
Abstract
Introduction
Fungal rhinosinusitis can be broadly divided into 2 categories based on histopathological findings: invasive and noninvasive, depending on the invasion of the mucosal layer. Fungus balls (FBs) are the most frequent noninvasive fungal rhinosinusitis. deShazo et al 1 proposed the diagnostic criteria for FBs based on clinical, radiological, morphological, and histological findings. The incidence of FBs in paranasal sinuses is increasing, which could be related to improved awareness, the popularization of diagnostic techniques, the overuse of broad-spectrum antibiotics, increased endodontic treatment, and an aging population. FBs usually occur unilaterally, and the maxillary sinuses are most commonly involved.2-4 FBs affect immunocompetent hosts and are prevalent in older patients and females. Computed tomography (CT) has revealed the opacity of the cavity associated with a hyperdense area within the lesion. Dhong et al 5 showed that FBs had a characteristic of gritty, matted, gross appearance, and the majority of them had CT characteristics such as radiographic heterogeneity.
This clinical study demonstrated that FBs are associated with sinus inflammation. Several studies reported the clinical and radiological characteristics of maxillary sinus fungal ball (MSFB), while only a few studies described sinus inflammation associated with MSFB. The present study aimed to explore the characteristics and possible pathogenesis of FB-related sinus inflammation. The patients were divided into 2 groups: those with obstructed ostiomeatal complex (OOMC) and those with clear ostiomeatal complex (COMC) (Figures 1 and 2). We evaluated the occurrence of sinus inflammation in paranasal sinuses of the 2 groups according to the CT findings and analyzed the putative causes.
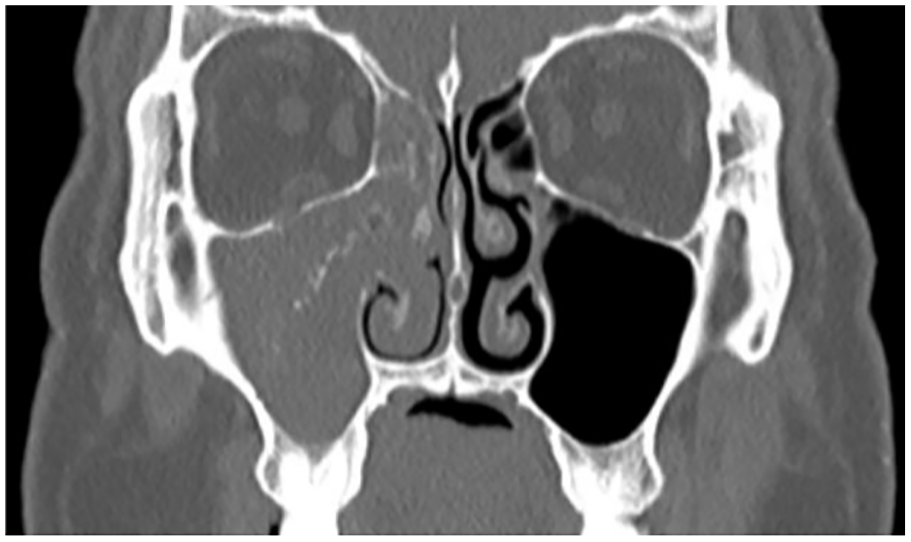
A coronal computed tomography scan showed fungal ball of the maxillary sinus protruded into the ostiomeatal complex and formed an obstructed ostiomeatal complex.

A coronal computed tomography scan revealed fungal ball of the maxillary sinus with a clear ostiomeatal complex.
