
Abstract
Significance Statement
Pilomatricoma is a benign tumor of the hair follicle matrix cells. Pilomatricoma in the preauricular area is difficult to diagnose preoperatively as most clinicians lack knowledge of this entity and confuse it with other tumors. Pilomatricoma should be considered in the differential diagnosis of any nodular mass located in the preauricular area in young female patients. To increase the incidence of correct preoperative diagnoses and appropriate treatment, otolaryngologists must be aware of this entity.
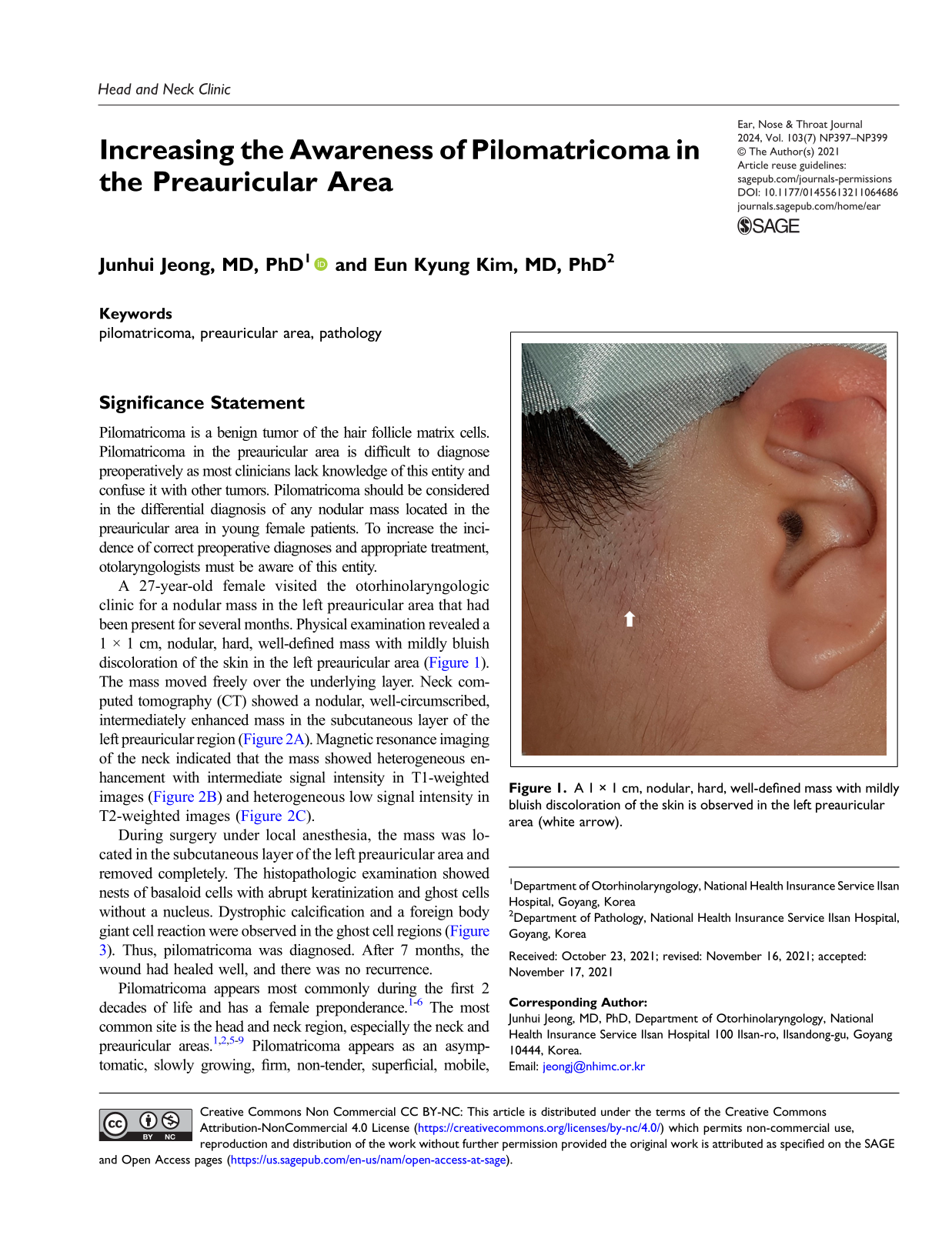
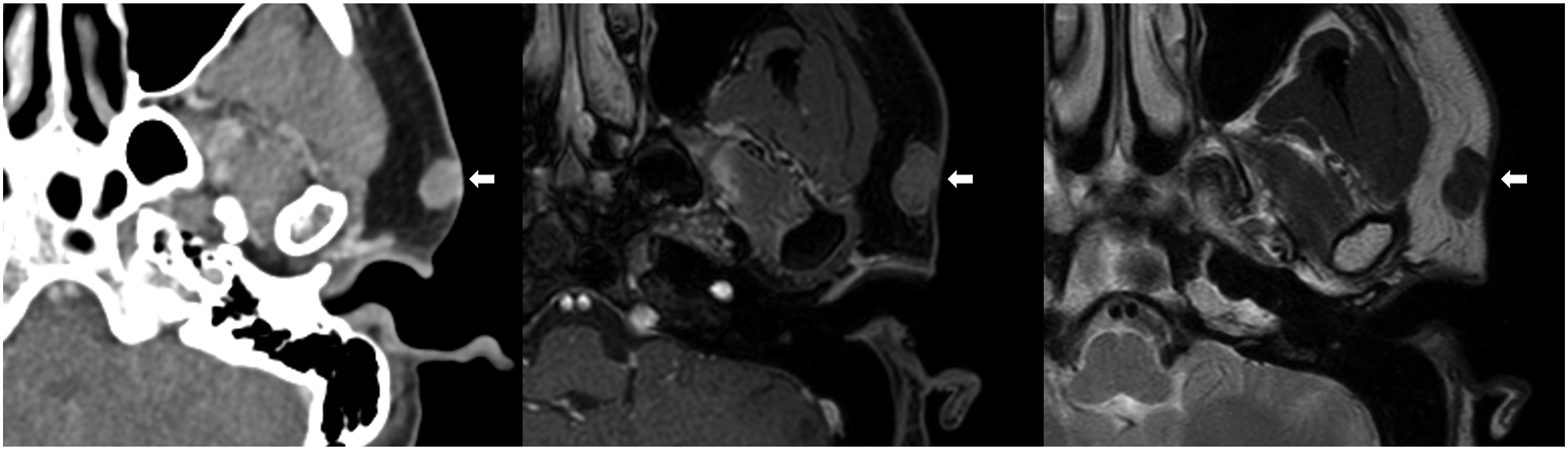
A 27-year-old female visited the otorhinolaryngologic clinic for a nodular mass in the left preauricular area that had been present for several months. Physical examination revealed a 1 × 1 cm, nodular, hard, well-defined mass with mildly bluish discoloration of the skin in the left preauricular area (Figure 1). The mass moved freely over the underlying layer. Neck computed tomography (CT) showed a nodular, well-circumscribed, intermediately enhanced mass in the subcutaneous layer of the left preauricular region (Figure 2A). Magnetic resonance imaging of the neck indicated that the mass showed heterogeneous enhancement with intermediate signal intensity in T1-weighted images (Figure 2B) and heterogeneous low signal intensity in T2-weighted images (Figure 2C). A 1 × 1 cm, nodular, hard, well-defined mass with mildly bluish discoloration of the skin is observed in the left preauricular area (white arrow). (A) Neck computed tomography reveals a nodular, well-circumscribed, intermediately enhanced mass in the subcutaneous layer of the left preauricular area. (B) Neck magnetic resonance imaging shows a mass with heterogeneous enhancement and intermediate signal intensity in T1-weighted images and (C) heterogeneous low signal intensity in T2-weighted images (masses are indicated with white arrows).
