
Abstract
Objective
To report two patients with iatrogenic, epidermoid implantation cysts associated with the standard retroauricular (Wilde’s) incision, to establish their etiology, to explore means to prevent them, and to ensure that this experience adds to the learning curve of the surgical training of the residents.
Methods
Case series with the review of literature.
Results
One of the two patients, who had an unremarkable follow-up period after cortical mastoidectomy and cartilage tympanoplasty performed three years back, presented with a retroauricular cystic swelling visible since two months. It was hyperintense on T2-weighted magnetic resonance imaging. A sequestered cystic mass was encountered at surgery in the subcutaneous plane in association with the retroauricular scar tissue from previous surgery. In the other patient, two similar cysts (one of them sequestered) were incidental findings at revision tympanomastoid surgery. Histopathology in both instances was consistent with epidermoid cyst. Given their subcuticular location and intimate association with a pre-existing surgical scar, they were considered to be of implantation in origin. This was a potential outcome of persistent inversion of one or both skin edges following simple interrupted suturing. The reason could be a faulty surgical technique, due to improper placement of the needle with respect to skin, inadequate or uneven tissue bite, a tight knot, or failure to manually evert the apposing edges at the point(s) of suspicion.
Conclusions
Sequestered epidermoid implantation cysts due to persistent inversion of sutured skin edges are unusual complications. The illustrations in this case series emphasize the need to adhere to the basic principles of surgical practice. They provide a caveat to the resident surgeons and the faculties who supervise them, that inadvertent and apparently innocuous misses, even at the elementary steps of surgery (like suturing), could lead to complications that are unwanted and potentially avoidable.
Introduction
Epidermoid cysts are monogerminal (ectodermal) encapsulated keratin-containing subepidermal lesions lined by squamous epithelium. 1,2 They are the simplest of the “dermoid” family—a heterogeneous group of lesions that are classified based on the composition and maturity of the epidermal, mesodermal, and endodermal derivatives. 3,4 The term dermoid cyst is often interchangeably used with epidermoid cyst, although a true dermoid arises in areas of embryonic fusion or following sequestration of ectodermal tissue, may be congenital and pre-pubertal, and typically consists of mesodermal component as well (like the adipose tissue and skin appendages). 2,3,5 -7 In the head–neck region, they are often encountered in both superficial and deeper tissue planes and usually arise in areas of craniofacial osseous junctions (e.g., around the orbit and pinna) and soft tissue areas of embryonic fusion (e.g., floor of the mouth). 2,5,6,8 They have the property of bone molding or scalloping, and occasional bone erosion with intracranial extension. 5 However, unlike the bi-/trigerminal lesions described in the “dermoid” family, and keeping aside some rare instances of syndromic disorders (Gardner syndrome, Gorlin syndrome, and Favre-Racouchot syndrome), the essentially monogerminal (ectodermal) epidermoid cysts arise sporadic or de novo in the post-pubertal life and rarely turn malignant. 1,3,9 Of interest, neurosurgical literature studies describe epidermoid cysts along the neuraxis (e.g., the cerebellopontine angle and spinal cord) as trapped ectodermal cell rests during neural tube closure in the embryonic period that may present clinically in both children and adults. 10,11 Therefore, these two entities which are distinct histologically and in germ cell composition might share similar embryologic origin pattern and clinical features and are close differentials.
An epidermoid implantation cyst, however, is a distinct, well-defined entity, similar in composition to the classic epidermoid cyst, but significantly differs in origin. They occur following localized penetrating trauma which may be trivial (needle prick, stapler injury, etc.,) that implant or seed epidermal components within the depth of the dermis or beyond. 9 They are commonly noted in the “working surfaces” of the body that are prone to trauma, like the palms, fingers, and feet. 9,12
Unlike the classic epidermoid cysts that are relatively common in the head–neck region (1.6–6.9%), epidermoid implantation cysts are seldom encountered here. 2,8 Iatrogenic causes that may be inadvertent and unavoidable might be of importance in this region, for example, an epidermoid implantation cyst as long-term complication of tracheostomy wound closure following decannulation. 2
However, such events might not be necessarily unavoidable, as described in the following clinical record of two patients who were diagnosed with epidermoid implantation cysts associated with the retroauricular (Wilde’s) incision as a part of prior otologic procedures.
