
Abstract
Introduction
Kimura disease is a rare chronic inflammatory disease of unknown cause.1-11 Kimura disease usually presents as an asymptomatic mass on the head and neck1-6,8 and is accompanied by peripheral blood eosinophilia.1-11
Herein, we analyzed the clinical characteristics and treatment results in surgical patients having a final diagnosis of Kimura disease at this hospital over a 16-year period.
Patient Population and Methods
This study received approval from the Institutional Review Board of Chonnam National University Hwasun Hospital. Surgical patients with a final diagnosis of Kimura disease of the head and neck region from January 2007 to December 2022 were enrolled.
Clinical data obtained from enrolled patients were reviewed for gender, age, smoking, alcohol drinking, past medical history, clinical symptoms, duration of symptoms, size of mass and site of Kimura disease, eosinophil granulocyte count, preoperative fine-needle aspiration cytology (FNAC), treatment method, postoperative treatment, follow-up and relapse.
All patients underwent one or more radiological examinations, including computed tomography (CT), magnetic resonance imaging (MRI), and/or ultrasound (US), before surgery to assess the extent of their lesion(s) and to assist with treatment planning. All surgical specimens were confirmed by histopathological examination.
Results
The clinical findings of the 8 patients with Kimura disease are summarized in Table 1. Of the 8 patients with Kimura disease, 6 were male and 2 were female. The mean age of the patients was 36.9 ± 4.9 years (range, 17-52 years). There was 1 smoker and 4 alcohol drinkers. Past medical history showed 2 patients with atopy, 1 patient with nephrotic syndrome, and 1 patient with hypertension, all of whom received treatment for these conditions.
Clinical Demographics of 8 Cases of Kimura Disease.
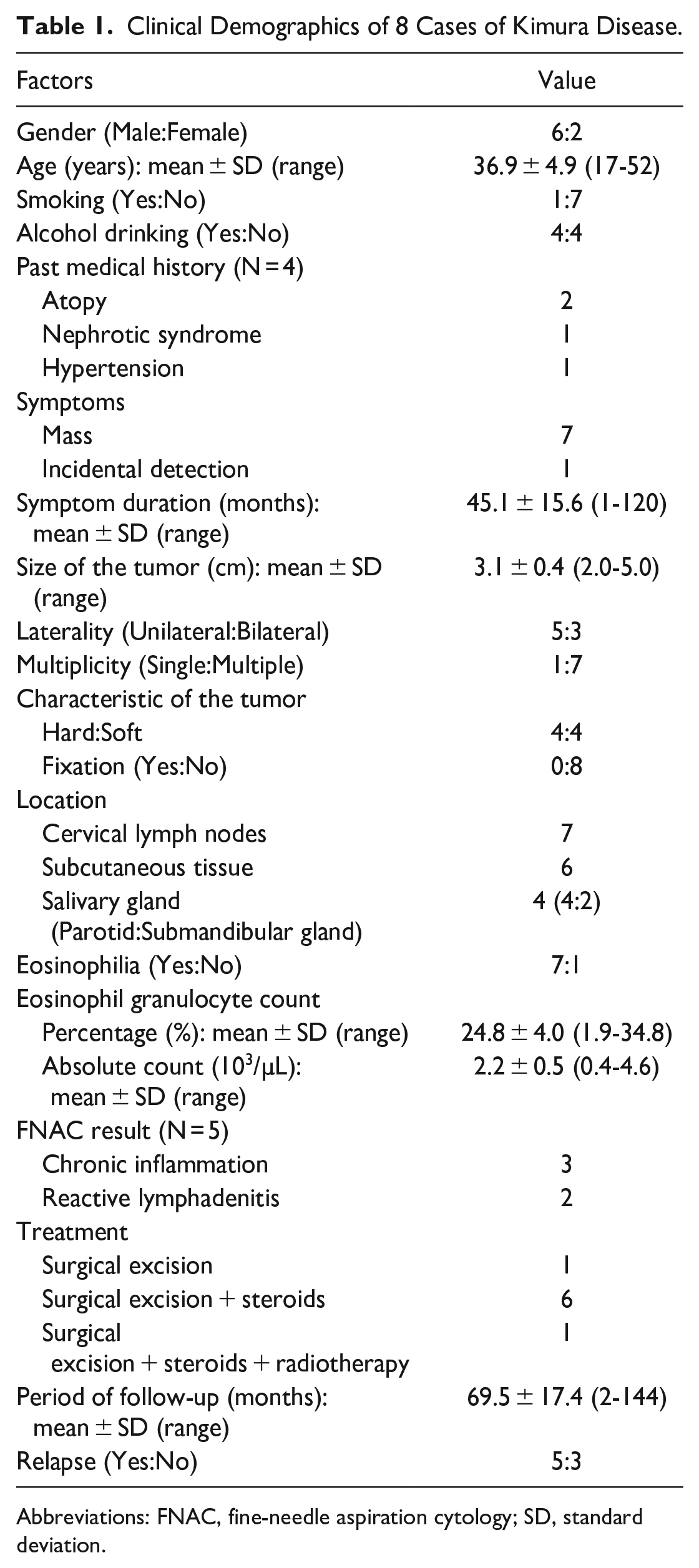
Abbreviations: FNAC, fine-needle aspiration cytology; SD, standard deviation.
The most common symptom was a mass in the head and neck region (n = 7), followed by incidental detection (n = 1). The duration of symptoms was 45.1 ± 15.6 months (range, 1-120 months). The mean tumor size was 3.1 ± 0.4 cm (range, 2.0-5.0 cm). Of the 8 Kimura disease cases in the head and neck region, 5 (62.5%) were unilateral and 3 (37.5%) were bilateral. Seven cases of Kimura disease with multiple lesions occurred, and the remaining patient had a single lesion (Figure 1). The tumors were hard in 4 patients, soft in four, and not fixed to surrounding structures in any of them. The most common location of Kimura disease in the head and neck was the cervical lymph nodes in 7 patients, subcutaneous tissue in 6 patients, and salivary gland in 4 patients.
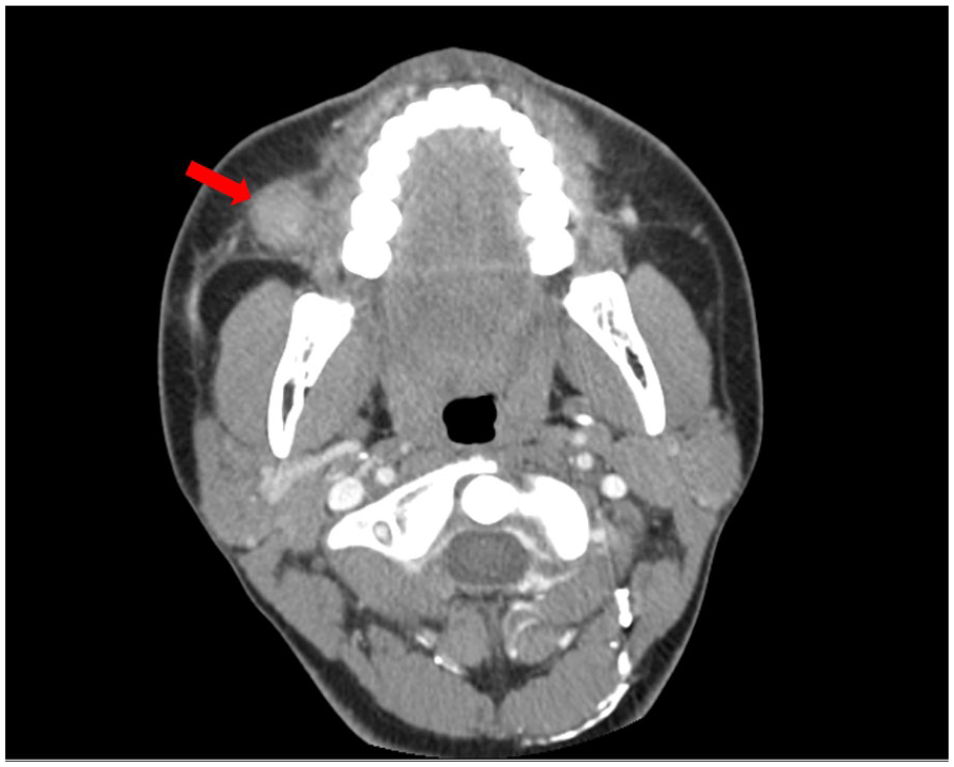
Axial computed tomography scan of a 17-year-old male patient with Kimura disease illustrates a single lesion (red arrow) in the right buccal space. The patient underwent surgery only, and there was no relapse.
