
Abstract
True thymic hyperplasia results from stressful situations such as chemotherapy. It commonly presents as an anterior mediastinal mass; cervical location is exceptional. Here we report a case of a cervical true thymic hyperplasia in a 12-year-old girl who had a Hodgkin lymphoma treated by radiotherapy and chemotherapy. She was referred to our department for a left cervical mass. The PET scan showed a hypermetabolic adenopathy. Mediastinal MRI was unremarkable. The patient underwent resection of the cervical mass under general anesthesia. Pathological examination confirmed the diagnosis of a true thymic hyperplasia. The aim of this paper is to illustrate a case of an incidental ectopic cervical thymic hyperplasia in a patient treated for Hodgkin lymphoma.
Introduction
True thymic hyperplasia after chemotherapy is a well-documented phenomenon in children. 1 Few cases of cervical ectopic thymus due to disruption of thymus embryogenesis or during thymus descent have been reported. 2 The presence of a cervical lesion in treated lymphoma habitually points to recurrence or dissemination of the disease.
The aim of this paper is to illustrate a case of an incidental ectopic cervical thymic hyperplasia in a patient treated for Hodgkin lymphoma.
Case report
A 12-year-old girl was treated for Hodgkin lymphoma group TG3 stage IIIB (according to Ann Arbor staging system). The patient received antitumor treatment based on radiotherapy and chemotherapy. She was in remission for one year. The patient was referred to our department for a left cervical mass, which was discovered incidentally (Positron emission tomography scan (PET scan)) during follow-up.
On physical examination, no palpable cervical swelling was detected.
Cervical ultrasound revealed multiple bilateral oval cervical nodes, sub-centimetric and without signs of atypia. PET scan showed tracer uptake in the left supraclavicular region: lymph node recurrence of Hodgkin lymphoma was suspected. Contrast enhanced CT (computed tomography) scan showed a 13 × 18 mm oval nodule located laterally to the left jugular vein: malignant adenopathy was suspected (Figure 1). Mediastinal MRI (magnetic resonance imaging) revealed no abnormal findings. Cervical CT scan in axial section showing a 13 × 18 mm oval nodule located laterally to the left vascular axis.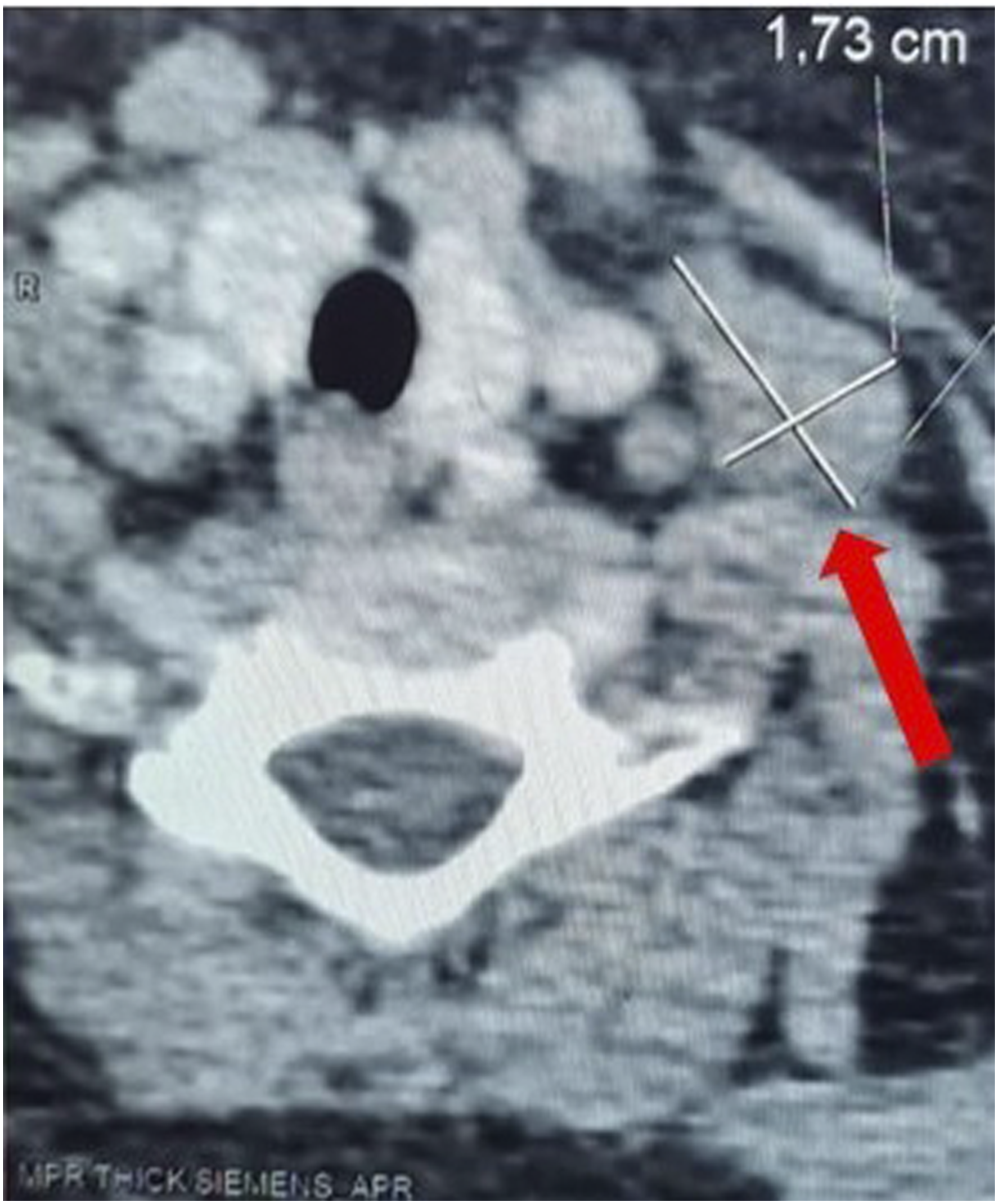
The patient underwent removal of the cervical mass under general anesthesia. Intraoperatively, the mass was adhered to the common carotid artery.