A clinically evident retroauricular swelling that arises years after tympanomastoid surgery raises the suspicion of recurrence of the primary disease in one of its various forms across the spectrum of chronic otitis media (COM), namely, cholesteatoma recrudescence, granulations with retention cyst, cholesterol granuloma, etc. A relatively long and uneventful follow-up with a dry ear and acceptable hearing gain reduces the chances of such complications and narrows the window of differentials for such a retroauricular swelling. An epidermoid cyst of implantation nature, nevertheless, is least suspected, especially in a sequestered form with a healthy overlying scar. It is also unexpected to encounter multiple cysts as an incidental finding during a planned revision tympanomastoid surgery. Circumstantial evidence from the clinical and surgical perspectives could suggest these epidermoid implantation cysts as iatrogenic, resulting from one or more miss(es) in the basic surgical steps. Such complications are unusual but necessarily avoidable. This clinical record introspects on the possible etiology of epidermoid implantation cysts associated with a scar (in this case, that of the retroauricular incision), the factor of human error, and the necessary steps to prevent them.
Case Report
Patient 1
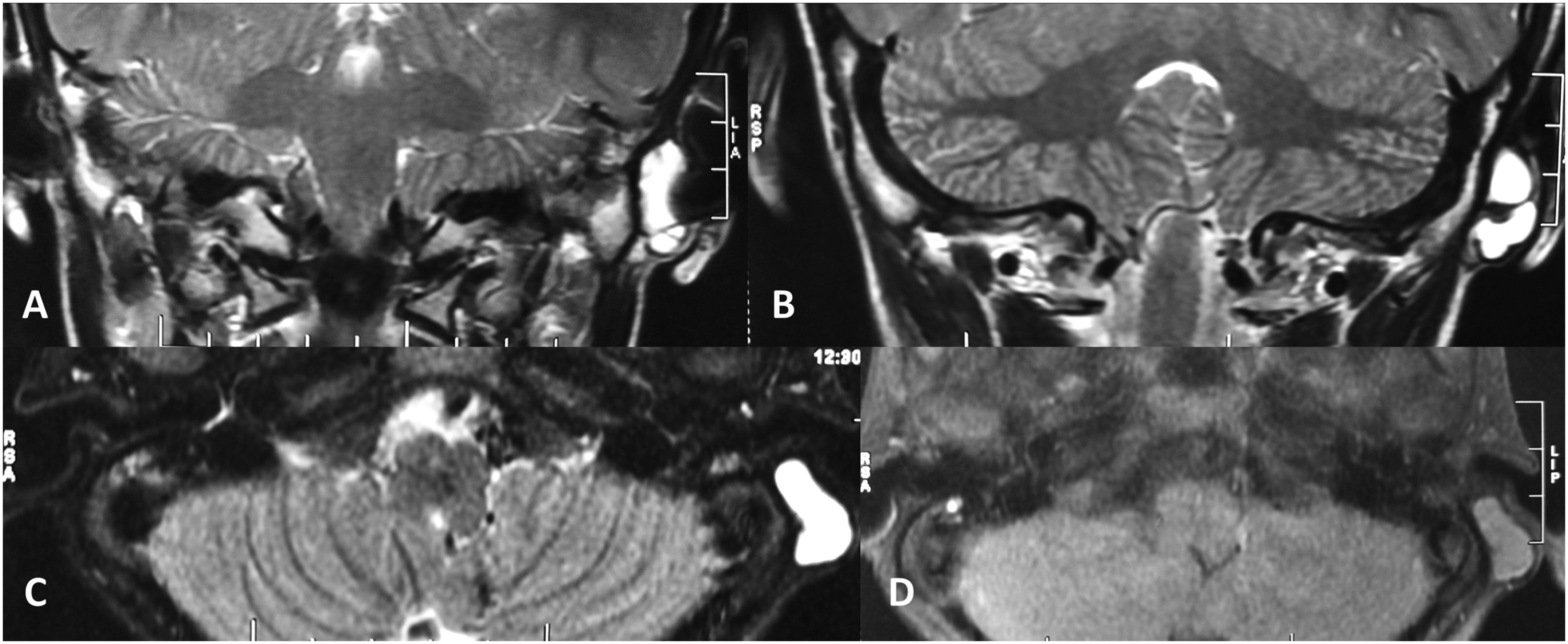