Materials and Methods
This retrospective study included 1308 patients who were hospitalized in Beijing Tongren Hospital to undergo functional endoscopic sinus surgery (FESS) for the treatment of MSFB, while 34 patients who have had FESS were excluded. Also, 48 patients who had more than a single maxillary sinus suffered from FB were excluded. Finally, the information of 1226 patients who had unilateral MSFB was analyzed in this retrospective study. All of the information reviewed was obtained from the case database from January 2008 to December 2018. In all cases, we performed preoperative nasal endoscopy and an imaging study. The inclusion criteria for patient data were as follows: (1) CT results, (2) FB found during surgery in the maxillary sinus, or (3) FB confirmed by histopathology. The information collected was the gender, age, chronic disease, main clinical symptoms, and CT features. The study was approved by the medical ethics committee and written informed consent was obtained from each patient. The CT features were categorized as follows: (1) presence of intralesional hyperdensity, (2) erosion of the inner sinus wall, (3) sclerosis of the lateral sinus wall, (4) OOMC, (5) COMC, and (6) others, such as smooth protruding lesion, suggesting sinus inflammation.
SPSS 22.0 statistical software was used for data analysis (IBM Corp, Armonk, NY, USA). Continuous values were expressed as mean ± standard deviation and analyzed by t-test or nonparametric test. Categorical variables were presented as absolute numbers and analyzed by χ2 test. P values <.05 indicated statistical significance.
Results
Demographics and Clinical Presentation
