
Abstract
This report describes a case of stapedial superstructure fixation with a mobile footplate, which is a rare occurrence among the ossicular malformations that cause conductive hearing impairment. A 44-year-old man with symptoms of left-sided hearing impairment since childhood presented to our department. The eardrum was normal, and pure tone audiometry showed conductive hearing impairment with a three-frequency (500, 1000, and 2000 Hz) mean of 53.3 dB and a normal tympanogram result. An abnormal shadow was observed on the internal side of the left stapes during the three-dimensional reconstruction of computed tomography. We suspected a stapes malformation and performed an exploratory tympanotomy with transcanal endoscopic ear surgery. We found a bony bar between the superstructure of the stapes and the promontory. The mobility of the stapes was significantly improved by removing the bony bar. Findings of postoperative audiometry were normal after surgery. The treatment of such cases of stapedial fixation is simple, and the prognosis of hearing gain after surgery is quite good. Thus, regarding the treatment of patients with conductive hearing impairment, clinicians and surgeons should be aware of the possibility of single stapedial superstructure fixation.
Introduction
Conductive hearing impairment can be caused by various factors, such as infection, trauma, and malformation of the ear. Even if there are no anomalies in the external ear, ossicular malformations can be considered a cause of conductive hearing impairment. Stapedial malformations are the most common congenital middle ear anomalies. 1 Among them, footplate fixation and superstructure defects are the most common. However, there have been only a few reports of stapedial superstructure fixation with a bony bar and mobile footplate.2-16
Here, we report a rare case of a bony bar between the stapes and the promontory with a normal stapedial superstructure and mobile footplate and present a comprehensive review of literature.
Case Report