During surgery under local anesthesia, the mass was located in the subcutaneous layer of the left preauricular area and removed completely. The histopathologic examination showed nests of basaloid cells with abrupt keratinization and ghost cells without a nucleus. Dystrophic calcification and a foreign body giant cell reaction were observed in the ghost cell regions (Figure 3). Thus, pilomatricoma was diagnosed. After 7 months, the wound had healed well, and there was no recurrence. Histopathologic examination shows nests of basaloid cells with abrupt keratinization and characteristic ghost cells along with a foreign body giant cell reaction (hematoxylin-eosin, × 100).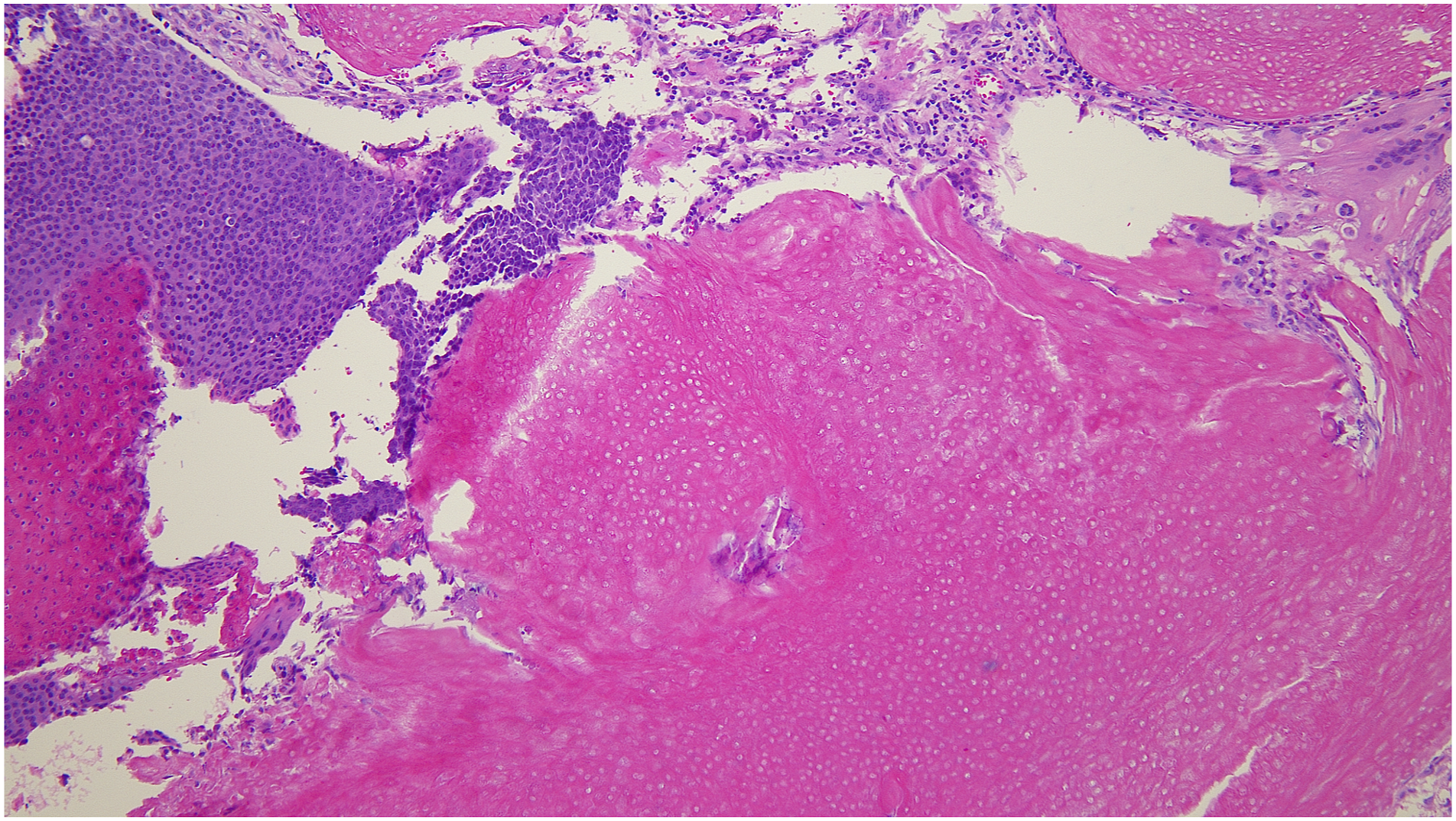
Pilomatricoma appears most commonly during the first 2 decades of life and has a female preponderance.1-6 The most common site is the head and neck region, especially the neck and preauricular areas.1,2,5-9 Pilomatricoma appears as an asymptomatic, slowly growing, firm, non-tender, superficial, mobile, well-circumscribed single nodule with bluish-reddish skin discoloration.1-3,5-7,10 This tumor can be fixed to the overlying skin1,3,5 and slides freely over the underlying soft tissue.1,5,7 These masses have an irregular and angulated shape when stretched, which is called the tent sign.1,5,6,10 When one edge of the mass is pressed, the opposite edge is displaced, which is called the teeter-totter sign. Tent signs and teeter-totter signs are the most helpful physical examination findings in diagnosis of pilomatricoma. 5
The exact pathogenesis of pilomatricoma is unknown. 4 However, mutation of the CTNNB1 gene, which encodes beta-catenin, might play a role.3,4,8,11,12 Multiple pilomatricomas can be associated with Gardner syndrome, Turner syndrome, Rubinstein-Taybi syndrome, myotonic dystrophy, and Steinert disease.1,6,7,9,10,12
Radiologic evaluation has a limited value in diagnosis of pilomatricoma.1,5-7 The primary reason for radiological exams is to differentiate preauricular tumors from parotid tumors.3,6,7,10 Pilomatricoma presents as a sharply demarcated, calcified, subcutaneous nodule with mild to moderate enhancement on CT.1,4-7,10,12 Magnetic resonance imaging shows inconsistent characteristics. 5 However, it is reported commonly that these entities appear as homogeneous masses with an intermediate signal intensity in T1-weighted images and as heterogeneous masses with intermediate signal intensity in T2-weighted images.1,4,5
