
Abstract
Objectives:
Hydroxyapatite is a commonly used material for medical applications due to its excellent biocompatibility. We use hydroxyapatite prosthesis for the reconstruction of the ossicular chain in stapes surgery. In this study, we report a case series of endoscopic ear surgery using a basket-type hydroxyapatite prosthesis.
Methods:
We retrospectively examined 8 cases of endoscopic transcanal stapes surgery using hydroxyapatite prostheses. We evaluated the postoperative results and complications.
Results:
The average postoperative air–bone gaps were within 10 dB in all cases. Postoperative sensorineural hearing loss was not observed in any case. There was an intraoperative complication with the chorda tympani in 1 patient. We were able to preserve the chorda tympani of all patients, including this case. Postoperative transient dizziness and transient taste disorder were observed in 50% of cases. No other complications, including facial nerve palsy, tympanic membrane perforation, or postoperative infection, were observed.
Conclusions:
The postoperative results and complications were comparable to those of surgery under a microscope. The hydroxyapatite prosthesis could be a possible alternative for the piston-type titanium or polytetrafluoroethylene prosthesis.
Introduction
Hydroxyapatite is a commonly used material for medical applications due to its excellent biocompatibility. As this is a nonmagnetic material, it is safe for patients with these implants to undergo magnetic resonance imaging (MRI). Prostheses made of hydroxyapatite have been used for tympanoplasty, stapes surgery, and ossicular chain reconstructions.1,2 High biocompatibility results in low levels of inflammation and fibrosis in the middle ear. 3 However, despite these advantages, the otologic prosthesis with hydroxyapatite is not as popular as other biocompatible materials (eg, titanium or polytetrafluoroethylene [PTFE]).
Recently, the usefulness of transcanal endoscopic ear surgery (TEES) has been widely recognized as it provides a wide viewing angle and close proximity to the object. Stapedectomy or stapedotomy is a good method of endoscopic surgery since in otosclerosis, the lesion is confined to the footplate of stapes. A finer and closer view of stapes footplate under endoscopy permits safe and secure work on the plate, keeping the ossicular chain and tensor tympani totally intact.
In this report, we aimed to discuss the procedure and report the postoperative results of our case series of endoscopic ear surgery using a basket-type hydroxyapatite prosthesis.
Patients and Methods
We retrospectively examined a year of consecutive cases of otologic surgery under general anesthesia by TEES at our hospital between June 2018 and June 2019.
The TEES surgery was used on 49 cases during the 12-month period. Among the cases, 9 cases were performed for otosclerosis cases (8 female and 1 male; mean age 60.6 years). We performed 8 stapes surgeries with prosthesis reconstruction and 1 mobilization surgery. One patient with only mobilization of stapes was excluded from further analysis. Hydroxyapatite prostheses were used for ossicular replacement in the 8 cases. These cases were enrolled in the study for analysis.
For included cases, the following parameters were examined: The rate of tympanic nerve preservation The type and rate of postoperative complications Preoperative and postoperative hearing levels were examined. Mean hearing level was calculated by averaging 500 Hz, 1 kHz, 2 kHz, and 3 kHz. The air–bone gap (ABG) was averaged at 0.5, 1, 2, and 3 kHz using the American Academy of Otolaryngology—Head and Neck Surgery guidelines. The percentage recovery after the procedure was calculated and compared with the best possible recovery (complete closure of the ABG) using the following formula as previously reported:
(preoperative ABG − postoperative ABG) × preoperative ABG × 100.
