
Abstract
Pharyngeal ectopic thymus is a rare cause of pharyngeal masses and is rarely considered in the differential diagnosis of neck and head masses in children. In this paper, the case of an infant with a pharyngeal ectopic thymus is presented and our intraoral surgical approach in the patient’s treatment is described.
Background
The thymus is a specialized primary lymphoid organ of the immune system that contributes to the development of T cells. 1 Ectopic thymic tissue most frequently occurs in the submandibular triangle and lateral neck, accounting for 0.4% of neck masses. 2 Rare cases of oropharyngeal ectopic thymus have been reported in the literature. 3 In this paper, we discuss a case of neonatal apnea due to a pharyngeal mass, which was confirmed to be an ectopic thymus via pathological examination.
Case Report
A 1-day-old female infant presented to our neonatal intensive care unit due to apnea, with an endotracheal tube already inserted by a secondary hospital. The patient had no history of respiratory distress, stridor, or dysphagia in her family. Accordingly, the patient was diagnosed as having respiratory failure, pneumonia, metabolic acidosis, septicemia, and asphyxia by a series of physical and laboratory examinations. Due to respiration recovery, the patient was prepared for extubation after 3 days of treatment with antibiotics, ventilation, and nutritional support. When the endotracheal tube was extracted, a mass was found protruding from the oral cavity. The mass, having an outer length of 4 cm, was soft and had 2 lobes anteriorly (Figure 1), and its base was not clearly observed via laryngoscope. Otolaryngology and stomatology were consulted while the patient was in the lateral position, and the mass was fixed. Fine needle aspiration (FNA) of the mass was not performed. Computed tomography (CT) revealed a solid columnar mass of 6 cm × 1 cm in the oral cavity (Figure 2). The mass had a blurred boundary with the tongue, and its base was located at the level of the oropharynx. Computed tomography was used to locate the mass, for which an excisional biopsy was done. Stomatology was consulted to assist otolaryngology in treating the oropharyngeal mass.

The mass had 2 lobes anteriorly out of the mouth.
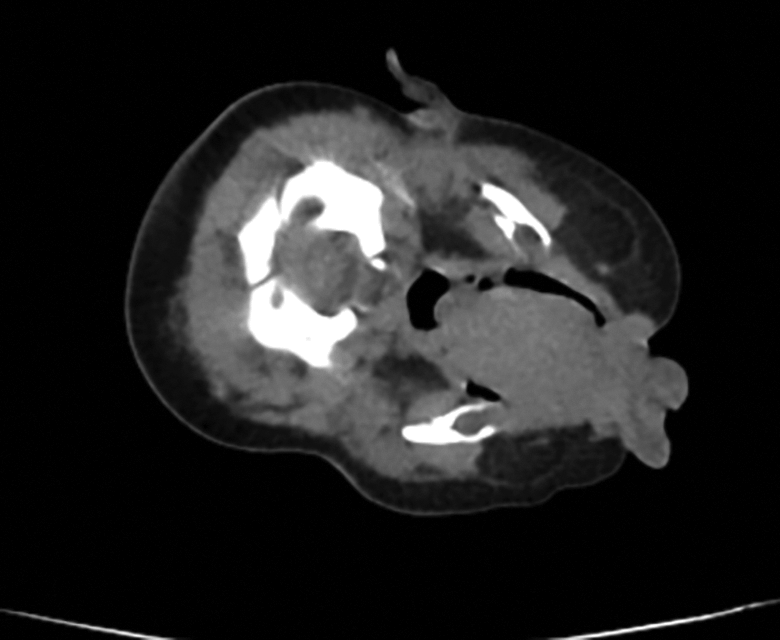
Computed tomography of the pharynx showed a solid, columnar mass in the oral cavity.
Under general anesthesia, a cuff-less endotracheal tube was inserted. A suspended Davis gag was then introduced. The perioperative macroscopic examination showed that the mass was lobulated in the front, the surface of mucosa was smooth, and blood vessels were distributed under the mucosa. The mass was solid, and the puncture was aneroid. The pedicle of the mass was thin and located in the lower part of the right palatopharyngeal arch, and there was no macroscopic lesion around the base. The mass was removed from the ligated base and submitted for histopathological study. The wound was nonhemorrhagic and had no remnants. The patient maintained a positive airway pressure until postoperative day 3, where she was able to take nutrition orally. A postoperative echocardiogram revealed a normal-sized thymus in the appropriate anatomic location. She was discharged home on postoperative day 12 in good condition. Postoperative pathology revealed a solid ectopic thymus (Figure 3).