A 15-year-old boy presented with a gradually progressive, painless, left-sided retroauricular swelling that he noticed two months earlier (Figure 1). Three years ago, he underwent cortical mastoidectomy and cartilage tympanoplasty in the same ear for COM with a central perforation and was currently under follow-up. The surgery was performed through the standard retroauricular (Wilde’s) incision under an operating microscope. During the follow-up period, the ear had been persistently dry with intact neograft, and the hearing improved over time to the boy’s satisfaction. The retroauricular swelling with which he now presented was immediately underneath the surgical scar. He denied any accidental or inadvertent trauma in that region during the course of follow-up. The swelling was non-tender, firm, doughy, and immobile and was not adherent to the overlying scar tissue. A non-contrast magnetic resonance imaging (MRI) of the temporal bones showed a well-marginated, loculated lesion superficial to the soft tissue of the left mastoid process, separate from the de-roofed mastoid cavity (Figure 2). The lesion was hyperintense on T2-weighted and relatively isointense on T1-weighted protocol. Given the nature of the primary ear disease and the encouraging post-operative clinical and functional outcome, a recurrence in the form of cholesteatoma pearls or granulations seemed highly unlikely. However, the possibility of cholesterol granuloma could not be ruled out from the current MRI findings because persistent Eustachian tube dysfunction—the primary reason for cholesterol granuloma—is intrinsic to the pathophysiology of COM. A formal exploration of the left tympanomastoid region was planned. This 15-year-old boy presented with left-sided