Surgical Procedure
All procedures were performed under general anesthesia. Slow injection of local anesthesia at the 2 sites of posterior wall (at either side of the predicted tympanomastoid suture) of the external auditory canal was performed. These injections aimed to elevate the thin canal skin released from the bony wall, thus facilitating easier and complete elevation of the tympanomeatal flap (Figure 1A). The posterior bony wall of the external auditory canal was curetted until the footplates of stapes were completely exposed. During the procedure, chorda tympani was identified with special care for preservation and was carefully detached from the surrounding tissue, including malleus and tympanic membrane (Figure 1B). This prevented the nerve from local stretching and damage on subsequent procedures. After confirming stapes fixation, we harvested the perichondrium of the tragus cartilage. In principle, small fenestration stapedotomy was selected. A small hole was created at the center of the footplate with a small Skeeter drill. Afterward, the remaining labyrinth membrane underneath the hole was carefully opened by sharp needles so the pulsing perilymph was released under closer observation. The posterior arch of stapes was cut by the drill, followed by division of the stapedial tendon with small scissors. Finally, the anterior arch was fractured by delicate force. We believe this avoids trauma to the inner ear during the process of small fenestration (Figure 1C and D). 4 In cases where the abovementioned procedure was difficult, we chose total or partial stapedectomy. The hole created on the stapes footplate was covered by prepared perichondrium (Figure 2A) and a cup-shaped hydroxyapatite prosthesis (Apaceram Type C: HOYA Technosurgical) was placed between the hole and the incus. The position of the prosthesis was adjusted by gently pushing it, elevating the perichondrium by a small pick from all directions for the tip of prosthesis located to the opened oval window hole (Figure 2B) and pulling and repositioning incus over the top cup of the prosthesis by Fisch’s hook (Figure 2C and D). The malleus was then carefully palpated to ensure appropriate movement of ossicular chains through the prosthesis to the round window reflex. The tympanomeatal flap was repositioned and sealed with Gelform and cotton gauze with antibiotic ointment.
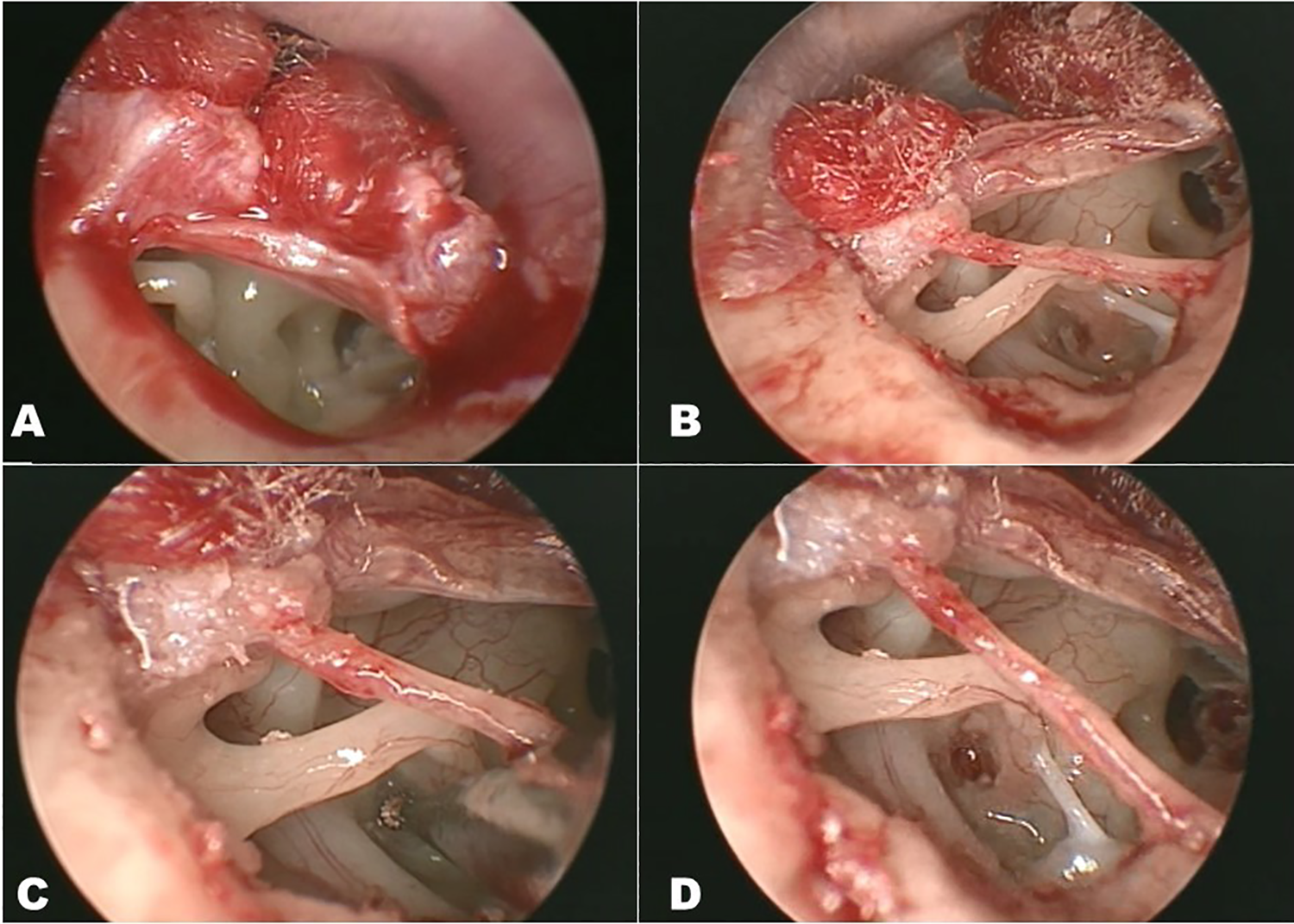
Surgical steps of stapedotomy. Right ear. A, Tympanomeatal flap raising. B, Identification and dissection of chorda tympani. C, D, Drilling of footplate of stapes.
