T2. E: Coronal CT scan showing the thinned bone in the left maxillary sinus wall, and part of the bone was nearly interrupted, especially in the inferior and lateral wall from the coronal, involving the left upper alveolar bone (yellow arrow). F–H Coronal MRI scans show the linear separations inside with solid components and linear separations evident upon contrast administration. I: axial CT scan showing that the left maxillary sinus was infiltrated by the tumor and the anterior sinus wall was destroyed (yellow arrow). J–L Axial MRI scans revealed hyperintensity on T2-weighted MRI images in the left maxillary sinus. CT: computed tomography; MRI: magnetic resonance imaging.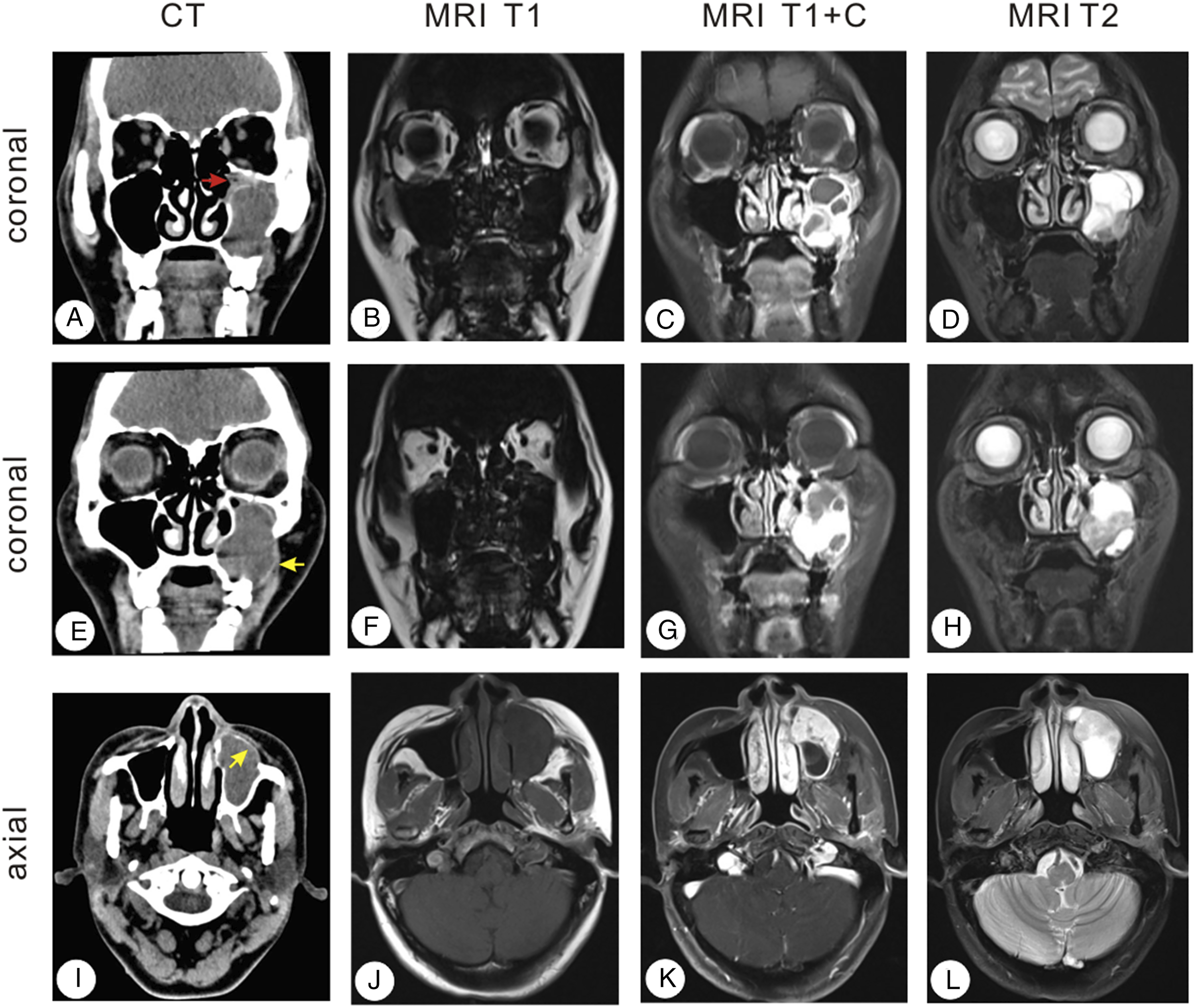
The MRI images confirmed the CT findings that the left maxillary sinus was completely filled with heterogeneous cystic and solid mass shadows (Figure 1B-D and F-G). The lesion was isointense in the T1-weighted imaging, while it was slightly hyperintense in T2. The linear separations were observed inside with solid components, and linear separations were visible upon contrast administration (Figure 1C and G). The local bone of the medial and inferior walls of the maxillary sinus was thinner, and the left upper alveolar bone was destroyed.