retroauricular swelling. Note the healthy scar over the swelling—reminiscent of a previous surgical procedure performed three years back. Non-contrast MRI of the temporal bones showed a well-defined, septate lesion over the soft tissue of the left mastoid process, isolated from the mastoid cavity, that was hyperintense on T2-weighted (A and B, coronal; C, axial) and relatively isointense on T1-weighted (D, axial) protocol.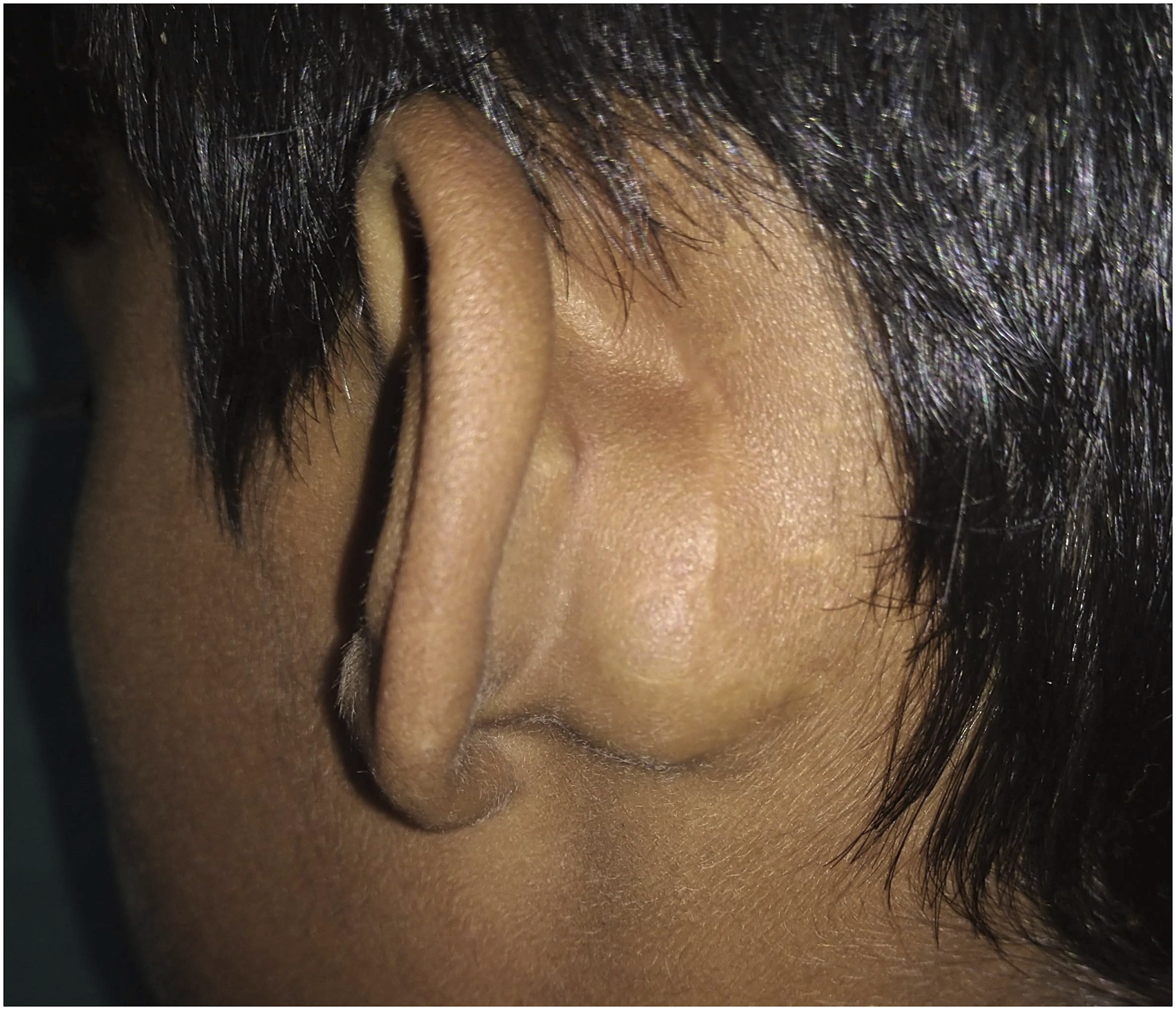
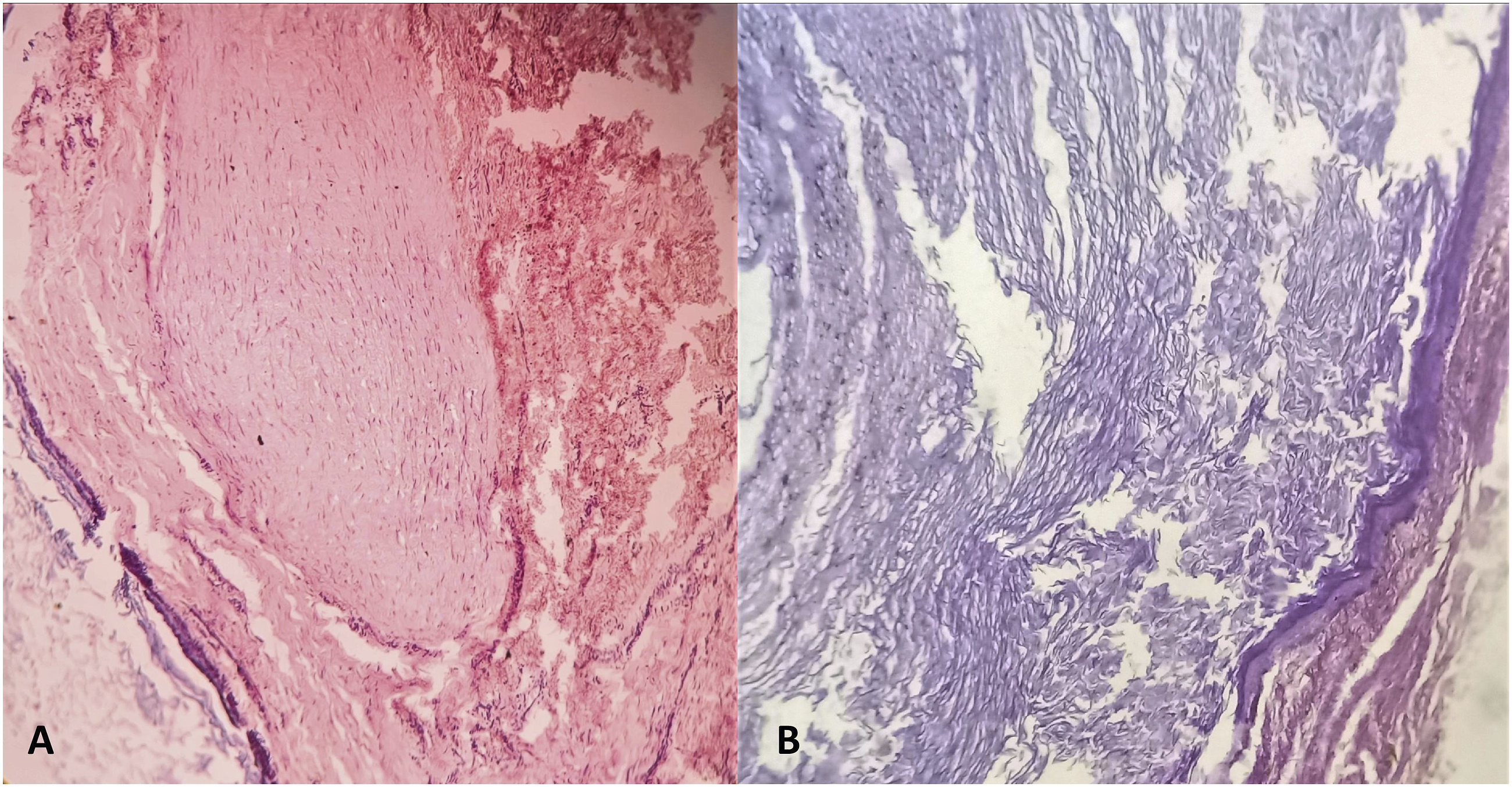
At surgery, a single tense cystic lesion was exposed following a curvilinear incision made just posterior to the existing surgical scar (Figure 3). The lesion was immediately underneath the scar but is separate from it and superficial to the soft tissue over the mastoid process. The cyst, approximately 2.7 cm × 2 cm, was removed intact. When incised, it revealed dirty-white, creamy content. The diagnosis of an epidermoid cyst was made clinically. On histopathology, areas of keratin filaments arranged in whorls forming a cyst could be noted surrounded by fibrous tissue and stratified squamous epithelium, confirming the diagnosis (Figure 4). During surgical exploration, a tense cystic globular lesion could be seen immediately beneath the pre-existing scar but is separate from it, that is, sequestered (A). It was positioned over the mastoid process but lateral to its soft-tissue covering (B). Note the pre-existing scar tissue (A, B); the incision during the present surgery was made just posterior to it. The cystic lesion (C) was partially