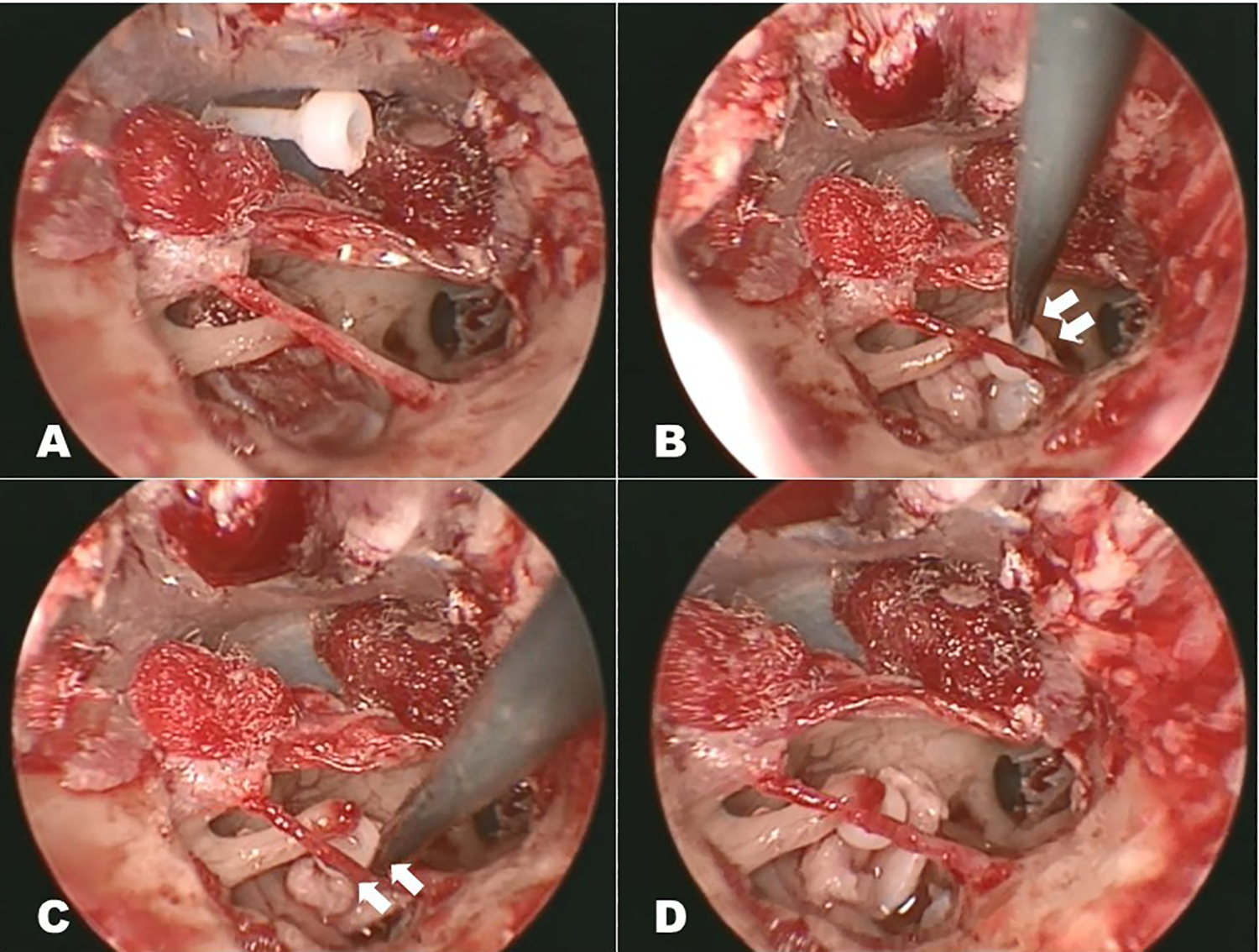
Surgical steps of prosthesis placement. Right ear. A, Seating the perichondrium on the hole. B, Pushing into the hole. C, D, Insertion of the incus into the top cup of prosthesis.
