
Abstract
Epidermoid cysts are generally benign lesions surrounded by squamous epithelium with cystic contents. The lining of the cysts produce keratin, which resemble a cheese-like material. They typically occur in the skin and mucous membranes and are congenital in origin; iatrogenic epidermoid cysts are rare. Epidermoid cysts are usually painless and asymptomatic, and their diagnosis is based on histological examination. This paper aims to present the case report of a 23-year-old patient with an iatrogenic epidermoid cyst that occurred following tracheostomy. The importance of preoperative radiological imaging in the diagnosis of epidermoid cysts is also highlighted.
Introduction
Epidermoid cysts are painless, slow-growing, benign tumors caused by the subcutaneous proliferation of sebaceous glands or epidermal cells. 1 Epidermoid cysts may be congenital or acquired. 2 However, iatrogenic epidermoid cysts are uncommon and very rarely reported to occur after tracheostomy. We report a case of an epidermoid cyst on the trachea found during revision tracheostomy in a 23-year-old patient, along with a review of previous literature. Ethical approval for this case report was obtained from the institutional review board of Pusan National University Yangsan Hospital (IRB No: 05-2021-064).
Case Report
A 23-year-old male patient was admitted to a hospital due to traumatic subdural and subarachnoid hemorrhage in September 2013. He underwent a percutaneous tracheostomy in November 2013. In December 2015, a revision tracheostomy was performed by an otolaryngologist under general anesthesia. The operative procedure, as performed, is described. A horizontal skin incision was made over the previous incision. The strap muscles were dissected and retracted laterally. A transverse cut was made between the third and fourth tracheal rings. The skin and cut ends of the trachea were approximated using interrupted 4-0 vicryl sutures; four stitches were placed at the 5, 6, 7, and 12 o’clock positions. Subsequently, a silicone, single-cannula tracheostomy tube of 7-mm diameter was inserted into the tracheal window from the previous tracheostomy.
A stomaplasty was later performed at the same hospital in May 2017. A skin incision was made around the stoma site and subcutaneous tissue, dissected. The skin and subcutaneous tissue were then closed with 4-0 vicryl sutures using Gambee’s technique.
During the rehabilitation phase of his treatment, he was admitted to our hospital with acute kidney injury (AKI) and pneumonia. Since the patient needed continuous mechanical ventilation, he was referred to our otolaryngology department in October 2020 for a second revision tracheostomy.
During the procedure, a vertical incision of approximately 2 cm was made over the previous incision site. After the scar tissue from the previous surgery was removed, a firm, mass-like lesion was found (Figure 1A). While dissecting out the mass, we observed that it was connected to the trachea at the previous tracheostomy site. The mass was approximately 1.5 × 2.0 cm in size, and a whitish, cheese-like material was seen inside it on cross-sectioning (Figure 1B). Prior to the surgery, the patient could not undergo contrast-enhanced computed tomography (CT) due to AKI and pneumonia; therefore, only non–contrast-enhanced chest CT images had been obtained. After the operation, a review of the non–contrast-enhanced chest CT revealed the presence of a hypodense, mass-like lesion anterior to the trachea (Figures 1C and 1D). The pathologic examination after surgery confirmed the diagnosis of an epidermoid cyst. (A) Intra-operative view of the cystic mass at previous tracheostomy site. (B) Excised specimen. (C and D): Non–contrast-enhanced chest computed tomography images, axial (C) and coronal (D), hypodense mass anterior to the trachea.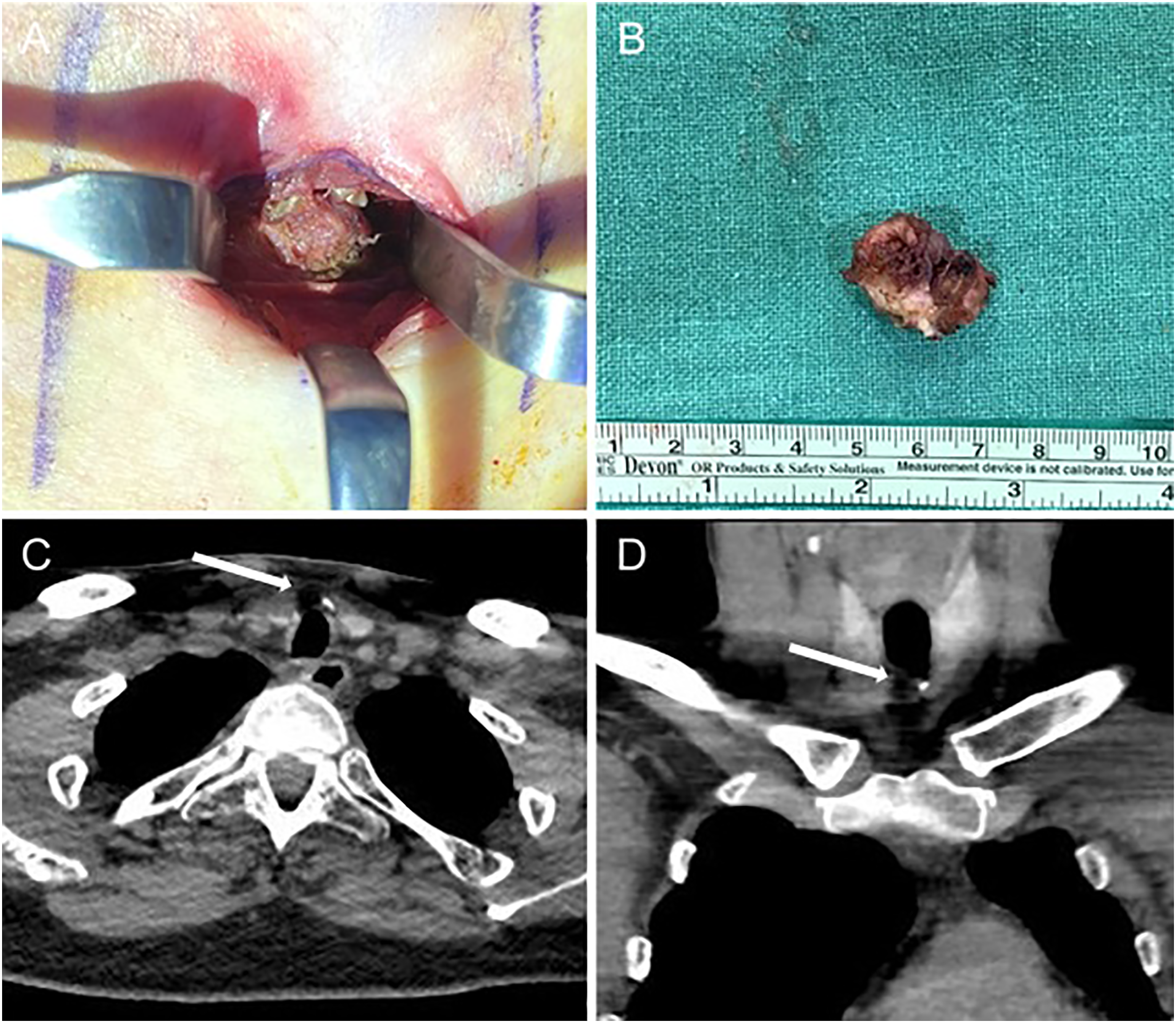