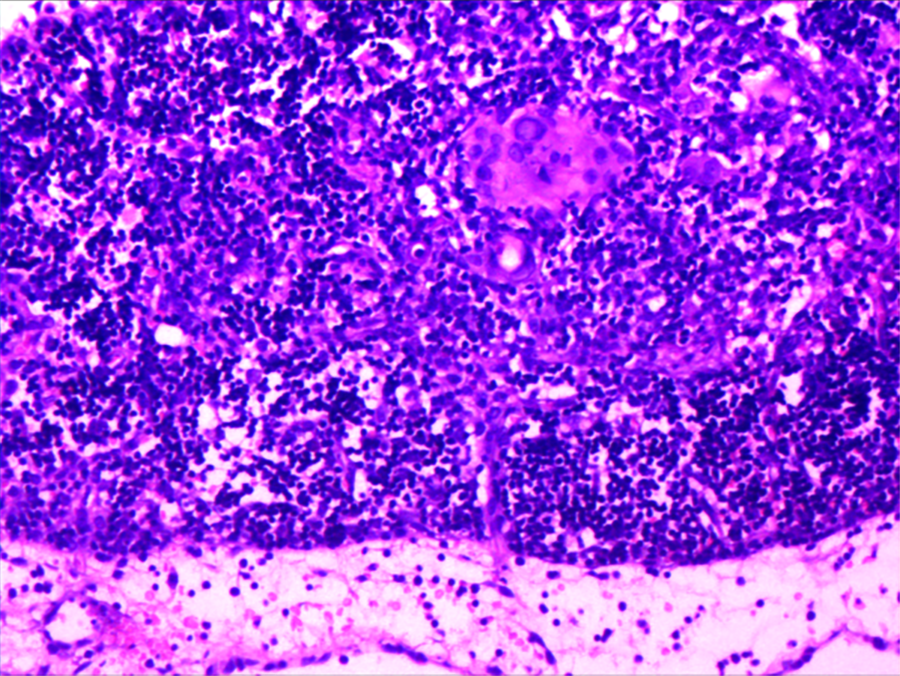
This H&E stain showed the typical characteristics of ectopic thymus tissue (original magnification ×40).
Discussion
The thymus is derived from 2 thymic primordia that arise in the belly of the third and fourth pharyngeal pouches. 4 These paired lobes proliferate in the sixth week of embryonic development and conventionally extend along a path from the pyriform fossa through the thyrohyoid membrane and along the vagus. 5 The 2 lobes fuse to form the thymopharyngeal duct in the midline and then descend from the mandibular angle to the mediastinum. Any defects in thymic embryogenesis may lead to the formation of a congenital ectopic thymus usually in the neck 6 or rarely, as in our case, in the pharyngeal region. Moreover, the development of thymus is intimately connected with that of parathyroid. They are derived from the third and fourth pharyngeal pouches, and a small amount of parathyroid tissue was found adjacent to the wall of thymic cyst. 4 Many studies have reported that the location of ectopic thymus was adjacent to the thyroid gland. 6 However, the 2 units are not presumed as one organ due to their differences in functions.
Ectopic thymus often occurs within the periods between childhood and early adulthood, reciprocal with the normal growth of the thymus gland. 7 It was reported that an ectopic thymus has an average length of 22.5 mm, ranging from 8 to 38 mm. 6 Some researchers ascribe this difference to the different ages among the patients as ectopic thymus is thought to follow the same growth trend. 1,6 Rarely, as in this case, the newborn possesses an ectopic thymus with a length of about 40 mm. Most lesions are located on the left side with a slight male predominance. 7,8 Ectopic thymus has a completely normal microscopic morphology and may be expressed as a mass in the neck or pleural surface. Generally, it is located adjacent to the thyroid gland, 6 near the carotid sheath, 5 in the submandibular region, 7 or rarely in the retropharyngeal region. 3 Most cases are asymptomatic; however, pain, upper respiratory tract infection, pressure, and hoarseness of voice may occur. 7 The remnants may be solid thymic tissue, thymic cysts, or cervical thymoma, with cysts being more common. 9 The solid cervical thymic tissue is caused by its abnormal descent. Cervical thymic cysts result from deterioration of Hassall’s corpuscles or cystic changes within the remnants of the thymopharyngeal duct. 5,10
In this case, the patient presented with an incidental finding of a pharyngeal mass. The differential diagnosis of a newborn with a pharyngeal mass is extensive and may include neuroblastoma, lymphoma, cysts such as bronchogenic or thyroglossal, cystic hygroma, hamartoma, tonsillar lesions, lipoma, dermoid cyst, and ectopic thymus. Most children with suspected pharyngeal space masses should undergo imaging such as CT, ultrasound, or magnetic resonance imaging. Ultrasound is recommended as the most direct and practical modality for preoperative diagnosis. 6 Magnetic resonance imaging is the most accurate noninvasive examination for identification and provides superior soft tissue delineation. 11 However, in this case, as the patient was a critically ill newborn, CT was more easily obtained. Imaging is helpful in demonstrating the cervical anatomy and evaluating the extent of the mass.
Removal of the lesion is the basis of treatment. It is recommended that the presence of a mediastinal thymus should be confirmed by imaging or FNA prior to surgery as an athymic child may suffer from immunological dysfunction. 5,11,12 For asymptomatic patients with ectopic thymus, it is prudent to identify its histopathological nature. The normal thymus in the mediastinum must be examined before surgery, and postoperative follow-up is required. In this case, the patient underwent immediate surgery to ensure her health without verification of a normal thymus. It is unique that a thymic remnant is located in the right palatopharyngeal arch, which has been rarely reported in the literature. 6 After reviewing the imaging, the otolaryngology department considered that the mass could be safely excised through an intraoral approach. Additionally, the postoperative ultrasound demonstrated the normal thymus exists. Histopathology was definitive in the finding of thymic tissue and Hassall’s corpuscles.
Conclusion
Pharyngeal thymic remnant is a rare cause of head and neck masses in the pediatric population. However, it must be considered in the differential diagnosis of head and neck masses, even in the pharyngeal space. An intraoral approach for resection of a pharyngeal mass is an excellent, safe option and is cosmetically acceptable to patients and their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received specific grant from National Natural Science Foundation of China (grant number: 81570926) and Health and Family Planning Commission of Gansu Province (grant number: GSWSKY2018-40).