Statistical Analysis
Paired t test was used to compare the preoperative and postoperative hearing level, and P value of <.05 was considered statistically significant.
Results
In our sample, 1 case was a reoperation from another hospital and 7 cases were primary operations. In the primary operation cases, small fenestration stapedotomy was used in 5 (71%) cases, and 2 (29%) cases resulted in partial stapedectomy. The mean age of the patients was 61.6 (range 53-77) years old.
In primary operation cases, preoperative average bone conduction thresholds were 41.3 ± 11.2 dB preoperatively and 32.1 ± 13.1 dB postoperatively (P = .034). Postoperative sensorineural hearing loss was not observed in any case. The average postoperative ABGs were within 10 dB in all 7 cases (Figure 3). In the reoperative case, the average postoperative ABGs were within 10 dB.
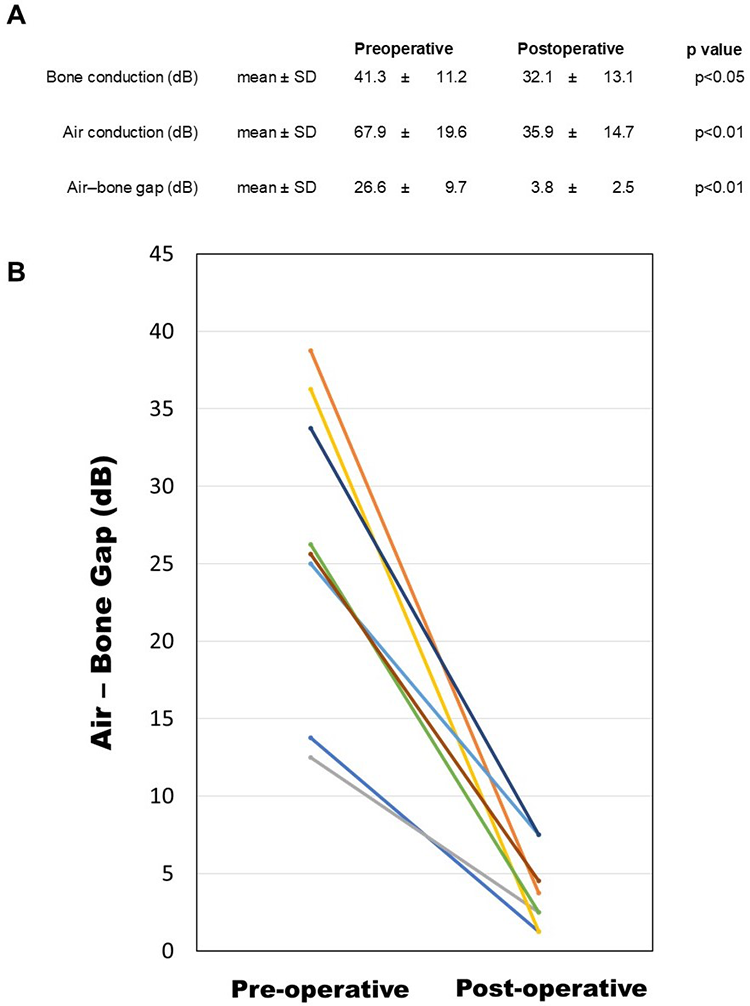
Comparison of preoperative and postoperative hearing level. A, Preoperative and postoperative audiological results. B, Preoperative and postoperative air–bone gap in each case were shown. Postoperative air–bone gap is significantly reduced.