The information of 1226 patients with unilateral MSFB was analyzed in this retrospective study. The ratio of men:women, age distribution, and duration of disease are shown in Table 1. The results indicated that 66.0% of patients were females (809/1226) and 34% were males (417/1226) in this study. The mean age of the cohort was 53.37 years. No significant difference was observed in the average age between men and women (P > .05). Moreover, 620 (50.6%) patients had left MSFB and 606 (49.4%) patients had right MSFB.
Demographic and Clinical Data for 1226 Patients in This Study.
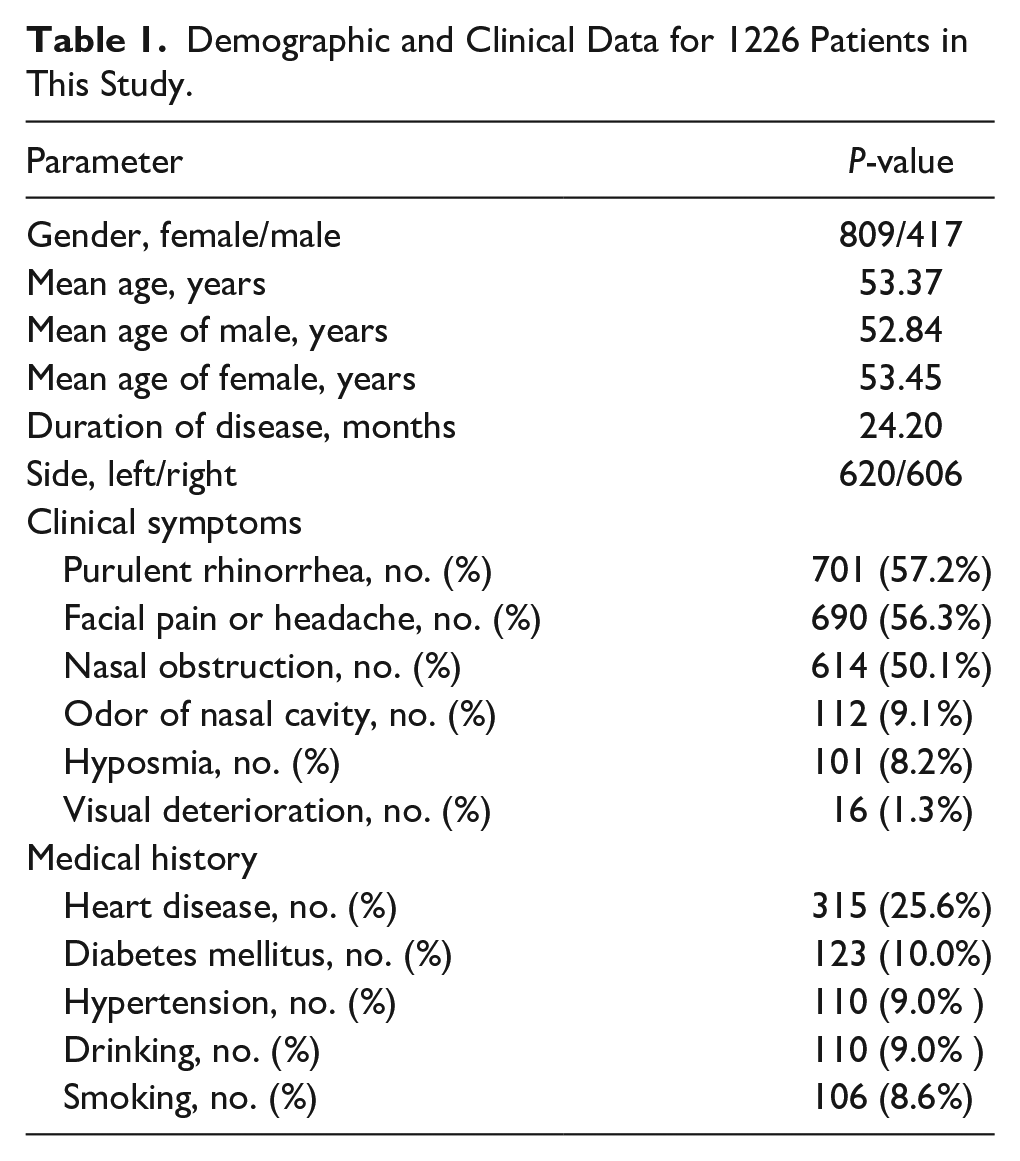
Most patients presented to our outpatient department were symptomatic, as shown in Table 1. The 3 main symptoms were purulent rhinorrhea (57.2%), facial pain or headache (56.3%), and nasal obstruction (50.1%). A total of 112 (9.1%) patients had an odor of nasal cavity, 101 (8.2%) patients had hyposmia, and 16 (1.3%) patients presented visual deterioration. Among them, 65 (5.3%) asymptomatic patients were diagnosed with MSFB by physical examination or imaging. The medical history of the patients is summarized in Table 1, and 25.6% of them had heart diseases, 10.0% had diabetes, and 9.0% had hypertension. Among these patients, 9.0% had a drinking history and 8.6% had a smoking history.
Analysis of Radiologic Characteristics
In the current study, 895 patients showed OOMC and 331 patients showed COMC on the ipsilateral side of MSFB. The demographic and radiological features of patients with OOMC were compared to those of patients with COMC (Table 2).
Sinus Inflammation Characteristics Between the OOMC and COMC Groups.
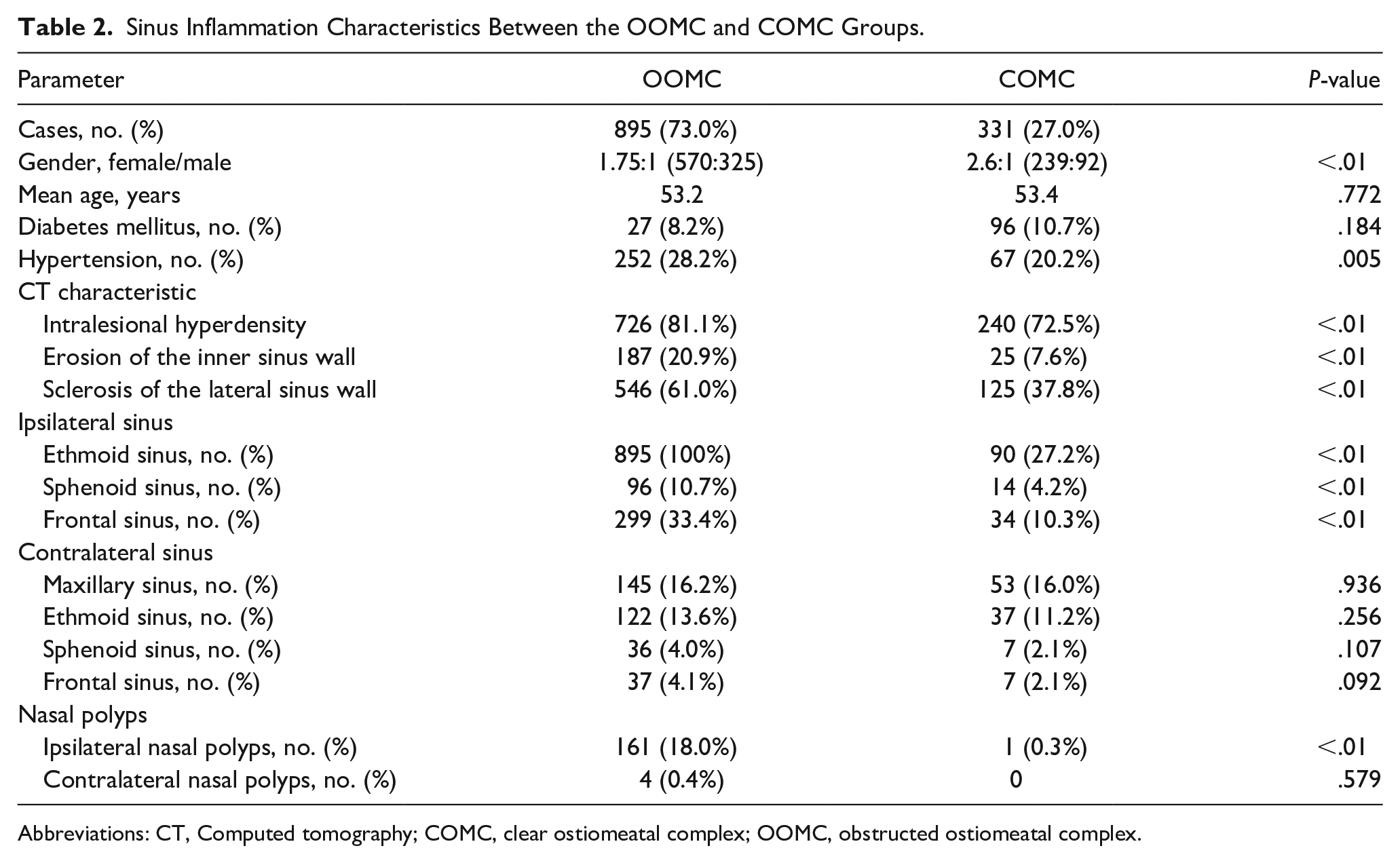
