
Abstract
Kimura’s disease (KD) is a rare chronic inflammatory disorder of unknown etiology. The purpose of this article is to increase the awareness of clinicians regarding KD presenting with intraparotid and neck nodes which can mimic various inflammatory and neoplastic conditions. A 22-year-old man presented with a slow-growing left parotid swelling for 3 years. Ultrasound and computed tomography showed multiple enlarged intraparotid and neck nodes. Fine needle aspiration results showed lymphoid tissue hyperplasia. A diagnosis of KD was based on characteristic histopathological findings after a superficial parotidectomy in conjunction with peripheral eosinophilia. KD should be included in the differential diagnosis especially in young Asian men with slow-growing lesions and peripheral eosinophilia. Cytology by fine needle aspiration is useful to exclude malignancy but the results may be inconclusive. Surgical excision is best for definitive histopathological diagnosis, and has been the mainstay of treatment of KD.
Introduction
Kimura’s disease (KD) is a rare chronic inflammatory angiolymphatic proliferative disorder of unknown etiology. 1 Most cases have been reported in young Asian men presenting with painless masses involving subcutaneous tissue, lymph nodes, or salivary glands primarily in the head and neck region, accompanying with blood eosinophilia and elevated serum immunoglobulin E. 1 The lesions can mimic a malignant tumor or chronic infection.
Parotid gland involvement has been variably reported in 10–58% of KD cases.1,2 Parotid gland swelling in KD results from lesions in the intraparotid lymph nodes or adjacent subcutaneous connective tissues, without involvement of the parotid parenchyma. 