An intraoperative complication was observed in one patient when the chorda tympani was slightly damaged by the heat from the drill. However, we were able to preserve the chorda tympani of all patients, including this case. Postoperative dizziness was observed in 4 (50%) patients, which resolved within 3 days. Postoperative taste disorder was observed in 4 (50%) patients. All taste disorders resolved within 2 weeks, except for 1 case that resolved by 4 months after operation. No other complications, including facial nerve palsy, tympanic membrane perforation, or postoperative infection, were observed (Figure 4).
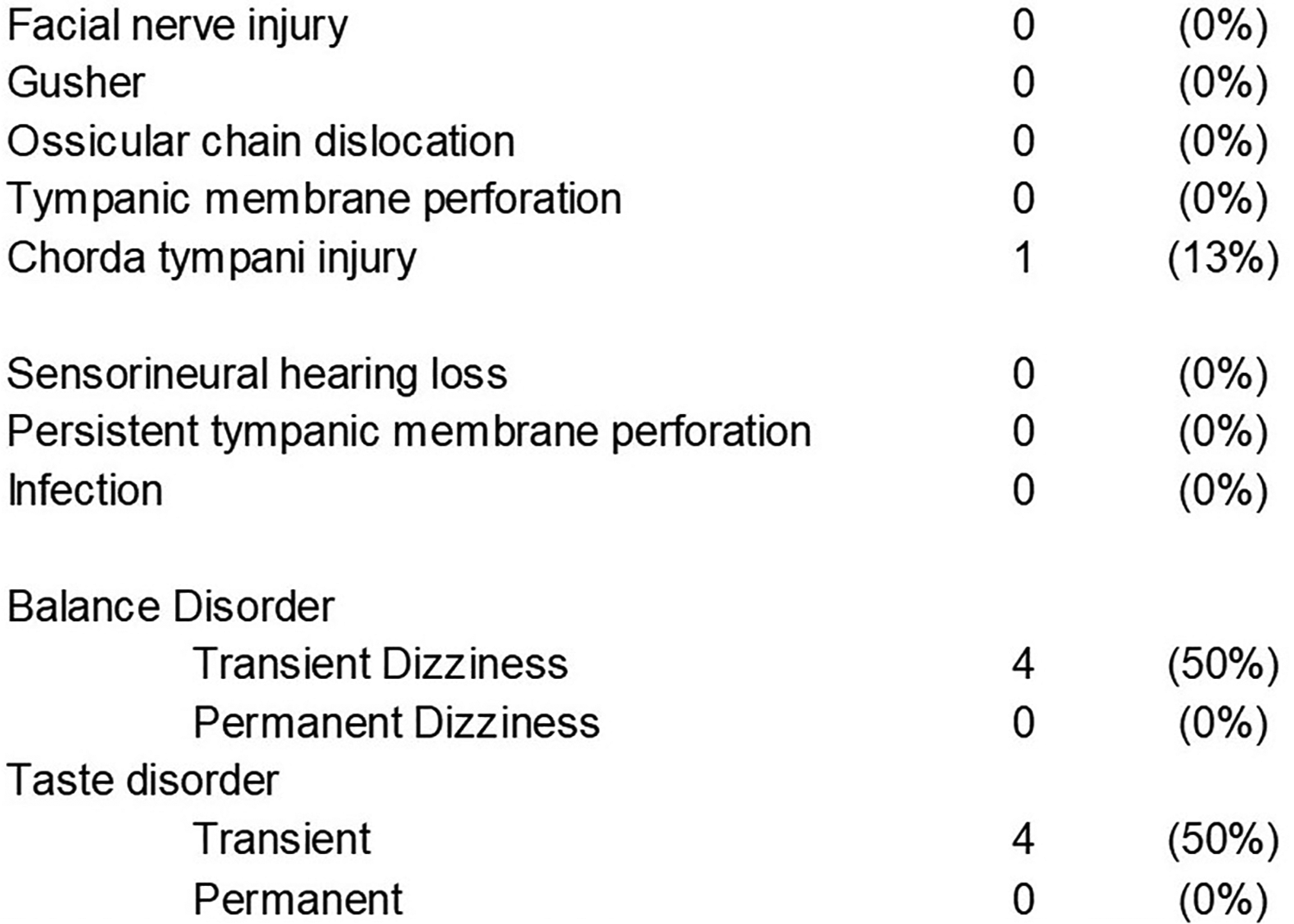
Intraoperative and postoperative complications in this study.
