
Abstract
A tonsillar mass in a young patient with no medical issues routinely presents as an infectious process. Practitioners must maintain a broad differential if diagnostic testing does not support an infection. Neoplasm must be excluded. Otolaryngologists must consider malignancies other than squamous cell carcinoma, the most common oropharyngeal malignancy, and lymphoma. Rare tumors, such as sarcomas, must also be considered. Otolaryngologists must be familiar with the proper management of rare oropharyngeal malignancies.
A 23-year-old, previously healthy male presented to the emergency department (ED) with 2-weeks of progressive odynophagia, dysphagia and dysphonia. On physical exam, the left tonsil was enlarged compared to the right with associated partial palatal effacement, contralateral uvular deviation, and trismus. Computerized tomography (CT) soft tissue neck with contrast revealed a 1.5 cm left tonsillar mass, which was presumed to be a peritonsillar abscess by an emergency medicine physician. The lesion was decompressed by the ED physician using fine needle aspiration with return of scant purulent fluid. The patient returned to the ED 2 months later worsening dysphagia, odynophagia, dysphonia, and globus sensation. The patient had severe effacement of the left peritonsillar region and rightward uvular deviation with mild erythema and no exudate or purulence noted on exam. A repeat CT soft tissue of the neck with contrast was obtained, revealing a 4.7 × 3.7 × 5.3 cm exophytic soft tissue mass arising from the left palatine tonsil without cervical adenopathy (Figures 1A-C). (A) Axial CT scan of mass, (B) Coronal CT of mass, (C) Sagittal CT scan of mass.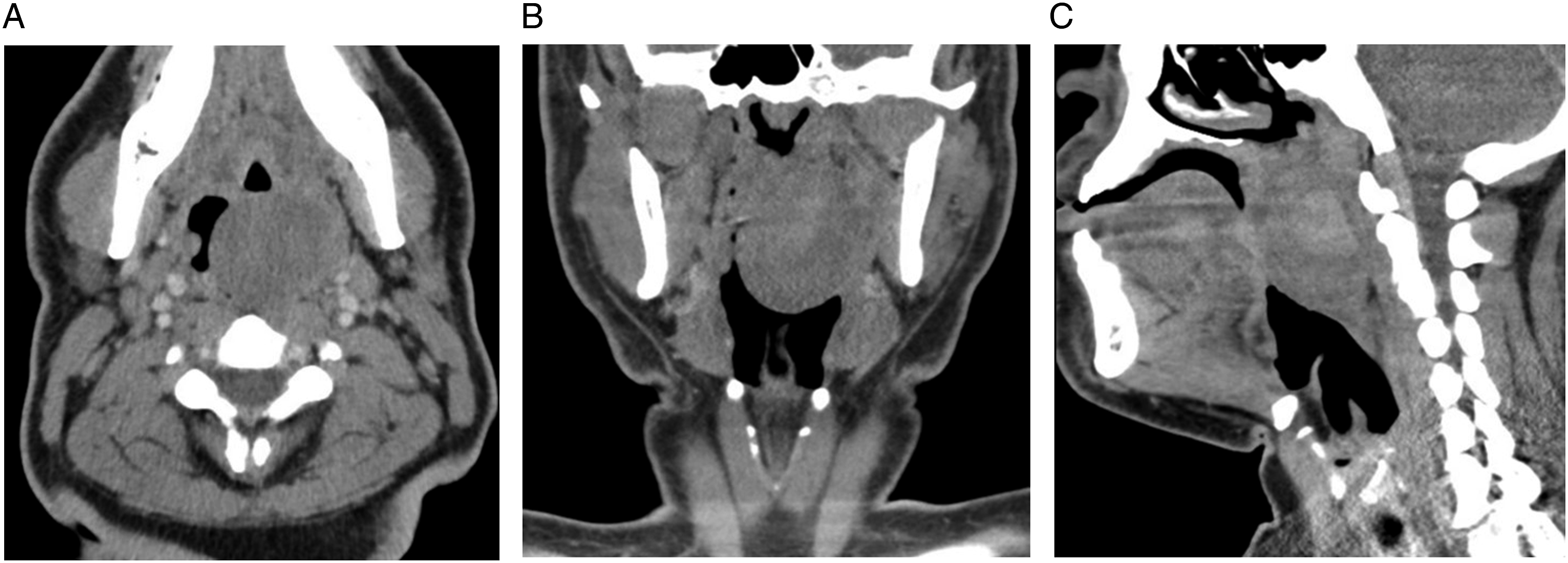
The patient underwent incisional biopsy in the operating room. Intraoperative frozen sections suggested a malignant process with a preliminary read of synovial sarcoma. The patient was lost to follow-up for 2 months, but returned to the emergency department 2 months later with progressive odynophagia, dysphagia, dysphonia, and dyspnea. There was near complete occlusion of the oropharynx by an irregular, highly necrotic mass (Figure 2). Postoperative recurrence roughly 1.5 months after original excision.