1 There have been only 5 reported cases of KD presenting with intraparotid lymph nodes enlargement.3-7 Herein, we report the case of a young man with left parotid swelling from intraparotid node enlargement and regional lymphadenopathy. Unlike previous reports, the diagnosis of KD in this case was difficult in the absence of typical cytological characteristics. A definite diagnosis was established based on histological findings after surgical excision. A review of the literature is provided, and the differential diagnosis is discussed.
Case report
A 22-year-old Thai man presented with left parotid gland swelling which had been slowly increasing for 3 years. There was no history of pain, fever, night sweats, or weight loss. The physical examination showed a non-tender, firm mass measuring 2 × 2 × 4 cm extending from the left angle of the mandible to the postauricular area with normal overlying skin. There was also a palpable node sized 1.5 cm at the leveI II left neck. There was no facial palsy. Fine needle aspiration (FNA) results showed lymphoid tissue hyperplasia of the intraparotid lymph node, without atypical cells. FNA findings of the left neck node also showed reactive lymphoid hyperplasia. The ultrasonographic and computed tomography (CT) findings are shown in Figure 1. Laboratory data included hemoglobin of 16.7 g/dL, platelet count of 293,000/uL, and white cell count of 10,300/uL: differentiation showed 30.9% eosinophils, 37.9% neutrophils, 25.4% lymphocytes, and 4.7% monocytes. Blood urea nitrogen, creatinine, electrolytes, and urinary analysis were normal. A chest radiograph was unremarkable. (A) Gray-scale color doppler ultrasound image showing a group of enlarged hypoechoic nodes with hilar vascularity at the left intraparotid and periparotid areas. (B) Axial contrast-enhanced CT showing multiple homogeneously enhancing left cervical nodes involving the left parotid and periparotid regions. (C) The coronal image shows associated cervical lymphadenopathy, greater on the left than the right.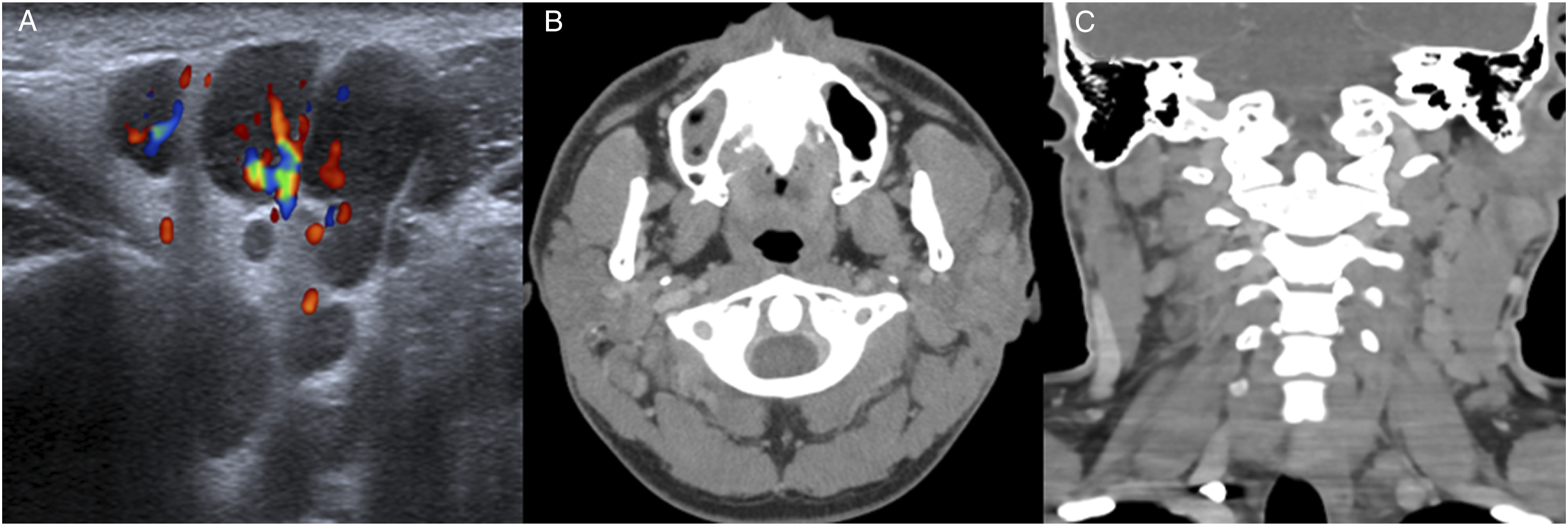