Abbreviations: CT, Computed tomography; COMC, clear ostiomeatal complex; OOMC, obstructed ostiomeatal complex.
An obvious female predominance was observed in patients with COMC (P < .01, χ2 test). No statistical difference was detected in the mean age between the OOMC and COMC groups. The OOMC group had higher incidences of intralesional hyperdensity, erosion of the inner sinus wall, and sclerosis of the lateral sinus wall than the COMC group (P < .01, χ2 test). In the ipsilateral sinuses of MSFB, patients with OOMC were significantly more likely to develop sinus inflammation than patients with COMC (P < .01, χ2 test). In the contralateral sinuses of MSFB, no statistical difference was observed in the probability of sinus inflammation between patients with OOMC and those with COMC. A total of 162 patients presented nasal polyps (NPs) on the ipsilateral nasal cavity of MSFB, while only 4 patients presented NPs on the contralateral nasal cavity.
In 1226 patients, the incidences of sinus inflammation in the contralateral sinuses were lower than that in the ipsilateral sinuses (P < .01, χ2 test). In the OOMC group, sinus inflammation was more common in the ipsilateral sinuses of MSFB than in the contralateral sinuses (P < .01, χ2 test). In the COMC group, the incidences of SI in ethmoid and frontal sinuses were higher in the ipsilateral sinuses of MSFB than in the contralateral sinuses (P < .01, χ2 test), while no significant difference was observed in the sinus inflammation incidence of the bilateral sphenoid sinuses.The radiological features of the ipsilateral sinuses of MSFB were compared to those of the contralateral sinuses in Table 3.