Eosinophilia was present in 7 patients (87.5%). Preoperative FNAC was performed in 5 patients (62.5%). Based on the FNAC results, 3 patients were diagnosed with chronic inflammation and 2 were established with reactive lymphadenitis.
All patients underwent surgical resection and were identified with Kimura disease based on the final specimen biopsy. No major complications arose after surgery. Six patients received steroids after surgery, and 1 patient underwent radiotherapy as a side effect of steroid treatment (Figure 2).
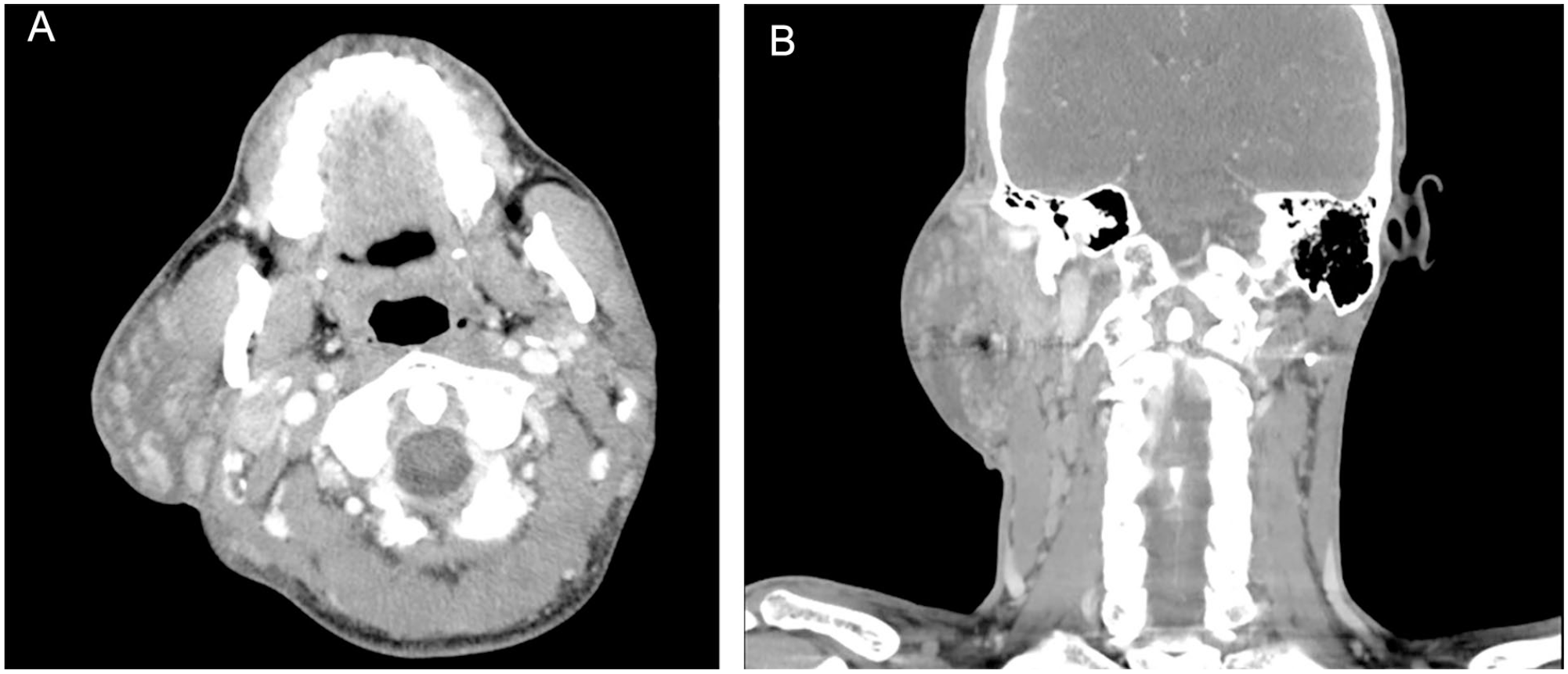
Axial (A) and coronal (B) computed tomography scans of a 40-year-old male patient with Kimura disease display multiple lesions in the right parotid gland and right cervical lymph nodes. The patient received steroids and radiotherapy after surgery, but relapsed.