After a discussion with the patient, she decided to undergo a second procedure in our department, transnasal functional endoscopic sinus surgery under general anesthesia. The natural opening of the left maxillary sinus was opened under nasal endoscopy. When the aspirator device was inserted into the left maxillary sinus cavity, mucosal hyperplasia in the ostium and partial mucosal polypoid changes were observed. Polypoid neoplasms were found and removed from the left maxillary sinus for further pathological examination.
The AM can be divided into five different patterns, with the plexiform pattern being the second most common pattern composed of basal cells arranged in strips. There are two different forms of lace-like structure: strands formed by two layers of basal cells or strands which are thicker and looser with a more squamous cell appearance.
3
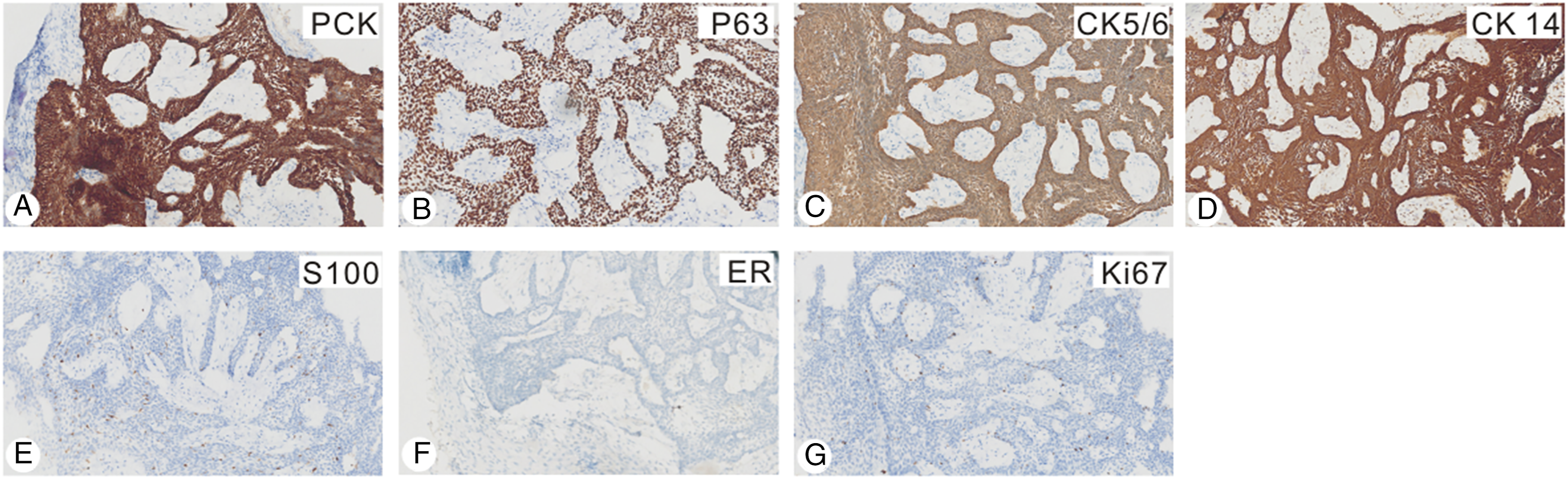
Since there is no obvious peripheral palisading and reverse nuclear polarity in both forms, the plexiform pattern is difficult to distinguish. In this case, the pathological findings revealed plexiform basal cells on the surface of the tumor (Figure 2). Immunohistochemical staining revealed that the lesions were positive for PCK, P63, CK5/6, and CK14 but negative for S100, ER, and Ki67 (Figure 3). Finally, according to the pathological and immunohistochemistry results, the patient was diagnosed