The treatment of choice is complete surgical excision.1,2,4-10,12 Recurrence is rare after complete excision.1,4-10,12 Malignant transformation has been reported after repeated recurrent tumor excision.2,3 Pilomatricoma in the head and neck should be differentiated from sebaceous cyst, ossifying hematoma, hemangioma, epidermoid cyst, dermoid cyst, trichilemmal cyst, preauricular sinus, degenerating fibroxanthoma, foreign body reaction, and basal cell carcinoma.1-3,5,7,8,10-12 For pilomatricoma that occurs in the preauricular area, salivary gland tumors composed of basaloid cells, such as pleomorphic adenoma, basal cell adenoma, basal cell adenocarcinoma, adenoid cystic carcinoma, and mucoepidermoid carcinoma, should be ruled out. 3
Pilomatricoma can be misdiagnosed as a malignancy based on cytology from fine-needle aspiration if there are predominant basaloid cells without ghost cells in the aspirate.1,5-7,9,10,13 Histopathology can reveal sharply demarcated nodules surrounded by a capsule of compressed fibrous tissue in the lower dermis.5-7,10,12 There are basaloid cells with a nucleus in the periphery, and ghost cells or shadow cells without a nucleus in the center.1,3-7,9,10,12 Calcification can be observed in ghost cell regions,3,6,7,9,10,12 and foreign body giant cell reactions often are identified in regions with keratinized debris.4-7,10
For preauricular nodular masses that move freely over the underlying layer in young female patients, pilomatricoma should be included in the differential diagnosis. However, clinicians without knowledge of pilomatricoma initially can suspect these as parotid gland tumors upon physical examination. The rate of correct preoperative diagnosis for pilomatricoma has been reported to be less than 30%.2,5,7,8,14 Otolaryngologists need improved understanding of its discriminative appearance, predominant age and sex, and characteristic radiologic findings to diagnose this entity more accurately.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Institutional Review Board of the National Health Insurance Service Ilsan Hospital exempted the review of this study (NHIMC 2021-09-033).