A benign tumor or inflammatory lesion was suspected. Malignant lesions, for example, lymphoma or nodal metastases, although unlikely from the clinical presentation, could not be totally excluded. A lymph node biopsy was suggested, but the patient decided to go directly to surgery due to cosmetic concerns at the parotid area. A left superficial parotidectomy was performed. During the operation, the plane between the subcutaneous tissue and the parotid gland was well-defined. The main trunk of the facial nerve and its branches were identified. The superficial lobe of the parotid gland was dissected and removed. The deep lobe of the parotid gland was not involved. Macroscopically, several gray-white irregular rubbery nodules measuring 0.5–2.0 cm were seen within the parotid gland. A microscopic examination revealed numerous nodal and extranodal reactive lymphoid follicles with germinal centers, dense eosinophil infiltration, eosinophilic microabscesses, stromal fibrosis, and increased vascularity (Figure 2). A diagnosis of KD was then made based on the histopathogical findings in conjunction with the clinical presentation and marked peripheral eosinophilia. The postoperative period was uneventful. At the 6-month follow-up, there was no recurrence. Histological findings showing reactive lymphoid follicles with germinal centers, and prominent eosinophilic infiltration with microabscess formation (H&E stain, 40X).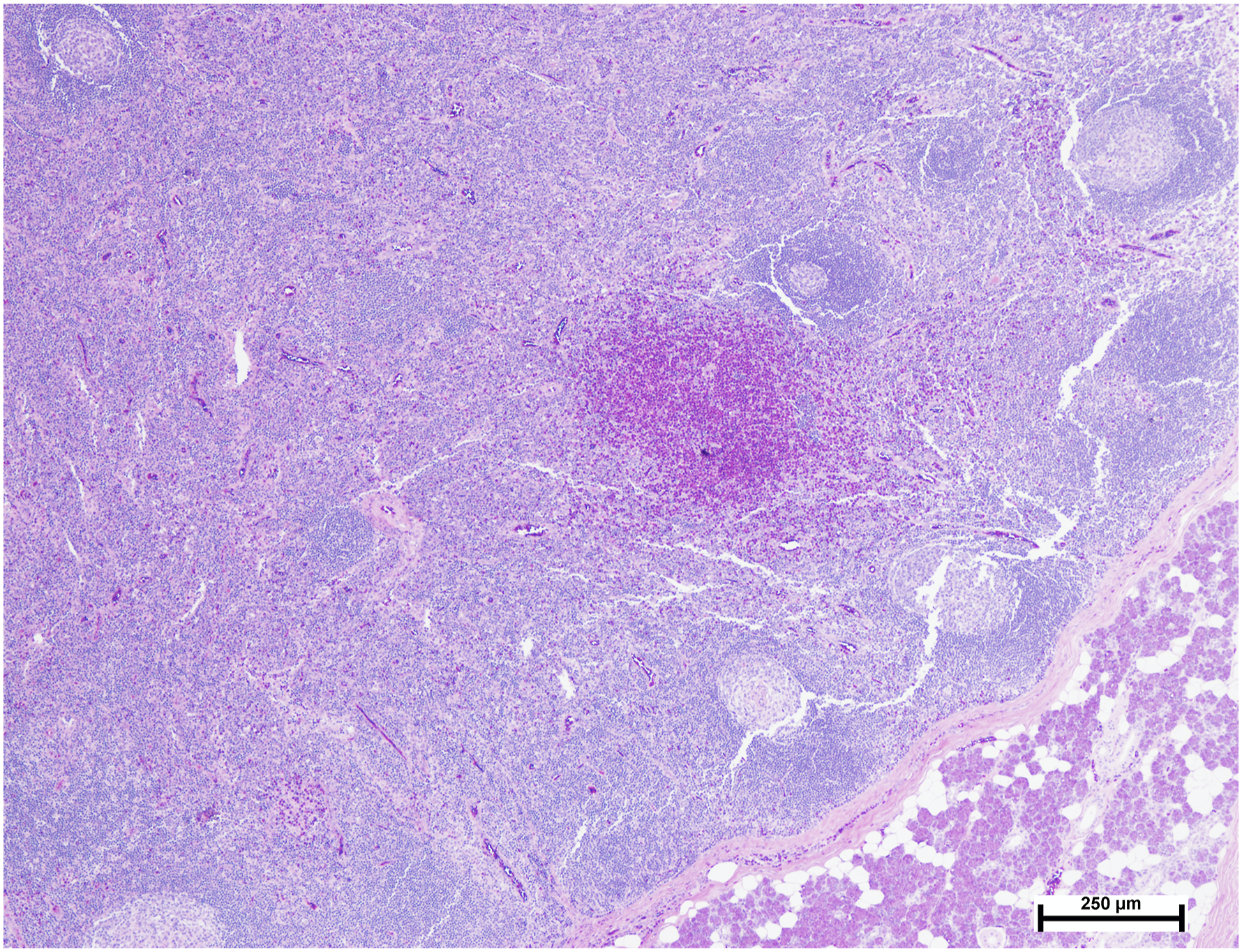
Discussion
Case reports of Kimura’s disease presenting with intraparotid nodes enlargement.