with AM. Histologic analysis of specimens. A: Microscopic examinations depict the lace-like architecture consisting of short strands of basal cells of plexiform pattern (HE × 40). B: An area of thin inter-anastomosing cords of ameloblastic epithelium, where strands are thicker and looser with more squamous cell appearance (HE × 200). HE: hematoxylin and eosin staining. Immunohistochemical staining of the specimens. A–D: The tumor cells are diffusely positive for PCK (A), P63 (B), CK5/6 (C), and CK14 (D) (IHC 100×). E–G: The tumor cells are negative for S100 (E), ER (F), and Ki67 (G) (IHC 100×). IHC: immunohistochemistry.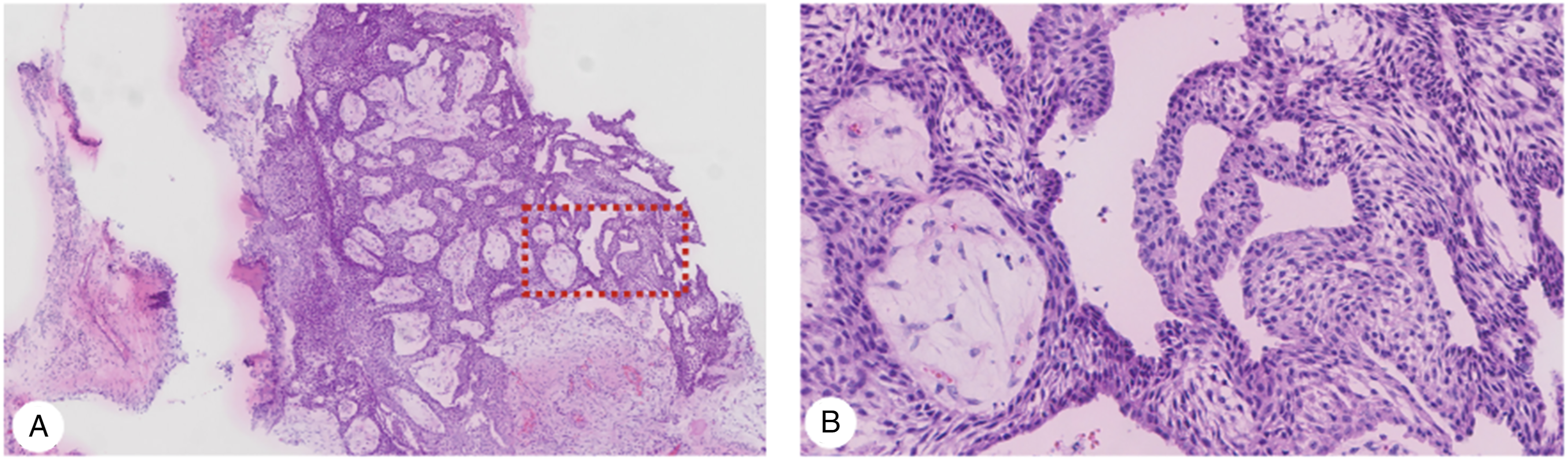
Discussion
AM was first described systematically by Falkson in 1879 and termed “ameloblastoma” by Churchill in 1933. AM is considered to be benign but has a high recurrence rate. 2 It is invasive and locally destructive, and a few of these tumors may become malignant. 8 AM is thought to be derived from the residual dental lamina or surface epithelium from the developing enamel organ 9 and mostly involves the mandible and less often the maxilla. 10 The ratio of maxillary and mandibular AM is 1:5.4. 11 Maxillary AM is very rare, and only a few cases have been reported. The tumor occurs in the maxilla, mostly near the second and third molars, and can invade the maxillary sinus destroying the walls, especially the anterior wall.