The follow-up period was 69.5 ± 17.4 months (range, 2-144 months). During the follow-up period, 5 patients relapsed. Only long symptom duration had statistical significance in the recurrence of Kimura disease, while age, size, peripheral blood eosinophilia, and high immunoglobulin E (IgE) concentrations had no statistical significance.
Discussion
Kimura disease is a rare disease whose exact mechanism has not yet been identified, although various hypotheses have been proposed, such as allergic reactions, infections, and/or autoimmune reactions.1-11 Kimura disease can accompany atopy or nephrotic syndrome, and in this study, 2 patients and 1 patient, respectively, had the co-morbid conditions listed.2,3,4,6,11
The most common symptom of Kimura disease is an asymptomatic mass that frequently involves the regional lymph nodes or salivary glands.1,2,4-7 In this study, all patients with Kimura disease except 1 presented with a neck mass, with bilateral lesions in 3 patients. In addition, multiple lesions in the head and neck region were observed except for 1 patient with Kimura disease in the buccal space (Figure 1).
Laboratory examination revealed elevated peripheral blood eosinophilia and increased IgE concentration.2,3,6 CT scan reveals an ill-defined lesion involving subcutaneous tissues and salivary glands with ipsilateral lymphadenopathy.3,4,6 Kimura disease is characterized by an ill-defined solid heterorechoic lesion on US and a heterogeneously hyperintense lesion on MRI T2. 6 However, these laboratory and imaging assessments cannot definitively diagnose Kimura disease, and histopathological examination is essential.1-11 In general, FNAC is inadequate for diagnosing Kimura disease.2,3,5 Herein, Kimura disease could not be diagnosed in the 5 patients who underwent FNAC.
A standardized treatment method for Kimura disease has not yet been established.1-11 The most commonly used treatment methods are surgery, steroids, immunosuppressants, and radiotherapy. Because Kimura disease generally requires surgery for diagnosis, surgery is the main treatment method. However, additional treatment after surgery is often required because of the high rate of relapse.1,3,5,6 Kimura disease has a very high recurrence rate of 25% to 100%, but fortunately, malignant changes do not usually materialize.1-3,5,7,8 In this study, the relapse rate was also high at 62.5%, but malignant changes did not transpire. However, Kimura disease can cause renal complications such as nephrotic syndrome in about 60% of patients, so caution is needed.2,3,4,6
Relapse rates are associated with large lesion size, long symptom duration, peripheral blood eosinophilia, and high IgE concentrations. 8 In this study, a statistically significant difference in Kimura disease recurrence was observed only in patients with a longer symptom duration (P < .05), which may be due to the small number of enrolled patients. This study has limitations in that it has a small sample size and is a retrospective study. Future prospective studies with larger cohorts will further enhance the impact of the findings.
Conclusion
Kimura disease is a rare disease of unknown etiology and is difficult to diagnose. However, clinicians should suspect Kimura disease based on asymptomatic masses, peripheral blood eosinophilia, and imaging examinations and make a definitive diagnosis via surgery.
Footnotes
Acknowledgements
The authors have no acknowledgments to disclose for this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent Statements
The study was approved by the Institutional Review Board of Chonnam National University Hwasun Hospital (Ethical Clearance Reference Number: CNUHH-2023-166) on August 24, 2023. All participants provided written informed consent prior to participating.