SI Characteristics Between Ipsilateral and Contralateral Sinus of MSFB.
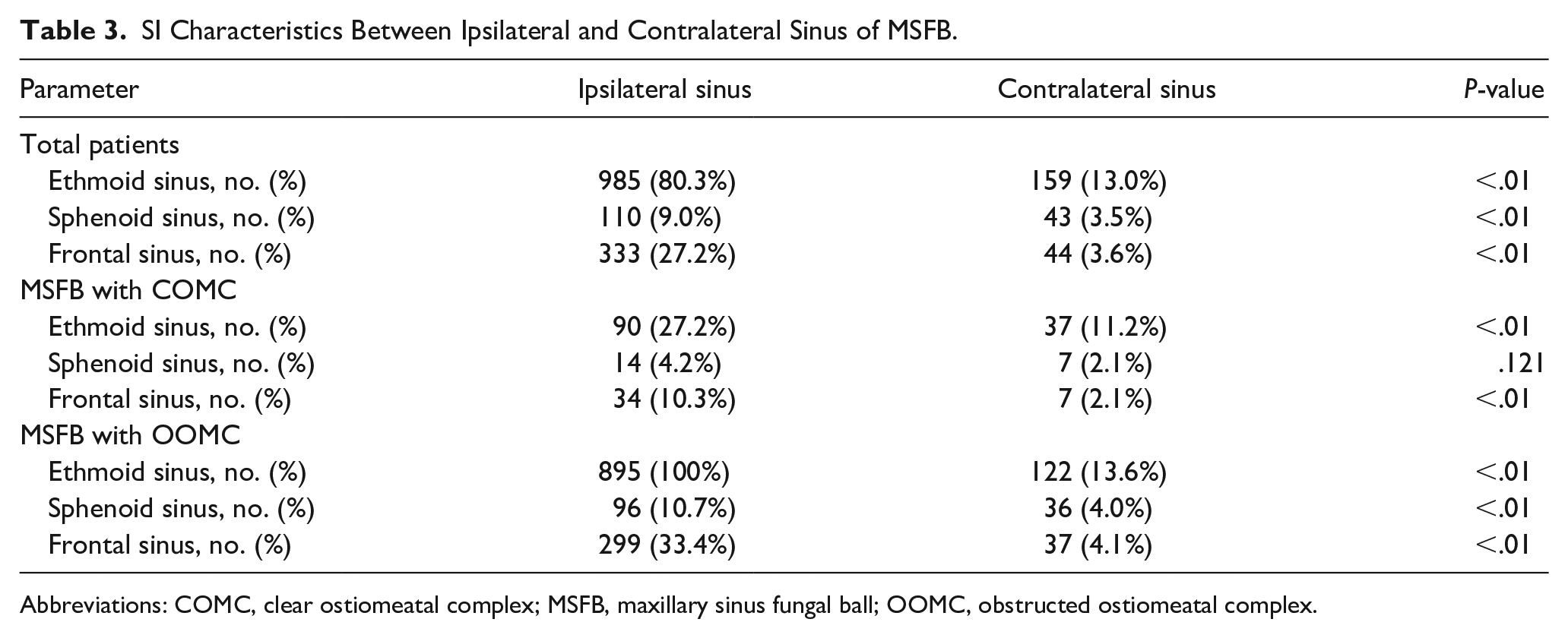
Abbreviations: COMC, clear ostiomeatal complex; MSFB, maxillary sinus fungal ball; OOMC, obstructed ostiomeatal complex.