Histological examination showed regular hyperplastic thymic tissue, with preserved architecture. No sign of malignancy was found. Thymic tissue was multinodular in appearance, separated by fibrous septa (Figure 2). An ectopic parathyroid tissue was also identified (Figure 2). (A) Hyperplastic multinodular thymic parenchyma, separated by fibroadipal septa (HE x 50); (B) Thymic parenchyma with Hassall’s corpuscles (blue star) (HE x 200); (C) Ectopic parathyroid tissue within the thymic parenchyma (green star) (HE x 50).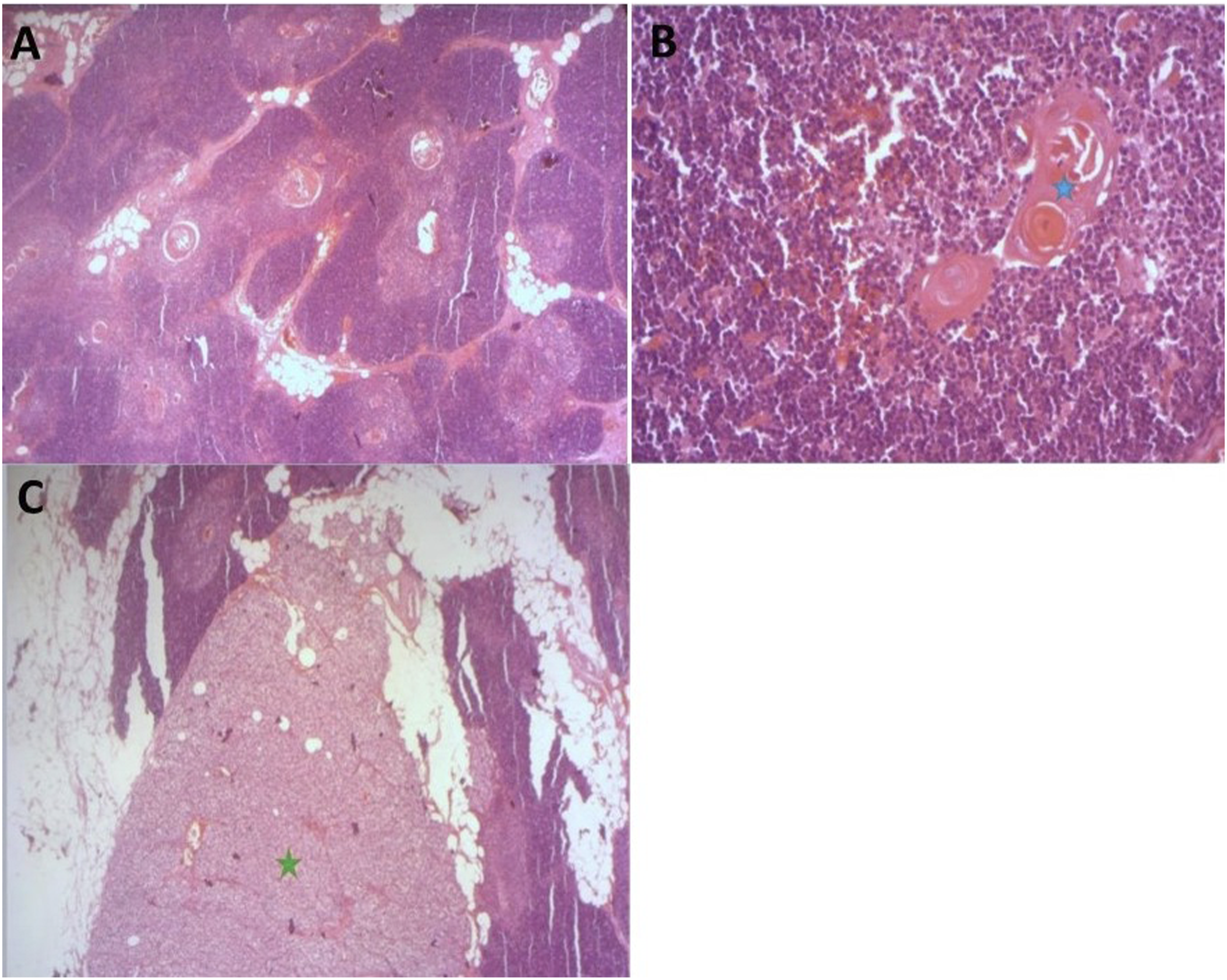
After one year of follow-up, the patient exhibited no evidence of recurrence.
