
Abstract
It is important for medical providers to distinguish between accidental and abusive mechanisms of injury in children. In the absence of a serious trauma, an isolated tongue laceration and oromaxillofacial trauma in a young, edentulous infant raises significant concern for abuse. The presented case demonstrates a unique injury pattern and serves as an opportunity to explore the multidisciplinary approach to infant trauma in Otolaryngology. Presented is an edentulous infant who sustained a deep splitting laceration of the oral tongue as a result of being dropped a short distance onto carpeted floor. This injury pattern, in the absence of other trauma, raised concern for abuse. Hospital social work and Child Abuse Pediatrics further investigated the matter. A surveillance camera video was produced which demonstrated the blunt force of the fall, coupled with the friction sliding on the floor, ripped open the infant's tongue and left a pattern otherwise suspicious for sharp object laceration. To our knowledge, this is the first report describing a full-thickness tongue laceration after a fall from a caregiver’s arms onto carpeted ground. This case underscores the responsibility of the astute provider coupled with a multidisciplinary team to identify or rule out potential child abuse.
Introduction
Trauma from unintentional injury is the leading cause of morbidity and mortality among the pediatric population in the United States. 1 Traumatic injuries to the face are usually the result of motor vehicle accidents, falls, sports injuries, or abuse. In the absence of a serious trauma, an isolated tongue laceration in a young, edentulous infant raises significant concern for inflicted injury or abuse. In cases where the latter is suspected, the treating provider is mandated by law to report to child protective services and/or law enforcement.
We present a case of a six-month-old edentulous child who sustained a deep splitting laceration of the oral tongue as a result of being dropped a short distance onto carpeted floor. This unlikely injury pattern is the first reported in the literature and provides information as to a potential mechanism of suspicious, yet unintentional oral injury from a fall.
Case Report
A six-month-old Caucasian male was brought to the Emergency Department in acute distress with significant active oral hemorrhage. He was tachycardic with otherwise stable vital signs and was awake, alert, and crying loudly. A 3 cm Y-shaped full-thickness laceration of the anterior oral tongue was identified (Figure 1). Additionally, a tear of the maxillary labial frenulum was noted, as well as mild ecchymoses of the upper and lower lips. During the initial workup, a skeletal survey and head CT were obtained which did not reveal any additional injuries. Given the patient’s age and injury pattern, a full non-accidental trauma work-up was completed and did not reveal any occult injuries. Hemostasis of the tongue was achieved with gauze compression. The patient was stabilized and then taken to the operating room for general anesthesia and orotracheal intubation followed by surgical repair. Full-thickness tongue laceration identified in the infant.
In the operating room, the tongue laceration was irrigated, and then closed with deep 4-0 braided absorbable suture and superficial 5-0 chromic suture in a simple interrupted fashion. The patient was extubated without issue, and then observed for 36 hours after surgery to monitor oral intake and pain. The patient made a full recovery and there were no complications.
Due to concern for the possibility of non-accidental trauma, the Child Protection Team and the inpatient social workers were notified. Upon speaking with the parents, they reported that they were not present during the incident. It was reported to them that a daycare worker fell with the infant while attempting to pick up another child and that the infant subsequently started bleeding from the mouth.