AM grows very slowly with a long disease course, so most patients are asymptomatic initially. The tumor gradually increases and compresses the surrounding bones, making them absorb, thin, or expand into the maxillary sinus, oral cavity, and nasal cavity. 12 Various symptoms manifest as (1) facial deformity: the facial or dental alveoli swelling, and there is a feeling of eggshell breaking when palpating; (2) nasal symptoms: nasal congestion, runny nose, epistaxis, and other symptoms; (3) eye symptoms: patients with orbital invasion may have eye displacement, tears, protrusion, etc.; (4) oral manifestations: invasion of the palate can cause mastication and pronunciation disorders. The recognition of AM may be delayed because the non-specific clinical features make it easy to be confused with a series of sinonasal pathologies, including benign nasal polyps and chronic sinusitis. 13
AM is benign, but since the tumor epithelium can invade the Haversian canal of the bone cortex or its surrounding epithelial tissue, there is a strong possibility of local invasion and relapse after surgery. 14 There is also the possibility of malignant transformation, but metastasis is rare. 9 The tumors contain different-sized cysts, which can be single, multiple, or honeycomb types. Multicystic tumors are more common. There are yellow serous or bloody secretions in the cyst, occasionally including a complete tooth. Radiographs or CT scans can show cysts or honeycomb shadows with irregular edges. Diagnosis should be differentiated from odontogenic cysts. 15
In our case, the nature of the mass was not clarified in the first surgery at the local hospital. When the patient was admitted to our hospital, the CT scan detected a space-occupying lesion in the left maxillary sinus, wrapping a bone that looked like an eggshell. MRI images further indicated that the sinus was completely filled with heterogeneous multicystic and solid mass shadows.
The histological manifestations of AM vary widely. According to the histological types of the epithelium, the tumors can be divided into five patterns: follicular, plexiform, acanthomatous, basaloid, and granular cells 1 with the follicular and plexiform patterns being the basic histological patterns. The follicular pattern is the most common and is composed of odontogenic epithelial islands in the fibrointerstitium. The basal cells of the epithelial islands are characterized as high columnar, with deeply stained nuclei and a polar arrangement. 16 The plexiform pattern comprises basal cells arranged in strips and interlaced into a network. The stellate reticular layer is not obvious, and the stroma is usually thin, often cystic. 3 It is not uncommon to have a combination of two or more patterns in one tumor. Different parts of the same tumor can also show different histological images but mainly follicular and plexiform, and the other types intersperse.
Although this tumor is benign, it is also locally heavily destructive. If the surgery is not thorough and complete, recurrence may occur. Repeated recurrence may lead the tumor to transform into AM or sarcoma. 17 This tumor should be completely removed by surgery, and postoperative radiotherapy can be attempted. 2
In conclusion, AM is an epithelium-derived odontogenic tumor mostly involving the mandible and less often the maxilla. Maxillary AM is very rare, and few Chinese cases have been reported in the literature. In this case, the tumor was easily misdiagnosed as a maxillary cyst by the smooth eggshell-like appearance, whereas the bone invasion was suggestive of a malignant tumor; therefore, this case is of great referential, exploratory, and observational value for clinicians.
Footnotes
Acknowledgment
We appreciate Mingzhu Zhou for her effort on the language editing.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the National Natural Science Foundation of China (81771005, ZT), the Research Grant of Union Hospital, Tongji Medical College, HUST (F016.02004.21003.126, ZT), and Open Project of Key Laboratory of Molecular Imaging (2021fzyx017, SH). “to” The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Natural Science Foundation of Hubei Province (2022CFB087 ZT), National Natural Science Foundation of China (81771005, ZT), and the Research Grant of Union Hospital, Tongji Medical College, HUST (F016.02004.21003.126, ZT).
Ethical/Consent Statement
Ethical approval and consent to participate: not applicable.
Data Availability Statements
All data generated or analyzed during this study are included in this published article (and its supplementary information files).