A 44-year-old man presented to our hospital with symptoms of left-sided hearing impairment since childhood. He had no other medical or family history of hearing impairments. There were no abnormal findings or significant malformations in the eardrum, external auditory canal (EAC), or auricle on the left side.
Pure tone audiometry showed conductive hearing impairment with a three-frequency (500, 1000, and 2000 Hz) mean of 53.3 dB, stiffness curve, and decline in bone-conduction threshold with Carhart’s notch (Figure 1). Tympanogram results were normal. Temporal computed tomography (CT) showed well-developed mastoid cells and no abnormalities in the auditory ossicles. However, an abnormal shadow was observed on the internal left stapes on three-dimensional (3D) reconstruction (Figure 2a). Based on these findings, we suspected a stapes malformation and performed an exploratory tympanotomy with transcanal endoscopic ear surgery. Pure tone audiometry showing conductive hearing impairment with a three-frequency mean of 53.3 dB, stiffness curve, and decline in bone-conduction threshold. Recovery of these findings after surgery and normalization of pure tone audiometry readings with a three-frequency mean of 16.7 dB. An abnormal shadow is observed on the left internal stapes in three-dimensional reconstruction of computed tomography (a). The stapes is fixed to the promontory with a bony bar (b). By removing the bony bar (c), stapes mobility improved radically. Black arrow indicates a bony bar. CTN, chorda tympani nerve; EAC, external auditory canal; P, promontory.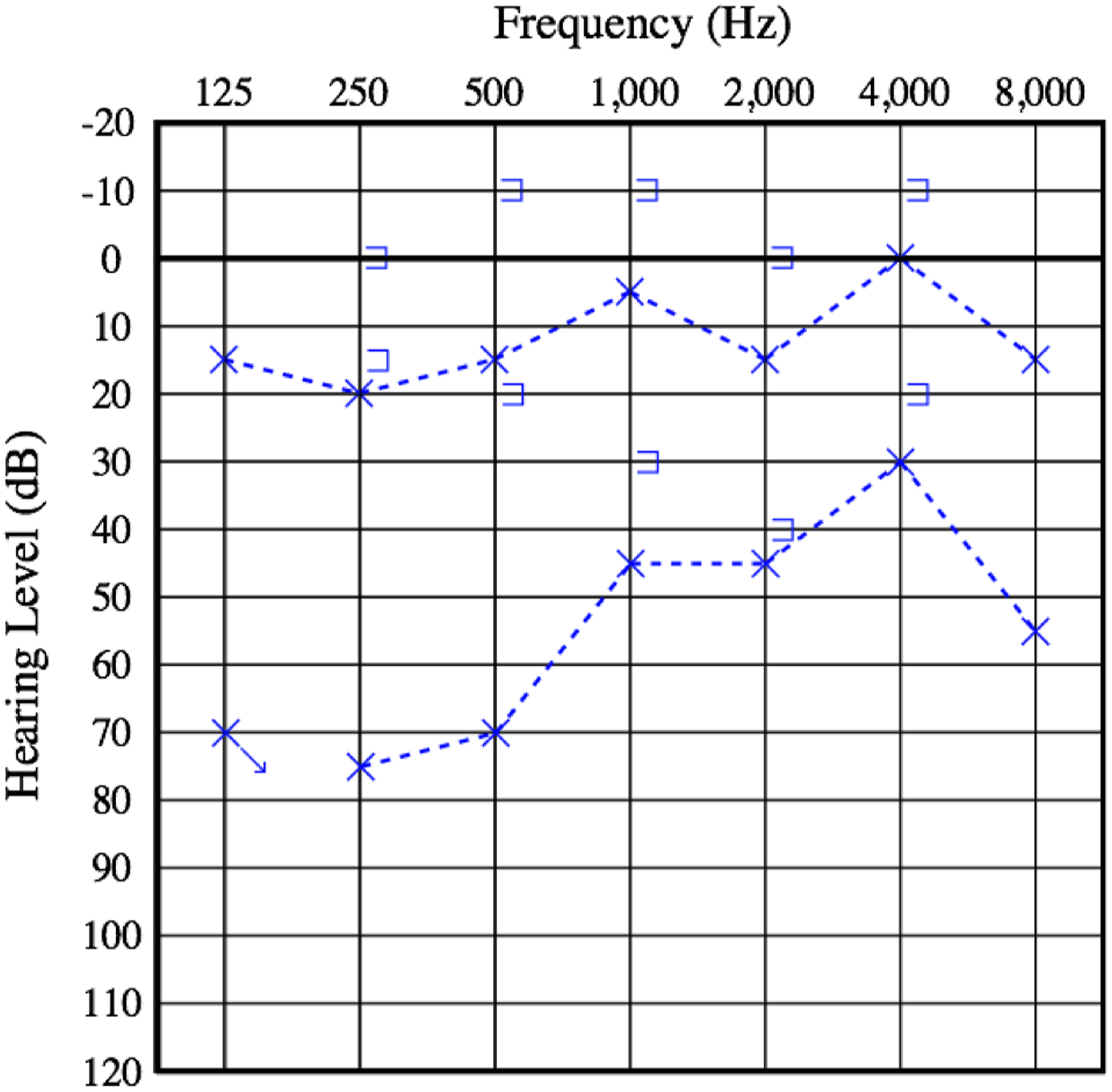
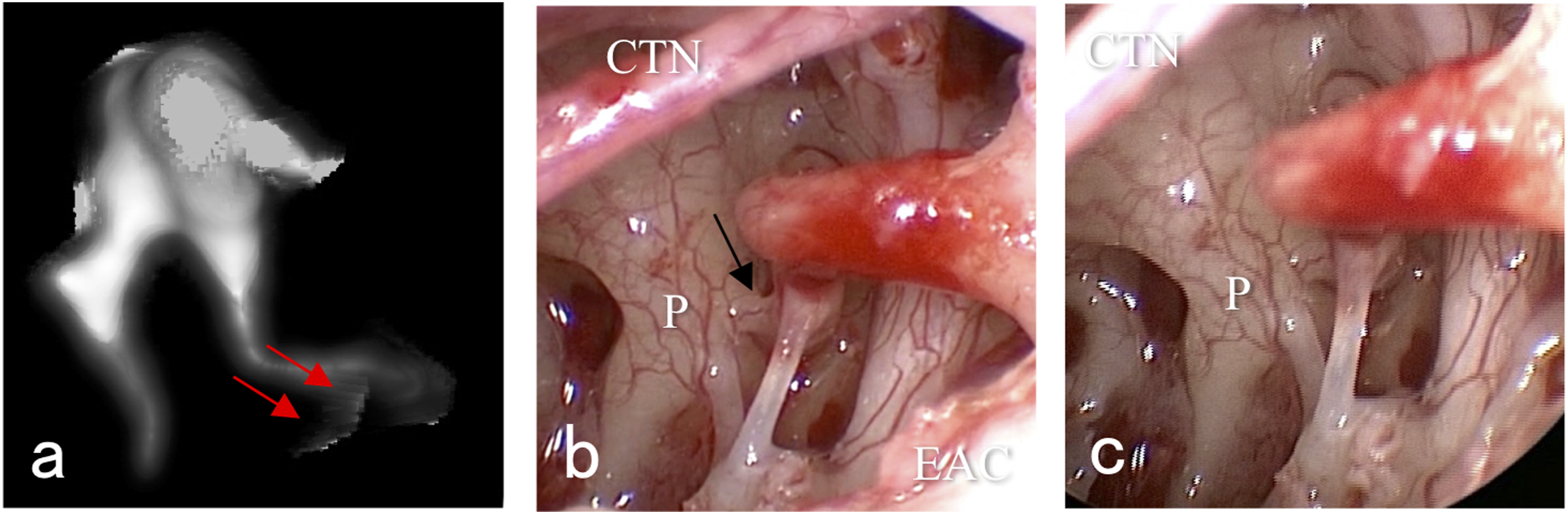
During surgery, no abnormal findings were observed in the EAC or eardrum. The shape and mobility of the malleus and incus were normal. However, the stapedial superstructure was completely fixed to the promontory with a bony bar (Figure 2b). Since the bony bar was fragile, it could easily be removed (Figure 2c), which improved the mobility of the stapes significantly. The postoperative clinical course was uneventful, and the patient was discharged the following day. Postoperative pure tone audiometry showed improvement in conductive hearing impairment with a three-frequency mean of 16.7 dB 6 months after the operation (Figure 1).