In our study, the average recovery rate in hearing was 85.15% of the maximum expected recovery. All 8 patients achieved an ABG closure of >50% and lower than 10 dB. Changes in the average pure tone audiometry thresholds of all patients are documented in Figure 3B.
Discussion
In general, the success rate in hearing with stapes surgery performed under the microscope is around 90%. 5 Although this study has a small number of cases, comparable results (8/8 cases) were obtained after endoscopic surgery using the hydroxyapatite prosthesis. Moreover, no permanent complication was observed after more than 1 year of follow-up.
Several materials have been tried for stapes prostheses,6,7 and thus far, titanium, titanium-based alloy, and PTFE are predominantly used worldwide. Steel was broadly used, but had been replaced by other MRI-tolerable nonmagnetic materials. 6 Gold, platinum, tantalum, and molybdenum were replaced as they were expensive, hard, and heavy.7-9 On the other hand, titanium is a nonmagnetic MRI-tolerable material and has relatively low cost. The lightweight of titanium is also suitable for the stapes prosthesis. 9 However, titanium has a disadvantage; it is stiff, hard, and difficult to shave. Thus, it is not adjustable during the surgery. Titanium–nickel alloy is, therefore, used as an alternative due to its shape-memory features10,11 so that the prosthesis can be adjusted by heat activation during the ossiculoplasty. However, the nickel can be a cause of metal allergy. 12 The PTFE is another well-used material for stapes prosthesis. It can be used for MRI because it is a nonmetallic material. Brar et al 13 reported that the time-tested, readily available, and cost-effective PTFE piston have equivocal results to the nickel–titanium alloy prosthesis. Bansal 14 reported that there was no obvious difference in the postoperative hearing result of PTFE and titanium prosthesis.