During the investigation, law enforcement obtained video surveillance footage from the daycare on the day of the incident (Figure 2 + Video Attachment). The surveillance footage shows a daycare worker holding the index infant in her left arm and attempting to pick up another child in her right. While attempting to stand, she loses her footing, causing her to fall forward and to the left, pitching the index infant forward onto the industrial carpet. The infant was then picked up and noted to be crying and bleeding from the mouth. The force of being thrown forward and downward, in addition to the friction by the industrial carpet, caused the tongue to rip and tear in such a way that it resembled being cut with a sharp object. The video footage provided an explanatory mechanism for how he sustained his injuries, thus ruling out physical abuse in this case. The patient’s parents signed informed consent allowing for this case to be reported. Progression from surveillance video depicting the incident. Caregiver, seen holding the patient (infant in blue, left arm of caregiver), attempts to pick up a second child in their right arm. They lose their balance, and the infant is pitched down, sliding across the carpeted floor.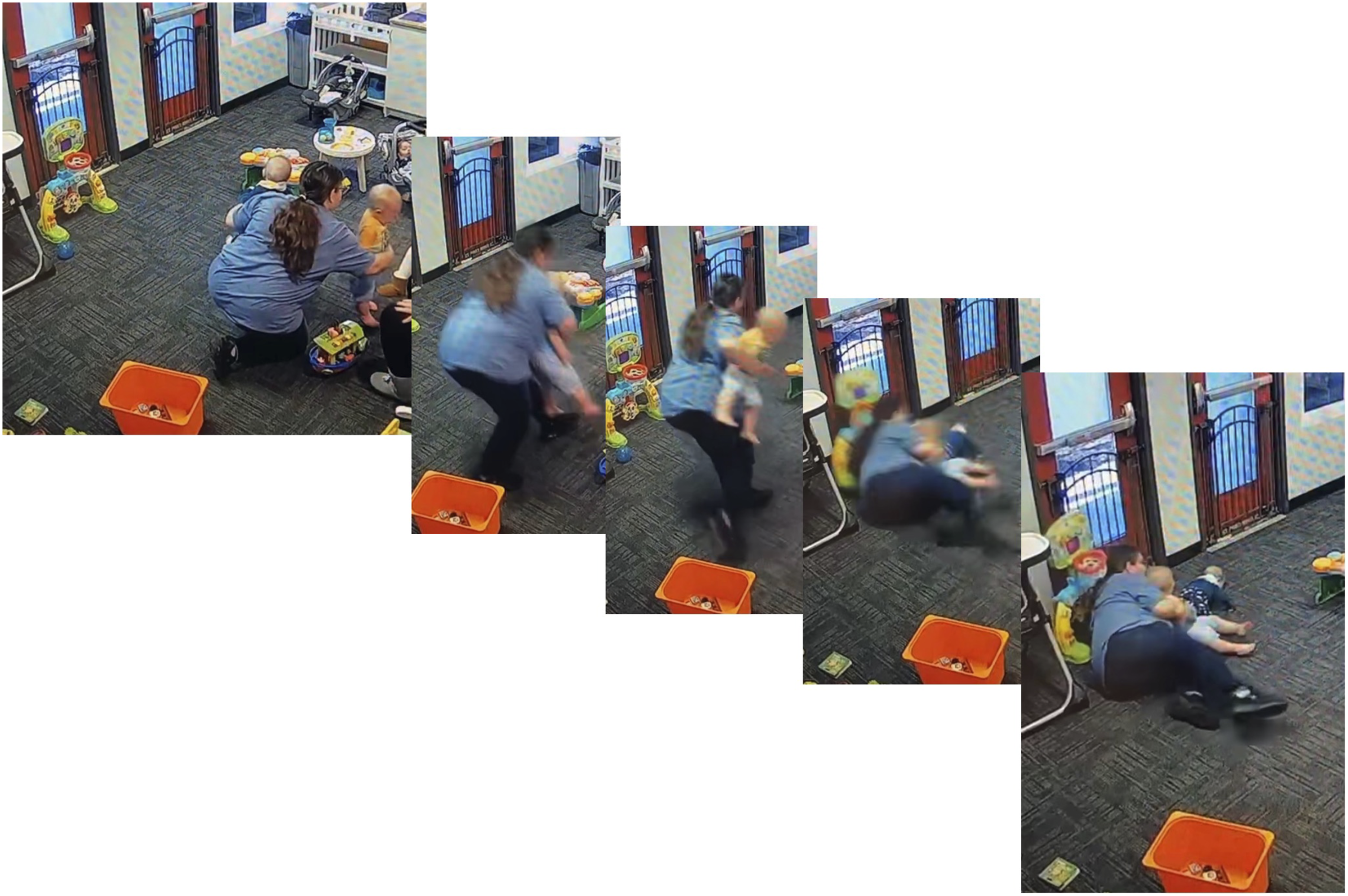
Discussion
In the acute setting, an infant with a tongue laceration requires emergent evaluation and stabilization. Uncontrolled oral bleeding may be life-threatening to an infant, either from aspiration, asphyxiation, or exsanguination from an uncontrolled arterial source. Assessment includes complete physical exam with vitals and comprehensive evaluation for concurrent trauma, along with a focused intraoral exam. Because an oral exam may be challenging on an awake and distressed infant, notifying the anesthesia and operating room teams may be necessary to prepare for exam under anesthesia.