Discussion
There are many types of malformations of the ear involving the auricle, EAC, and middle ear. Congenital ossicular malformation is a rare disease that occurs in less than 1 in 15000 people. 17 Among these malformations, stapes malformation is the most common middle ear abnormality. 1 Cauldwell and Anson hypothesized that stapes malformation can have two different origins: the first or second branchial arch.18,19 Although the theory of disturbance in the development process of the stapes is controversial, our case supports this theory. The development of auditory ossicles begins around 5–6 weeks of fetal life. The ossicles originate from Meckel’s cartilage of the first branchial arch and Reichert’s cartilage of the second branchial arch. The stapes originates from the lateral end of Reichert’s cartilage. In the present case, no malformations were observed in the ossicles other than the stapes; thus, it was considered that the malformation originated from the second branchial arch. The development of the stapes begins around the 5th week of fetal life during which it attaches to the otocyst, pushing it slightly toward the inner surface. This development process causes the lateral wall of the stapes to attach to the mesenchymal tissue of the otocyst, 20 which was thought to be the cause of the fixation between the stapes and the promontory in our case.
Clinical characteristics of reported cases of stapedial superstructure fixation with mobile footplate.
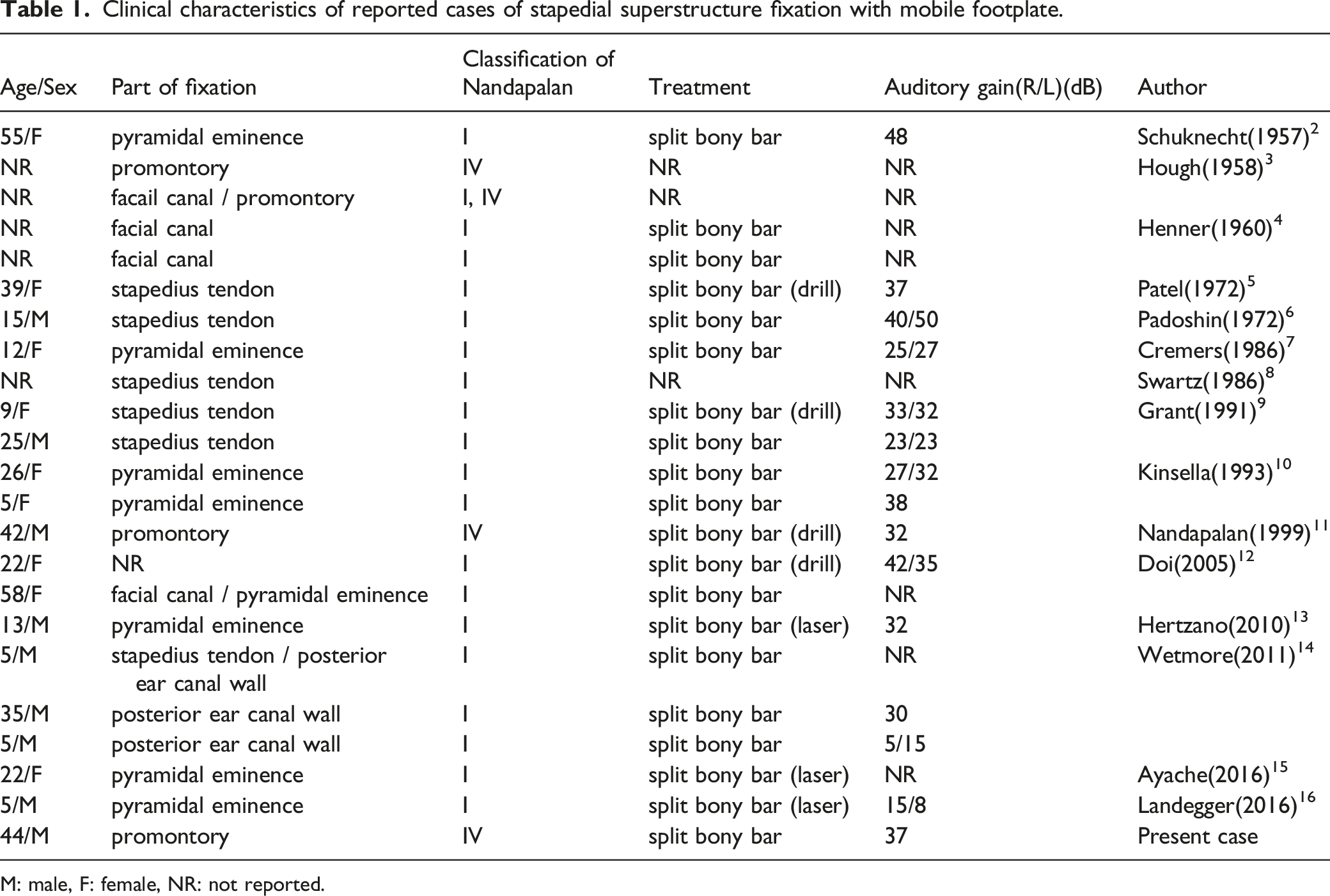
M: male, F: female, NR: not reported.