Discussion
The thymus derives from the ventral pouch of the third and fourth branchial arch. It appears during the sixth week of gestation and starts to grow and migrate in a caudal and medial direction. During the eighth week of fetal life, a fusion of both thymic lobes at the median line causes the thymus to take its final position in the anterior-superior mediastinum. 1 The thymus tends to increase in size during childhood reaching its greatest volume at puberty, before eventual involution. 1
Ectopic cervical thymus results from disruption of thymus embryogenesis or incomplete migration of the thymus. It can be found anywhere along the course of the embryonic thymopharyngeal ducts from the angle of the mandible to the anterior mediastinum. 1 Studies found that most ectopic cervical lesions occur in the central neck either intrathyroidal or extrathyroidal. 2
Cervical thymic ectopias commonly remain asymptomatic, therefore rarely detected clinically in children. 3 It was thought to be a very rare condition (under 1%). Nevertheless, some studies have found that up to 50% of children who underwent neck imaging, had lesions demonstrating radiographic features of ectopic cervical thymus. 1
Ectopic cervical thymus can present as a mass that is solid cystic or mixed, with solid thymic tissue, as in our observation being less frequent. 2
Hyperplasia of the thymus are divided into two groups, true hyperplasia in which there is both increase in size and in weight of the gland with retention of normal microscopic appearances, and lymphoid hyperplasia in which the presence of lymphoid cells with germinal centers prevails without taking into account the size or the weight of the thymus. 4 The present case falls into the first category.
Stressful biological conditions, such us chemotherapy, can induce acute involution of the thymus with reduction of thymic volume. This phenomenon is well known in patients with various types of malignancy who were undergoing chemotherapy, and it was followed by thymic rebound hypertrophy after cessation of chemotherapy. 5 It is a common occurrence, found in up to 90% of children and adolescents with malignant lymphoma after treatment. 6 This is indicative of an immunological rebound phenomenon and seems to be a favorable sign for the control of the malignant disease and a positive prognostic factor. 7
Thymic rebound is defined as enlargement of thymic tissue by more than 50% of its size prior to initiation of treatment. 1 It can occur in both orthotopic and ectopic thymus. 8 Its onset varies from 2 months after the initiation of treatment to as late as 15 months after completing treatment. 1
Predictive factors for reactive true thymic hyperplasia found in the literature are young age, absence of thymic infiltration by lymphoma at baseline, and absence of radiotherapy to the thymus site. 7
True thymic hyperplasia of ectopic tissue in the cervical region after chemotherapy for Hodgkin's lymphoma raises the problem of differential diagnosis with persistent or new lesions, mainly malignant ones, or benign lymph nodes hyperplasia frequently observed. 6
Our patient showed incidental left cervical swelling on follow-up CT scan after completion of chemo and radiotherapy for Hodgkin lymphoma. Initially, a relapse was suspected. However, the final diagnosis was true thymic hyperplasia from an ectopic thymus located in the cervical region.
It is very difficult to distinguish benign thymic rebound hyperplasia from other disease processes. The use of advanced imaging techniques has been of help to clarify the diagnosis in adults due to the large fatty component of the thymus. However, in pediatric population thymus is composed of soft tissue. This implies that neither cross-sectional imaging, nor scintigraphy, nor PET scans are able to differentiate with certainty between neoplastic tissue and thymic hyperplasia. 6
In cases when the diagnosis is unclear, whether there is concern for malignancy or in the setting of compressive symptoms, biopsy and/or complete excision should be considered. 2
Some authors suggest CT scan follow-up every 3 to 6 months after histological confirmation of thymic hyperplasia. 9
Conclusion
Residual ectopic tissue may persist during its migration to its final position in the anterior mediastinum. True thymic hyperplasia may result from chemotherapy for lymphoma in the pediatric population. However, its presence in the cervical region is exceptional. Histological examination is necessary for diagnosis if imaging techniques are unable to rule out malignancy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
The data can be shared.
Informed consent
Informed consent was obtained from the patient for the publication of her information.