In the reports presented, we used another nonmetallic biocompatible material, hydroxyapatite for the ossiculoplasty. This material is chemically similar to the natural bone and thus has a high affinity to connective tissues.15,16 Truy et al 17 reported that hydroxyapatite prosthesis showed good functional results, stability, and low exclusion rates, with no statistically significant differences between the hydroxyapatite and titanium prostheses. In this report, we used this prosthesis for the endoscopic stapes surgery. The advantages and disadvantages of well-used materials for stapes prostheses are shown in Figure 5.
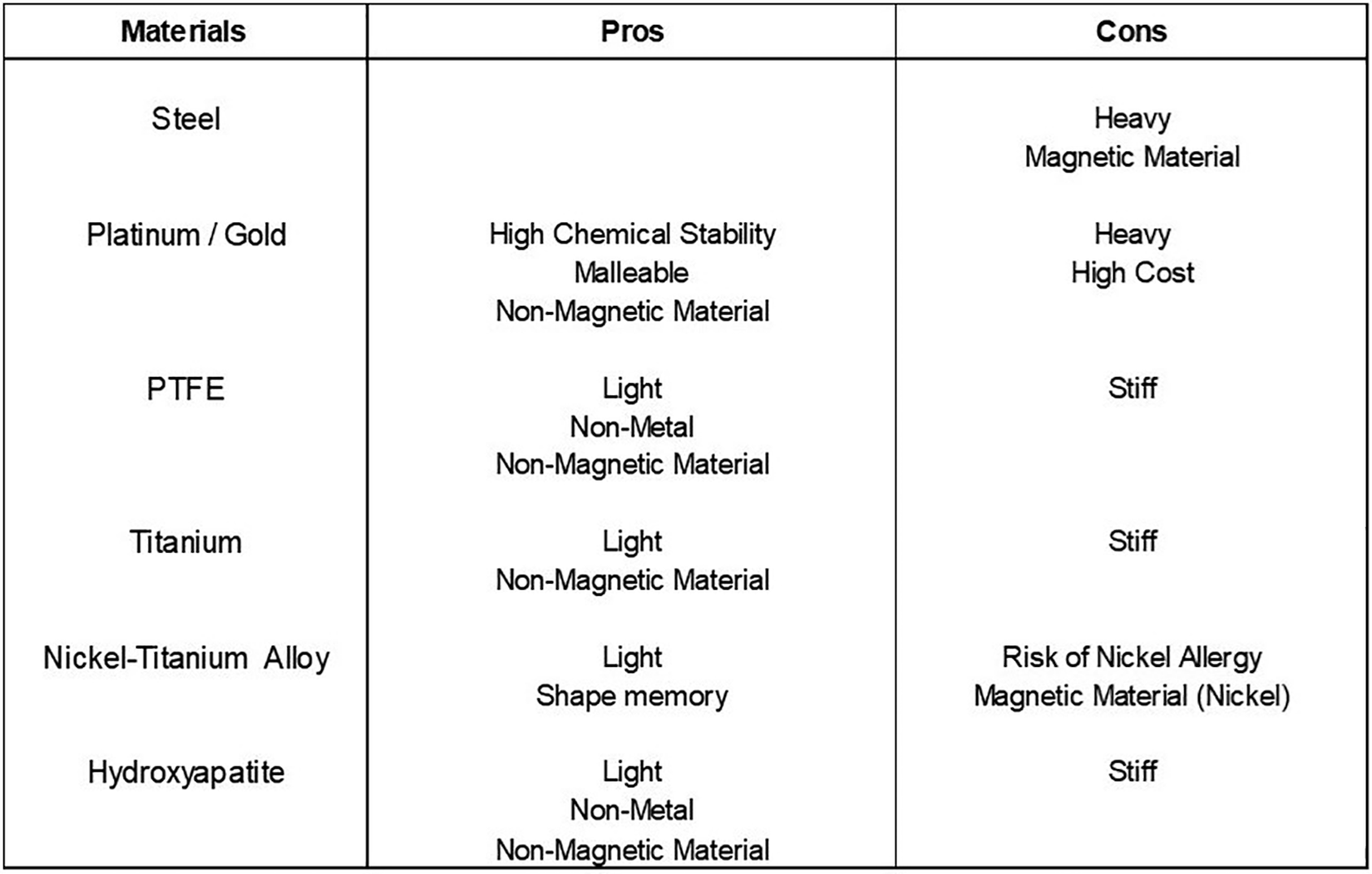
Pros and cons of materials used in stapes prostheses.
We believe that the endoscopic approach provides a clear and high-resolution view, which helps the surgeons perform a better and safer procedure. Fine and closer view of stapes footplate under endoscopic approach enables us to work on the plate and to carefully drill when opening the stapes footplate, leaving the ossicular chain and tensor tympani completely intact. In most cases, the procedures can be performed under direct observation. Thin and fragile epithelium beneath the bony footplate can be preserved by a careful opening after drilling. In the case of stapedectomy, the distance to the macular can be estimated by direct observation. Several groups reported the usefulness of endoscopic approach for stapes surgery (Figure 6).18-35
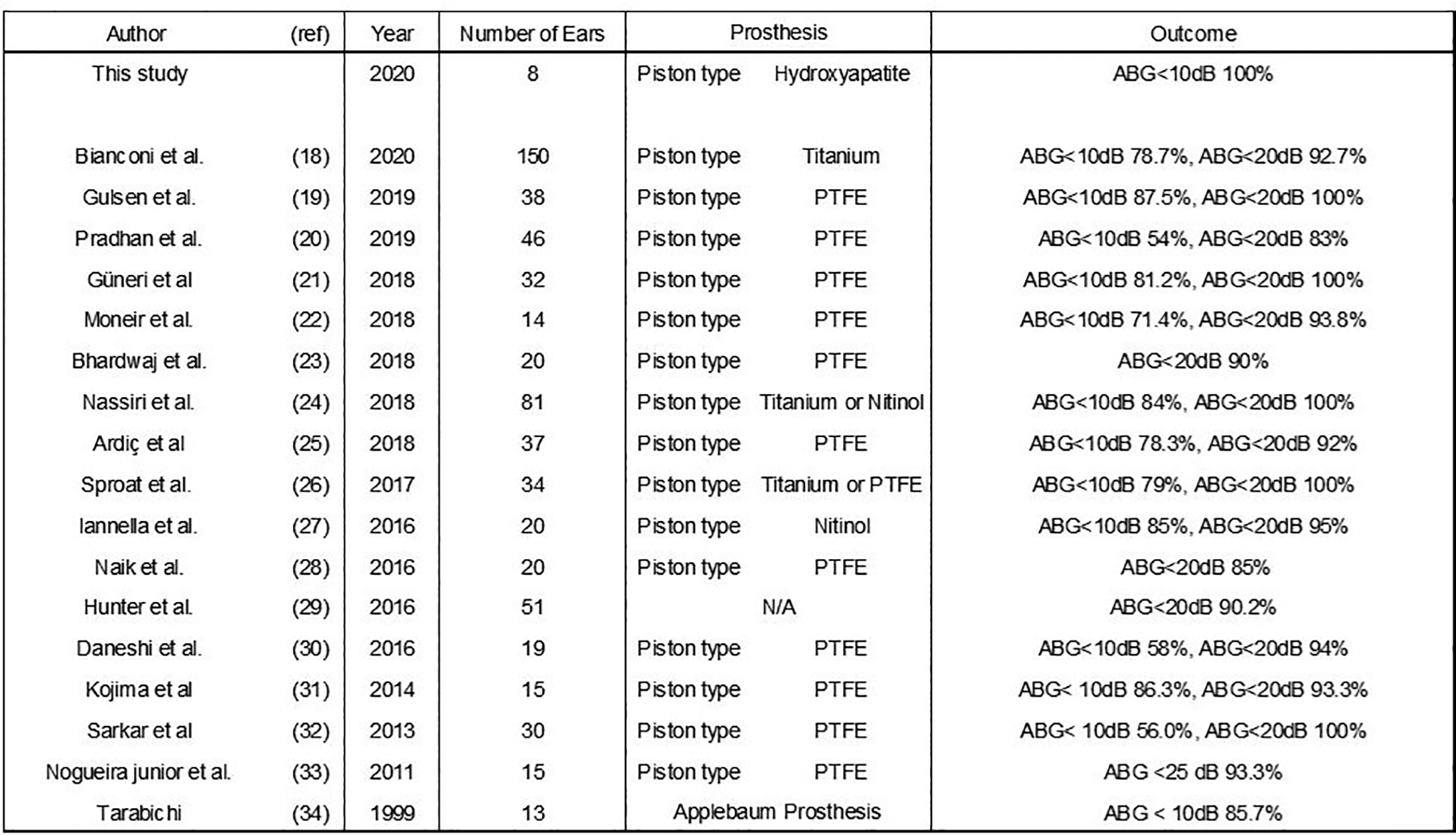
Previous case series of endoscopic stapes surgery.
There are several potential dilemmas for the surgeon when considering TEES. The nondominant hand of the surgeon is used for the endoscopic operation, leaving only 1 hand for the TEES surgery. In using hydroxyapatite prosthesis, the tip of the prosthesis is pushed through the perichondrium membrane seated on the hole made in the footplate of stapes and the cup part into incus. On the other hand, in a piston-wire type prosthesis, “hooking” the hook part into the malleus is more comfortable than one-handed operation. This surgery requires becoming accustomed to handling with one hand and to be familiar with the depth sensation peculiar to an endoscope.