Discussion
Compared to the COMC group, the patients in the OOMC group had higher incidences of sinus inflammation in the ipsilateral sinuses of MSFB (P < .01, χ2 test). On the contrary, there was no difference in the incidence of paranasal sinus inflammation contralateral to MSFB between the OOMC and COMC groups. Perhaps it is because the nasal septum leaves the contralateral sinuses unaffected. A similar pattern can be seen in a previous study, patients with severe MSFB had high Lund–Mackay scores in the anterior ethmoid and frontal sinuses on the affected side. 6 Above all, the severity of MSFB was positively associated with the occurrence of ipsilateral sinus inflammation and had no effect on the occurrence of sinus inflammation in the contralateral sinuses. Thus, stimulating effect of MSFB on sinus inflammation may be effectuated only through local factors.
Among 159 MSFB patients with COMC, the incidence of sinus inflammation of ethmoid and frontal sinuses on the ipsilateral sinuses was 27.2% and 10.3%, which was higher than 11.2% and 2.1% of the contralateral sinuses, respectively. In the COMC group, the increased inflammation in the ipsilateral sinuses may be due to other local causes besides obstruction, which we hypothesized to be the influence of the local microenvironment. The middle meatus agreed in culture comparison studies with the maxillary sinus and is a fair representation of the underlying sinuses in chronic rhinosinusitis (CRS).7,8 The total bacterial load in healthy and diseased sinuses was similar in adults. 9 However, high interindividual microbiome variation is often observed in healthy controls and CRS patients. 10 The microbiota of patients with CRS had reduced diversity and abundance of bacteria, which could be related to the state and prognosis of the disease. 11 A cross-sectional study of CRS and non-CRS patients who underwent endoscopic sinus surgery demonstrated a correlation between loss of bacterial species richness and diversity and severity of inflammation and tissue eosinophilia. Bacterial community dysbiosis was more apparent in fungal rhinosinusitis samples and was limited to the middle meatus. 12 Moreover, haemophilus was associated with FB. Haemophilus was overrepresented in FB compared to non-fungal rhinosinusitis. The pathogenesis of FB could result from fungi–bacteria interactions in a mixed biofilm-like structure. 13 In addition, dysfunctional glycerophospholipid and sphingolipid metabolism is present in the lesion of fungal ball sinusitis. 14 FB group differed from the chronic rhinosinusitis with nasal polyps (CRSwNP) group, and the healthy controls in terms of microbial diversity. Neisseria abundance revealed the most significant difference in the FB group compared with other groups. 15 The possible role of microbial dysbiosis as a pathogenetic mechanism of nasal mucosal inflammation needs to be confirmed further. We believed that changes in the microbiota of the middle nasal meatus in the COMC group were associated with sinus inflammation in anterior sinuses.
Among the 895 MSFB patients with OOMC, all patients had sinus inflammation in the ipsilateral anterior ethmoid sinuses, and 122 (13.6%) patients had sinus inflammation in the contralateral ethmoid sinuses. Furthermore, sinus inflammation was seen in 299 (33.4%) ipsilateral frontal sinuses and in 37 (4.1% ) contralateral frontal sinuses. The difference in the incidence of ipsilateral and contralateral paranasal sinus inflammation was statistically significant. The ostiomeatal complex is a functional entity of the anterior ethmoid complex that is the final common pathway for drainage and ventilation of the frontal, maxillary, and anterior ethmoid cells. We speculated that the obstruction of ostiomeatal complex effectuated the sinus inflammation of the ethmoid sinuses and frontal sinuses on the ipsilateral side of MSFB. In addition, the change in local microorganisms might lead to greater sinus inflammation incidences in the ipsilateral ethmoid sinuses and frontal sinuses in the OOMC group.