cut open to reveal its dirty white, creamy content (D). Histopathology revealed confined areas of keratin filaments arranged in whorls, either densely packed within a cyst (A; hematoxylin-eosin, ×100) or loosely arranged (B; hematoxylin-eosin, ×400), surrounded by fibrous tissue and stratified squamous epithelium. Figure subpart A is from the young boy who presented with the retroauricular swelling following a previous otologic procedure, and figure subpart B is from another patient in whom the epidermoid implantation cysts were incidentally discovered during a planned revision tympanomastoid surgery.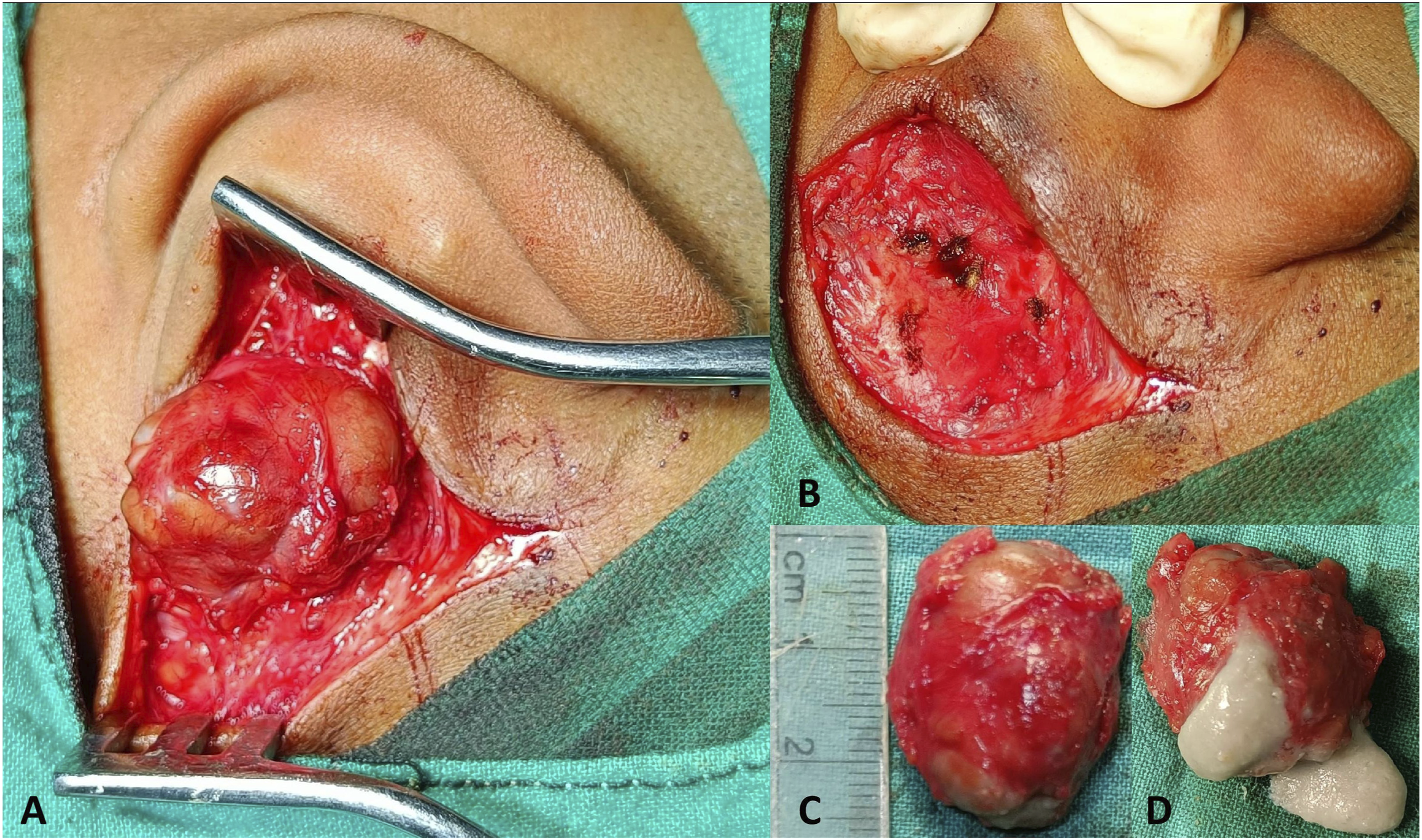
Patient 2
Similar findings were encountered in another patient who underwent revision tympanomastoid surgery due to cholesteatoma recrudescence. The previous surgery (a modified radical mastoidectomy performed through the retroauricular incision) was performed a decade ago in the same institute. During the follow-up, the retroauricular region and the scar it bore were unremarkable. However, in this patient, two separate epidermoid cysts were incidentally discovered at revision surgery beneath the previous surgical scar, one separate from it and the other adherent to the overlying fibrous tissue (Figure 5). Both were free from the underlying soft tissue and were completely excised. Histopathological features were identical to those of the first patient, confirming the diagnosis as multiple epidermoid implantation cysts (Figure 4). Two epidermoid implantation cysts (A, B) were incidentally