Previous case series of endoscopic stapes surgery with more than 10 cases are shown in Figure 6.18-34 Most surgeons have used piston-type PTFE prosthesis or titanium (or its alloy: nitinol) prosthesis. Whichever prosthesis was used, good surgical results were reported. Gulsen and Karatas 19 and Pradron and Preetam 20 reported the acceptable results with PTFE prosthesis. Sproat et al 26 and Iannella and Magliulo 27 reported the satisfactory surgical results of endoscopic stapes surgery using titanium prosthesis. Recently, Bianconi et al7-18 reported the surgical results of 150 stapes surgery by TEES. They concluded that endoscopic stapes surgery is a safe procedure with a low risk of perioperative or postoperative complications and is a possible alternative to the traditional microscopic surgical procedure in the treatment of otosclerosis. In their study, a piston-type titanium prosthesis was used for reconstruction of ossicular chain. They reported an ABG percentage recovery rate of 73.85%.
In contrast, we used hydroxyapatite prosthesis and our percentage recovery rate was 85.15% in the primary surgical cases. Our result indicates that hydroxyapatite prosthesis could be a possible alternative for piston-type PTFE or titanium prosthesis.
The number of cases in this study is limited, and we believe that a larger study should be conducted in the future.
Conclusion
The postoperative results and complications of endoscopic transcanal stapes surgeries using hydroxyapatite prostheses were comparable to those of surgery under a microscope with other prostheses. Our result indicates that hydroxyapatite prosthesis could be a possible alternative.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.