Among them, a bony bar between the stapes and the promontory was present in only four cases. In the abovementioned 23 cases, the median age of the patients was 22 years, with a wide range of 5–58 years. The male to female ratio was same (9:9). All patients presented with the chief complaint of non-progressive hearing impairment over a long period of time. Trauma, infection, and obvious deformity in appearance were ruled out in advance. Our patient did not have a family history of hearing impairment. To date, there is no sufficient evidence that this condition maybe hereditary. However, some reports have indicated that family history may be relevant.9,10,12,14
Regarding the side of involvement, 13 patients were affected on both sides, three on the right side, and four on the left side. Thin-section CT is useful for the preoperative diagnosis of stapedius ossification, especially the stapedius tendon, which shows soft-tissue attenuation at the bony bar. 21 The axial CT slice shows unremarkable findings, while an abnormal shadow can be seen on 3D reconstruction CT. Due to diversity in malformations, preoperative diagnosis must be performed with some CT configurations. Fixations include the pyramidal eminence, stapedius tendon, facial canal, posterior ear canal wall, and promontory. The connection between the stapedial superstructure and the footplate was observed in all the previously described cases, which were classified according to Teunissen and Cremers classification as class 1. 1 Whereas, 19 cases were classified as class Ⅰ according to the classification by Nandapalan. 20 The present case is extremely rare and was classified as class IV that was seen only three other cases. All the 23 patients were treated by splitting the bony bar. The present case was also treated similarly because the bony bar was fragile, and there was a connection between the superstructure and the mobile footplate without any other ossicular malformation. The average of the auditory gain of 30 dB in 23 patients, which was calculated from preoperative and postoperative audiometry, indicating that an improvement of 37 dB in our patient is appropriate. The prognosis of hearing gain after surgery in patients with a mobile footplate without other anomalies is significantly better than that in patients with other ossicular malformations. 22
Our case was performed under endoscopic surgery, which was very useful in observing the condition of the stapes and footplate mobility. In this case, the bony bar was easily removed during observation with a raspatory as it was very fragile. However, if the bony bar is solid, a laser13,15,16 or a drill5,9,11,12 should be used to reduce damage to the inner ear. Although there is only one report of these being used in the fixation to the promontory, 11 overall reports of stapedial superstructure fixation indicate that the use of laser or drill is expected to increase in the future.
In summary, we encountered a rare case of fixation caused by a bony bar between the stapedial superstructure and promontory which was captured by 3D CT. We hypothesized that this was caused by the partial adherence of the stapes primordium and endosteal ossicles during the embryonic period. It was treated by splitting only the bony bar because there was a connection between the stapedial superstructure and the mobile footplate, without any other ossicular malformation. Endoscopic surgery was useful in showing a clear view of the surgical field in our case. We also reviewed previous cases of stapedial superstructure fixation with a mobile footplate to determine patient trends, the relationship between fixation and surgical strategy, and the prognosis for postoperative impairment. In patients with conductive hearing impairment, clinicians and surgeons should be aware of the possibility of single stapedial superstructure fixation with a bony bar.
Footnotes
Declaration of Conflicting Interests
The authors declare that there are no actual or potential conflicts of interest related to this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Ethical Approval
All procedures performed on the patient in this study were in accordance with the ethical standards of the Institute Ethics Committee and the Declaration of Helsinki 1964 and its later amendments or comparable ethical standards. Written informed consent was obtained from the patient and his family for publication of clinical details and images.