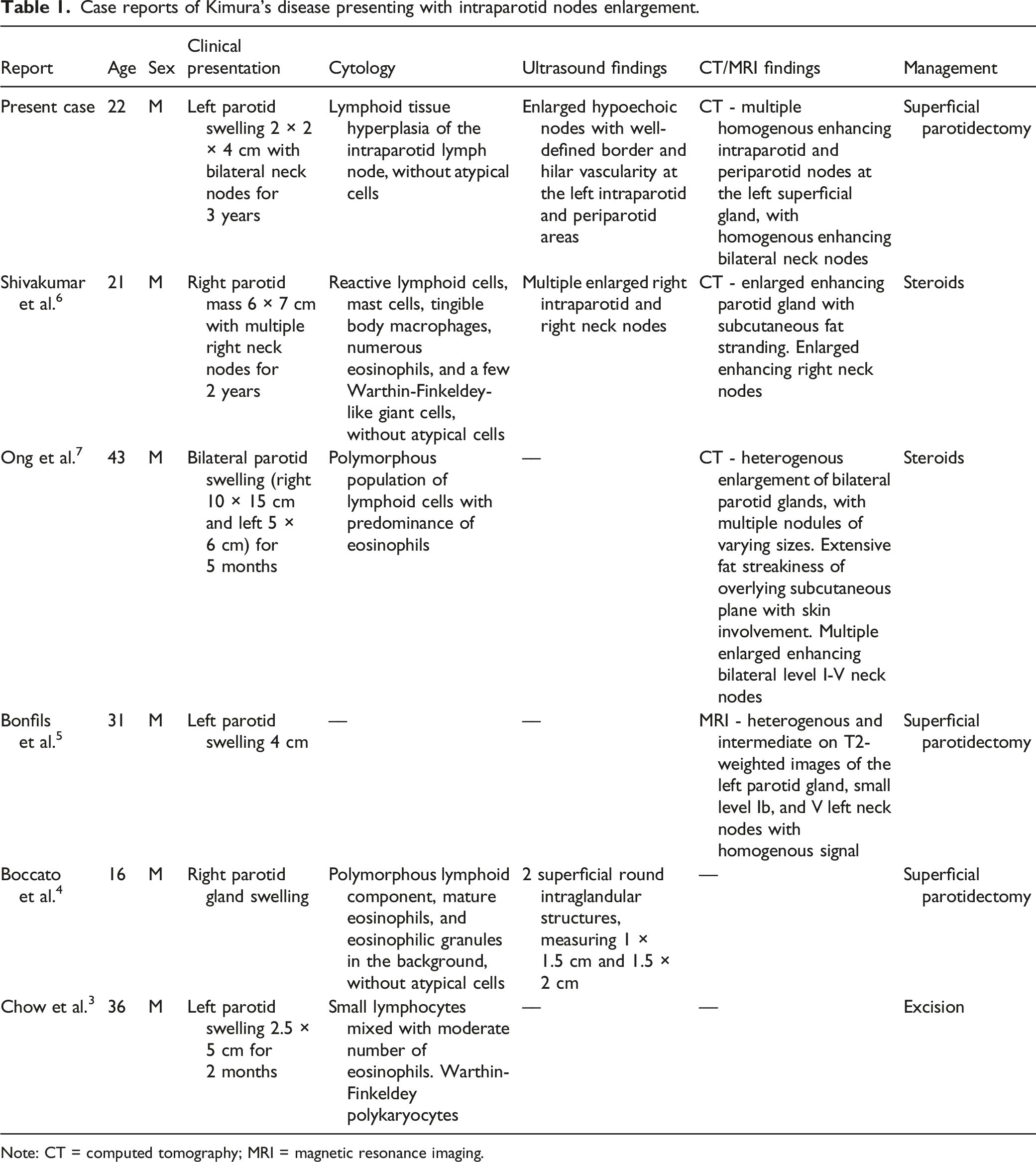
Note: CT = computed tomography; MRI = magnetic resonance imaging.
Differential diagnosis for intraparotid lymph node enlargement with fine needle aspiration results showing lymphoid tissue hyperplasia.