Discussion
The treatment of an epidermoid cyst is complete resection of the mass. The procedure involves application of a transverse incision on the skin over the cyst, dissection from the surrounding tissues, and removal without damaging the cyst wall. Recurrences can occur in case of incomplete resection. In this patient, we tried to reduce the possibility of recurrence by performing a complete resection of the tissue around the trachea connected to the mass. 3
As mentioned earlier, epidermoid cysts are often congenital, whereas iatrogenic cysts are rare. Rkhami et al reported a case of an iatrogenic epidermoid cyst in the cauda equina following lumbar disc herniation surgery. A 69-year-old woman was admitted to the hospital with complaints of lower-back pain, dysuria, and weakness in the lower extremities for 2 years. She had undergone spinal surgery 30 years prior due to L3–L4 lumbar disc herniation. Magnetic resonance imaging revealed intradural cystic lesions. Her symptoms improved after surgery, and the biopsy confirmed the diagnosis. 4
Rarely, iatrogenic epidermoid cysts have also been reported in the field of otolaryngology. Thompson et al reported the case of a 30-year-old man who presented with a left parotid mass and a history of undergoing tympanoplasty via an endaural incision using temporalis fascia, approximately 3.5 years ago. The mass was then excised through superficial parotidectomy; the histological examination confirmed a diagnosis of epidermoid cyst. 5
In both of the above-mentioned cases, the iatrogenic epidermoid cysts are thought to have occurred due to the invagination of epithelial cells after surgery.
There are two methods of tracheostomy: percutaneous and open surgical tracheostomy. There have been many reports comparing the perioperative and postoperative complications involving both these methods. Klotz et al 6 reported that there was no significant difference in the incidence of complications between percutaneous and open surgical methods in a systematic review. In our patient, tracheostomy had been performed twice in addition to stomaplasty, which had been performed once. The first tracheostomy was performed using the percutaneous method. Thus, the possibility of epithelial invagination due to skin puncture needs to be considered. The other possible hypothesis is that epithelial cells could have been implanted into the subcutaneous tissue during the first revision tracheostomy. Stomaplasty could also have resulted in the invagination of epithelial cells into the subcutaneous tissue. Any of the above occurrences could have led to the formation of an epidermoid cyst anterior to the trachea. During our literature search, we could not find any reports of epidermoid cysts that occurred in close proximity to the trachea or following a tracheostomy or stomaplasty.
To conclude, we have reported a case of an epidermoid cyst that occurred at the tracheostomy site following tracheostomy. Surgeons should exercise caution during tracheostomy or stomaplasty so as to not facilitate epithelial cell invagination into the subcutaneous tissue. In addition, this case suggests the significance of obtaining radiological images prior to revision tracheostomy in order to rule out the presence of lesions such as epidermoid cysts around the trachea.
Footnotes
Author Contributions
Eui-Suk Sung: design Min-Sik Kim: conduct Minhyung Lee and Jin-Choon Lee: analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.