The sphenoethmoidal recess is located in the posterior-most aspect of the nasal cavity between the nasal septum and superior turbinate. The ground plate or lamella of the middle turbinate is the most significant bony partition, dividing the cells into anterior and posterior groups. The drainage from the posterior ethmoid and sphenoid sinuses flows through the sphenoethmoidal recess. Due to the anatomical barrier of the lamella of the middle turbinate, the MSFB does not affect the microbial environment of sphenoethmoidal recess. Our study showed that sinus inflammation occurred in 4.2% of ipsilateral sphenoid sinuses and 2.1% of contralateral sphenoid sinuses in the COMC group, and no significant difference was observed in the incidence of sinus inflammation between the bilateral sphenoid sinuses in the COMC group. However, in the OOMC group, 10.7% of patients had sinus inflammation in the ipsilateral sphenoid sinuses, and 4.0% had sinus inflammation in the contralateral sphenoid sinuses. The difference between the 2 groups was statistically significant. The possible reason is that in the OOMC group, a subgroup had FB protruded beyond the ostiomeatal complex, causing compression and medial displacement of the superior turbinate, thus interfering with the drainage of the posterior sinuses. This phenomenon explained why sinus inflammation was more common in the ipsilateral sphenoid sinuses than in the contralateral sphenoid sinuses in the OOMC group. The pity is, we were not able to compare the CT findings of the sinuses in the population with those on the contralateral side of FB. The severity of FB did not show an effect on the presence of contralateral disease, but the presence of FB may have an effect on the presence of contralateral disease.
In the ipsilateral nasal cavity of MSFB, the incidence of NPs was 18.0% in the OOMC group and 0.3% in the COMC group. The incidence of NPs was higher in the ipsilateral nasal cavity for the OOMC group. On the contralateral nasal cavity of the MSFB with OOMC, NPs had an incidence of only 0.4%, while no NPs were detected in the COMC group. Ponikau et al 16 proposed that fungi are the drivers of inflammation in all CRS. Boase et al 17 detected fungi in CRSwNP patients but not in chronic rhinosinusitis without nasal polyps (CRSsNP) or controls. Aspergillus fumigatus and Demodex curveatus are the fungal genera detected in CRSwNP patients, indicating that fungi are associated with NPs formation. 17 However, other studies did not show any difference in the abundance of fungal species between CRS and controls.18,19 Negative clinical trials have cast doubt on the critical pathogenic role of fungi in the immunopathology of CRSwNP. A previous study in China showed that 10% of FB patients develop NPs. 20 The role of fungi in driving local inflammatory immune response and NPs formation is yet to be explored. Based on the current data, we presumed that the high proportion of NPs in the ipsilateral nasal cavity of the OOMC group was due to local obstruction rather than fungi stimulus. The only case in the COMC group was confirmed as an antrochoanal polyp. This phenomenon suggested that simple ostiomeatal complex obstruction gives rise to FB with NPs. European Position Paper on Rhinosinusitis and Nasal Polyps 2020 pointed out that FB is a secondary localized chronic sinusitis. 21 Our study indicated that FESS relieving ostiomeatal complex obstruction might achieve a good therapeutic effect for NPs associated with FB.
Conclusion
We hypothesized that the stimulating effect of MSFB on sinus inflammation was effectuated only through local factors. In addition to obstruction of the ostiomeatal complex, changes in the local microenvironment may also lead to the occurrence of sinus inflammation. By comparing the incidence of NPs in the OOMC group and the COMC group, we considered that the NPs ipsilateral to MSFB was caused by local obstruction.
Footnotes
Acknowledgements
We acknowledge the reviewers for their helpful comments on this article.
Author’s Contributions
Chengyao Liu and Ting Yang: contributed to study design, acquisition, analysis, and interpretation of data, and drafting of the article; Yun Zeng, Pengyu Shi, and Yi Wang: contributed to acquisition and interpretation of data; and Yunchuan Li and Hongzheng Wei contributed to study design and interpretation of the data and revision of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Beijing Natural Science Foundation of China (approval number: 22G10194).
Ethical Approval
The study was approved by the medical ethics committee of Beijing Tongren Hospital.
Informed Consent
Written informed consent was obtained from each patient before participation.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.