encountered following a left-sided retroauricular incision in another patient during a planned revision tympanomastoid surgery. One of them was sequestered (A), and the other was adherent to the overlying fibrous tissue (B). Inset: one of the epidermoid cysts punctured to show the characteristic content. Note the pre-existing scar just anterior to the present incision (A, B).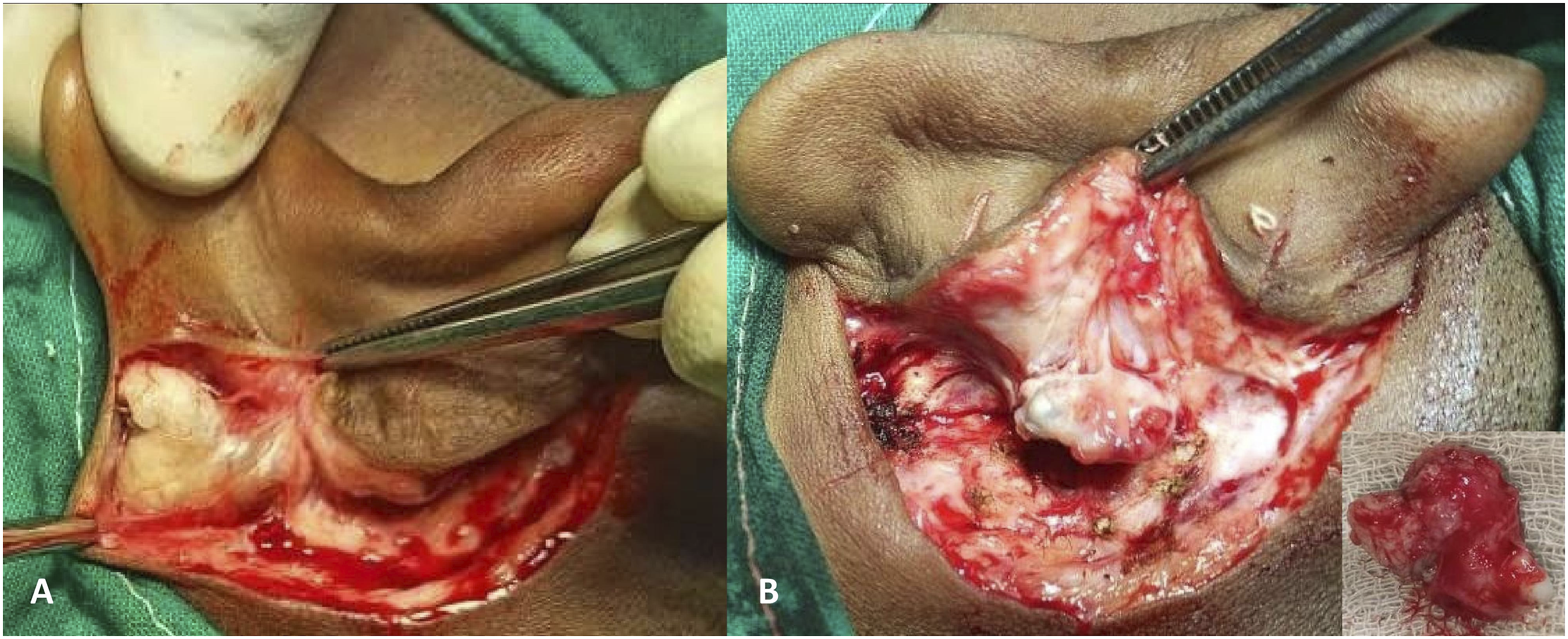
Discussion
The above two illustrations demonstrate sequestered epidermoid cysts in relation to the retroauricular scar from previous ear surgeries that are strongly suggestive of implantation in nature. The lesions could be differentiated from cholesteatoma pearls clinically, by studying the natural course of COM (in the first patient; COM mucosal variety, with uneventful follow-up), the protracted course of the disease (in both patients), and the inert nature of the keratinous lesions; and at surgery, when the cysts were found strictly in the subcutaneous plane in close association with the overlying surgical scar. Histologically, however, the two entities shared identical features, except that the epidermoid implantation cysts lacked the perimatrix components that characterize a cholesteatoma. 13
Such epidermoid implantation cysts associated with a surgical scar might be ubiquitous and would find relevance to all surgical disciplines. For such events in the head–neck region associated with a known surgical incision, it is imperative for the concerned otolaryngologists to explore the etiology and the means to prevent them.