Primary repair of a tongue laceration is a controversial topic. Intraoral injuries typically heal well under secondary intention with few complications, and introducing a foreign body such as sutures into the mouth of an infant can be potentially harmful. Previous studies of pediatric tongue laceration have suggested that the injuries requiring primary surgical repair are larger than 2cm, feature gaping wound edges, through-and-through lacerations, large flaps, active hemorrhage, or involve the anterior tip of the tongue. 2 If operative repair is performed, the wound should be washed with sterile saline, and then closed with buried absorbable braided suture with large bites to prevent tearing of the intrinsic muscles of the tongue. A superficial layer may be closed with an interrupted or running layer of absorbable suture, either additional 4-0 braided absorbable suture, or a 4-0 or 5-0 chromic gut. Parents should be cautioned that these sutures may come out after several days, and if loose, they should be removed to prevent swallowing hazard. Complications of surgical repair include scarring, granulation, wound dehiscence, and rarely, issues with articulation such as lisping. Rates of complications between cases with and without operative repair were similar. 2
Postoperative care includes a pureed or soft diet for 7 to 10 days and pain control with non-narcotic medication. Special attention should be paid to food, breast milk, or formula intake, as the child may be reluctant to eat due to pain, resulting in dehydration or malnutrition. If the child is refusing feeding, a low threshold should exist for hospital admission for supplemental fluids and nutrition.
In the absence of a plausible accidental trauma history, a tongue laceration and oromaxillofacial trauma in an edentulous infant raises significant concern for inflicted injury, thus warranting further medical assessment.3,4 Reported abusive mechanisms for intraoral injuries include forcing a bottle or pacifier into the mouth when a caregiver is frustrated by feeding problems or excessive crying, intentional gagging, or causing a direct blow to the face with an object or hand. 5 Intraoral injuries have also been described in the literature to represent “sentinel” injuries, precluding worse and sometimes fatal abuse.6,7 Though intraoral injuries are uncommon in non-mobile infants, it is important for medical providers to distinguish between accidental and abusive mechanisms of injury. Medical providers should obtain a thorough history and medical evaluation of children presenting with intraoral injuries. Timing, history of the event surrounding the incident, mechanism of injury, and the child’s developmental capabilities should be evaluated for consistency with the characteristics of the injuries seen on physical exam and the child’s presenting symptomatology. 8 Providers seeing patients with facial trauma should have a very low threshold to consult social work, and to notify child protective services as appropriate.
To our knowledge, this is the first described case of a full-thickness tongue laceration found in an edentulous infant after a fall onto carpeted ground. Prior research on intraoral injuries in infants has overwhelmingly demonstrated the need for medical providers to have a high index of suspicion for physical abuse when intraoral injuries are identified with minimal or no history provided by caregivers. In cases of suspected abuse, social work and child protective services should be contacted. However, in certain specific instances, unusual and even improbable accidental injuries can occur.
Supplemental Material
Footnotes
Author’s Note
Presented September 2022, American Academy of Otolaryngology-Head & Neck Surgery Society, Philadelphia, PA, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval is not applicable for this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Informed Consent
Written informed consent was obtained from the patient’s parents for their child’s anonymized information to be published in this article.
Supplemental Material
Video 1. Surveillance Video of the Incident
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.