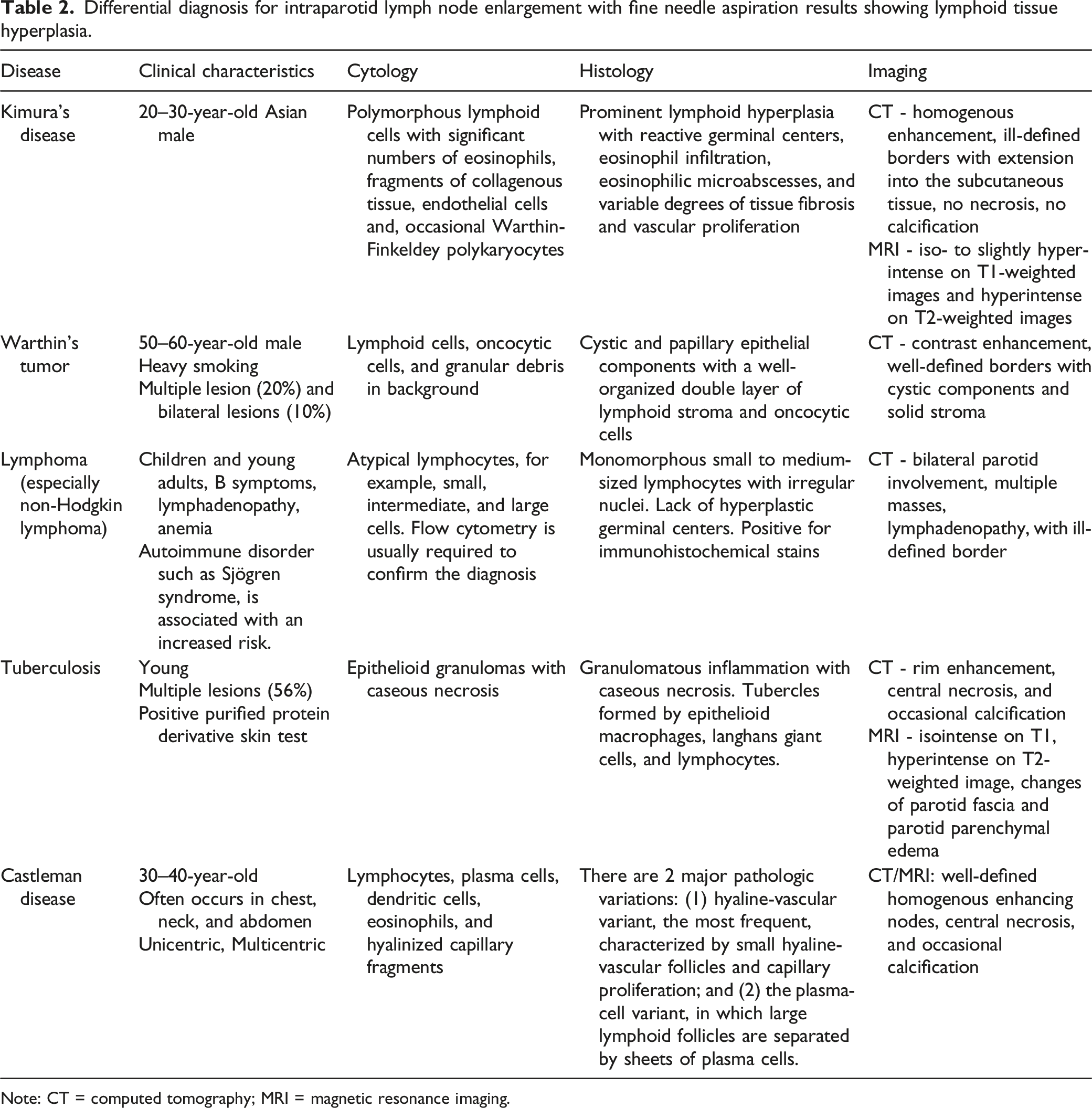
Note: CT = computed tomography; MRI = magnetic resonance imaging.
Conservative treatment with steroids or cyclosporine is an initial option to avoid surgical risks. Surgery is an effective single treatment especially for patients with tumors smaller than 3 cm, and symptom duration shorter than 5 years. 10 However, recurrence rate is as high as 26%, 35%, and 50% after surgery, medication and radiotherapy, respectively. 10 Good practice is based on discussing the advantages and disadvantages of each modality with the patient.
Conclusion
Kimura’s disease is a rare chronic inflammatory disorder of unknown etiology that involves the subcutaneous tissue, lymph nodes, or salivary glands of the head and neck region. The presentation of our case highlights the need for awareness of Kimura’s disease by clinicians and pathologists. A high degree of suspicion leading to early diagnosis is helpful to put the clinicians in a better position for diagnosis and management. Cytology by fine needle aspiration is useful to exclude malignancy but the results may be inconclusive. Surgical excision is best for definitive histopathological diagnosis, and has been the mainstay of treatment of Kimura’s disease.
Footnotes
Acknowledgments
We thank Dr. Suchaya Pajareeyaphan, Songklanagarind Hospital, for preparing pathological results of the patient in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
The study was approved by the Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand (REC.65-392-13-1).
Data availability statements
Requests to access the data should be directed to the corresponding author.