An introspection into the above-mentioned clinical events led the authors focus their attention on some basic faults in suturing technique during wound closure. The skin was closed with simple interrupted sutures using 3-0 monofilament following the standard practice in otologic surgery. 14 Somehow, the needle placement (entry and exit) with respect to the skin surface was not correct, the tissue bite was of inappropriate depth and thickness, the skin edges were kept under tension (rather than being gently apposed) due to over-tightened knots, or, following completion of the suture, the edges were not made to evert manually at the point(s) of suspicion. The last possibility follows the practice guidelines from the authors’ institution (evidence level 5). 15 Any of them could lead to persistent inversion of the apposing skin edges. Inappropriately apposed edges are known to result in contracted and sunken scar, overriding or stepping, and hypertrophied scar tissue secondary to vertical shearing of the apposing surfaces. 16 However, it is indeed unusual to have epidermoid implantation cysts as long-term complications of persistently inverted edges despite having an otherwise neat and cosmetically acceptable scar, as seen in the patients in the present series.
The fact that two of the three cysts were sequestered, that is, separate from the overlying scar, was intriguing. Continued growth of squamous epithelium of the inverted epidermal edges led to the formation of implantation cysts, but the prolonged duration of the process might have caused healing of the epidermal surfaces resulting in an apparently healthy-looking scar and an independent, sequestered existence of the cysts in the subepidermal plane. The one which was adhered to the overlying fibrous tissue (in the second patient) could likely be in this process of sequestration.
Regardless the outcome of persistent wound inversion, this was a call to return to the basics of the surgical skills.
The tertiary-care teaching institute where the authors are affiliated trains residents in otolaryngology and head–neck surgery. They receive basic surgical training during their undergraduate tenure and specialty training in otolaryngology during their post-graduate residency period. As an integral part of this training, and also because the department needs to cater to a huge influx of patients at any given time, the residents are regularly called upon to assist the faculties in various surgeries. During this period, they are often allowed to perform certain surgical steps under active guidance. At a certain period of time in their training, after they have gained a favorable evaluation of their learning curve, they are allowed to perform the key steps independently under supervision. However, elementary steps like wound closure and dressing are often performed by them on their own because the supervising surgeon gets busy with his/her next surgery assignment. There is also the assumption that the residents, who are uniformly well-versed in the general surgical principles since their undergraduate training days, can finish the remaining steps. Nevertheless, an inadvertent and unintentional omission of a basic step, often an element of human error, might lead to potentially avoidable complications.
Accepting the vicarious responsibility and in order to address the gap in training, the faculty members called upon the resident surgeon group to discuss the complications encountered in the two patients described above. There, the residents were advised to remain equally vigilant throughout the duration of surgery, enduring the psychomotor fatigue that tends to set in toward the end. Also, no surgical step is to be ignored or discriminated as “major” or “minor.” It was reemphasized that the outcome of an intervention depends, apart from many other factors, on every step of the surgery done with full alertness, thereby minimizing the factor of human error. In other words, it is the entirety of the surgical procedure, not only the “key” steps, that tests the attitude and temperament of the surgeon.
In this context, the tenets of proper suturing technique (simple interrupted suture), especially those that would prevent inversion of the apposing skin edges, were revised (Figure 6).
16,17
The senior author group prefers vertical mattress sutures to close a retroauricular incision (evidence level 5).
15
At the cost of a relatively prominent scar, this ensures hemostasis especially where the incision encroaches the scalp and also prevents inadvertent inversion of the edges. However, for uncomplicated tympanomastoid surgeries, a simple interrupted suture is often practiced, with subcuticular and running locked sutures being better but less frequently followed alternatives. Due to variations in individual preference, the principles of common suturing techniques must be mastered and practiced with patience so that scar-related complications can be avoided. Tenets of the discussion with the resident group that focused on revising the techniques to prevent inversion of the apposing skin edges during simple interrupted suture are presented here. The hand-drawn schematic diagrams have been provided by the first author. While interpreting the figure subparts and their legends, the readers are advised to note the trajectory of the suture material within the skin and subcutaneous tissue, and the relative position of the skin edges. Point 5 of the discussion follows authors’/institutional practice (level 5 evidence; reference 15).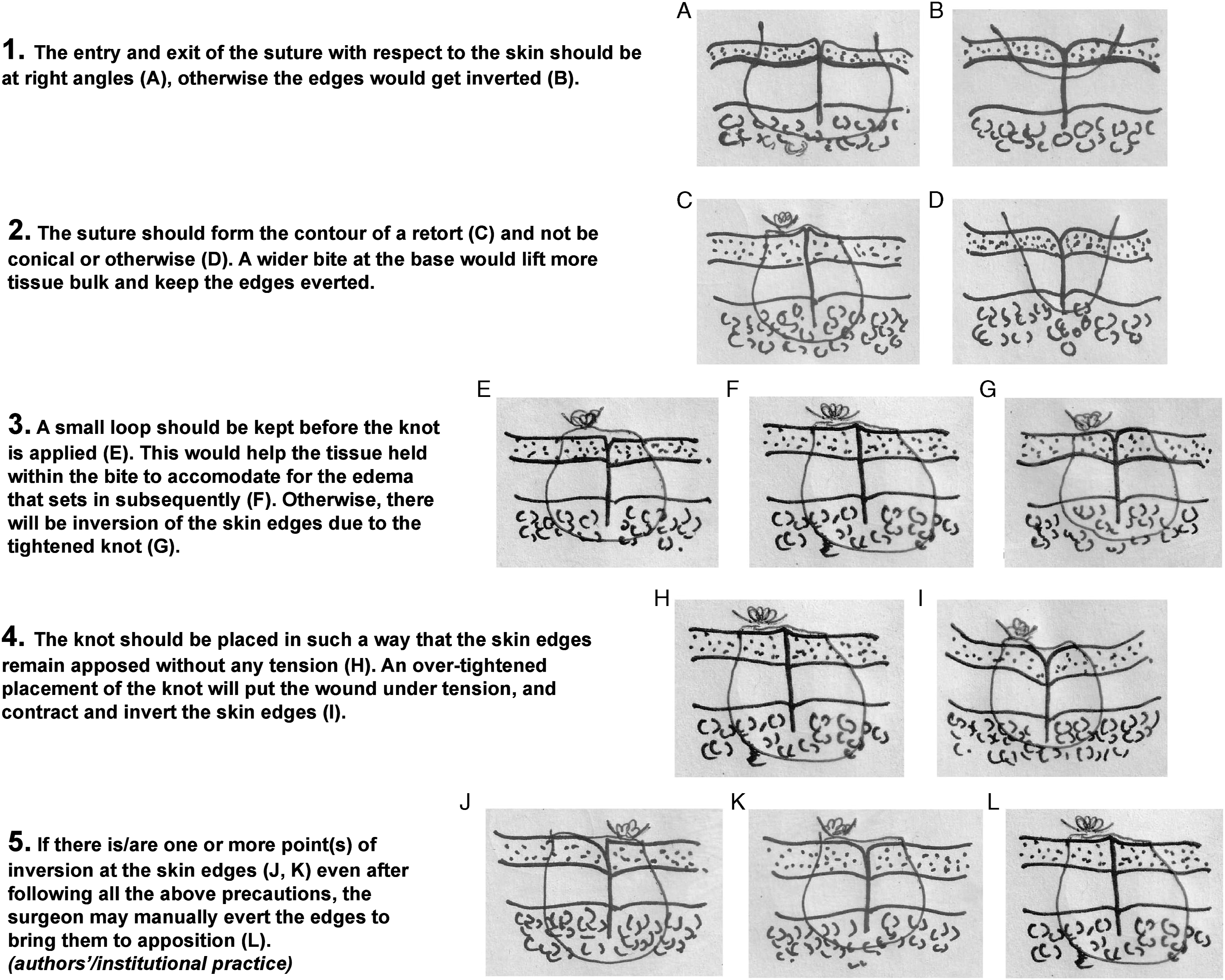
Conclusions
The apposing skin edges following a simple interrupted suture should not get inverted and appropriate techniques should be adopted during suturing to ensure this. It demands full attention of the resident surgeon, lest he/she overlooks the basics. Improper apposition of the edges produces several scar-related complications. However, sequestered epidermoid implantation cysts associated with a healthy scar are unusual sequelae of wound inversion. This unexpected but avoidable outcome provided a valuable learning experience for the resident surgeons, who realized the importance of adhering to the fundamentals of surgical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The clinical data pertaining to the patients are available with the authors and can be reproduced on request.
Ethical Statement
Written informed consent has been obtained from the patients for the publication of this case series. The clinical and surgical principles adopted for the management of the patients complied with the ethical standards of the relevant national and institutional guidelines on human experimentation, as laid down in the Declaration of Helsinki, 1975, as revised in 2013, at Fortaleza, Brazil.