The patient underwent an emergent, awake open tracheotomy. Magnetic resonance imaging (MRI) of the head and neck with contrast at that time revealed a heterogenous T1-weighted and markedly T2-weighted hyperintense oropharyngeal mass measuring 5.6 × 4.4 × 5.2 cm (Figures 3A-B). Positron emission tomography (PET) scan revealed a lobulated oropharyngeal mass along the left wall extending into the laryngopharynx measuring 4.7 × 5.1 × 6.1 cm (SUV 16) with no evidence of local or distant metastasis. (A) T1-weighted coronal MRI showing oropharyngeal mass, (B) T2-weighted coronal MRI showing oropharyngeal mass.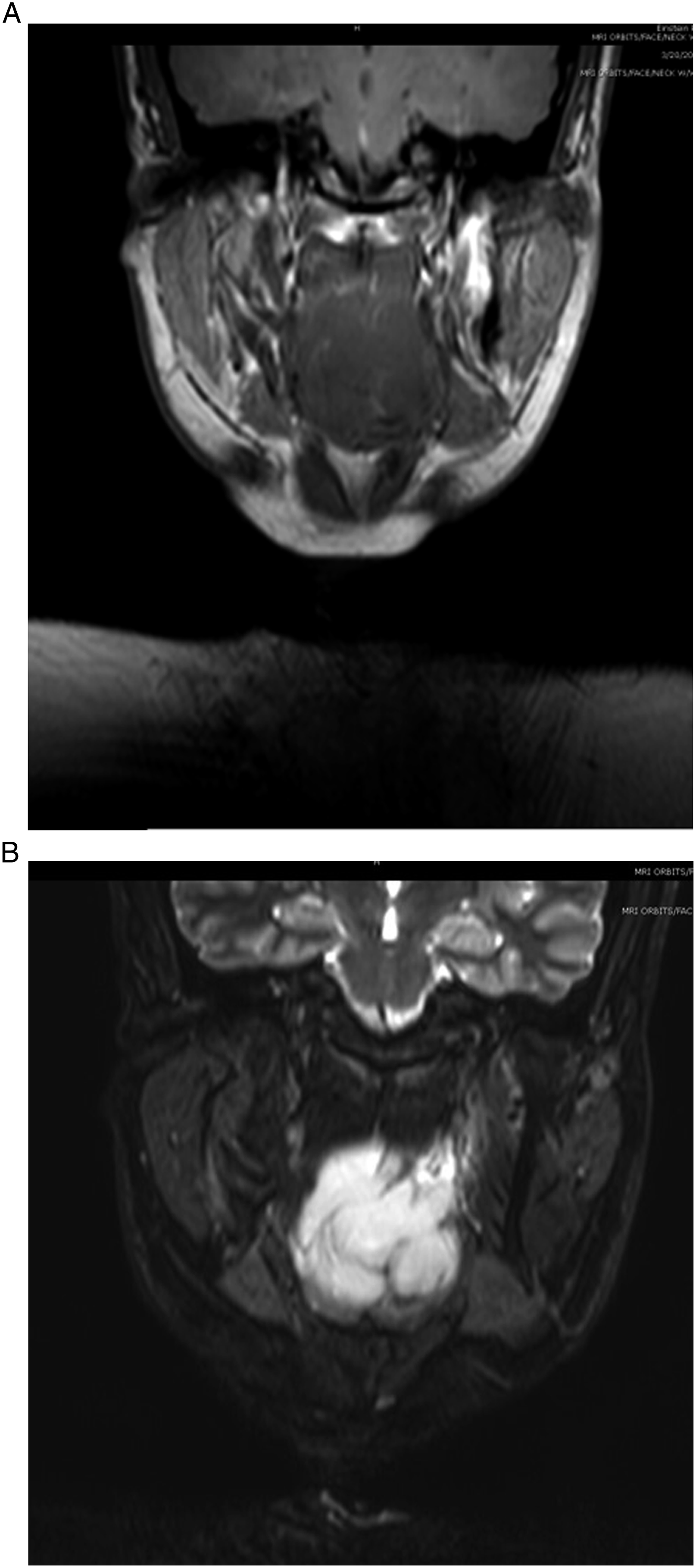
The patient underwent a surgical resection via paramedian lip-split mandibulotomy and partial oropharyngectomy (Figures 4A-B). (A) Intraoperative BCOR-rearranged oropharyngeal sarcoma prior to debulking and excision, (B) Intraoperative BCOR-rearranged oropharyngeal sarcoma postexcision.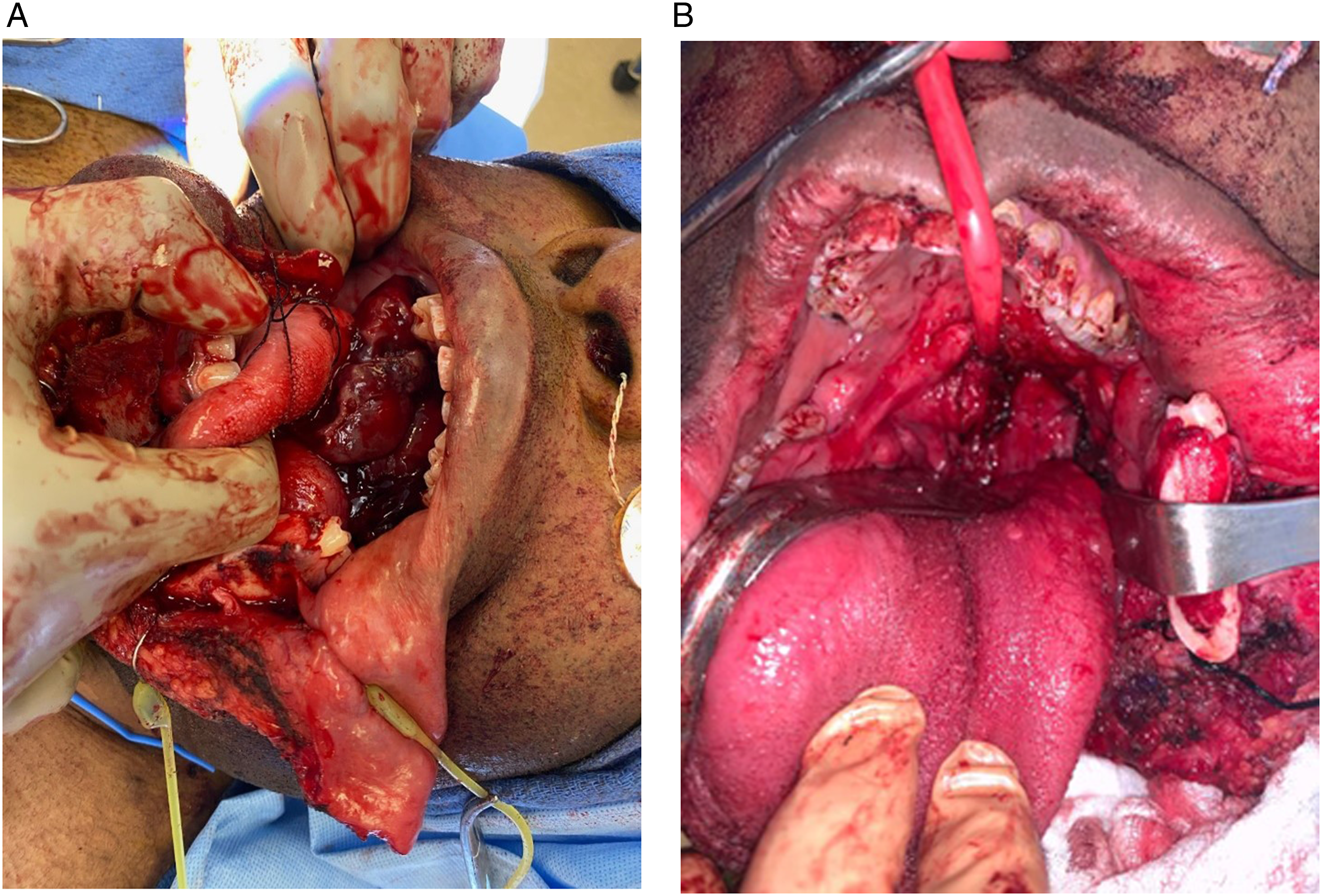
Pathology revealed high grade, undifferentiated round cell sarcoma with a mitotic rate of 30/10 high-power fields (Figure 5). Immunohistochemistry was positive for BCL-2 and CD56, and negative for EMA, AE1/3, CK5/6, S100, synaptophysin, chromogranin, desmin, p63, P40, CD34, CD21, CD 43, and SS 18-SSX fusion. Methylation pathologic review was performed and revealed a match to small blue round cell tumors to BCOR alteration. Sequencing was negative for BCOR internal tandem duplication, suggesting fusion related alterations. Final surgical margins did reveal residual microscopic disease. The patient was staged as pT3N0cM0 (AJCC 8th Edition). The patient was scheduled to undergo chemotherapy every 3 weeks alternating between two regimens for a total of 8–10 cycles of each. The first regimen included vincristine, doxorubicin, cyclophosphamide, and mesna. The second regimen included mesna, ifosfamide, and etoposide. The patient would receive Neulasta at the end of each completed cycle. The patient received one cycle then refused further treatment. Photomicrograph of the tumor shows an undifferentiated sarcoma with round to ovoid cells and increased mitoses (Hematoxylin and eosin stain, 200X).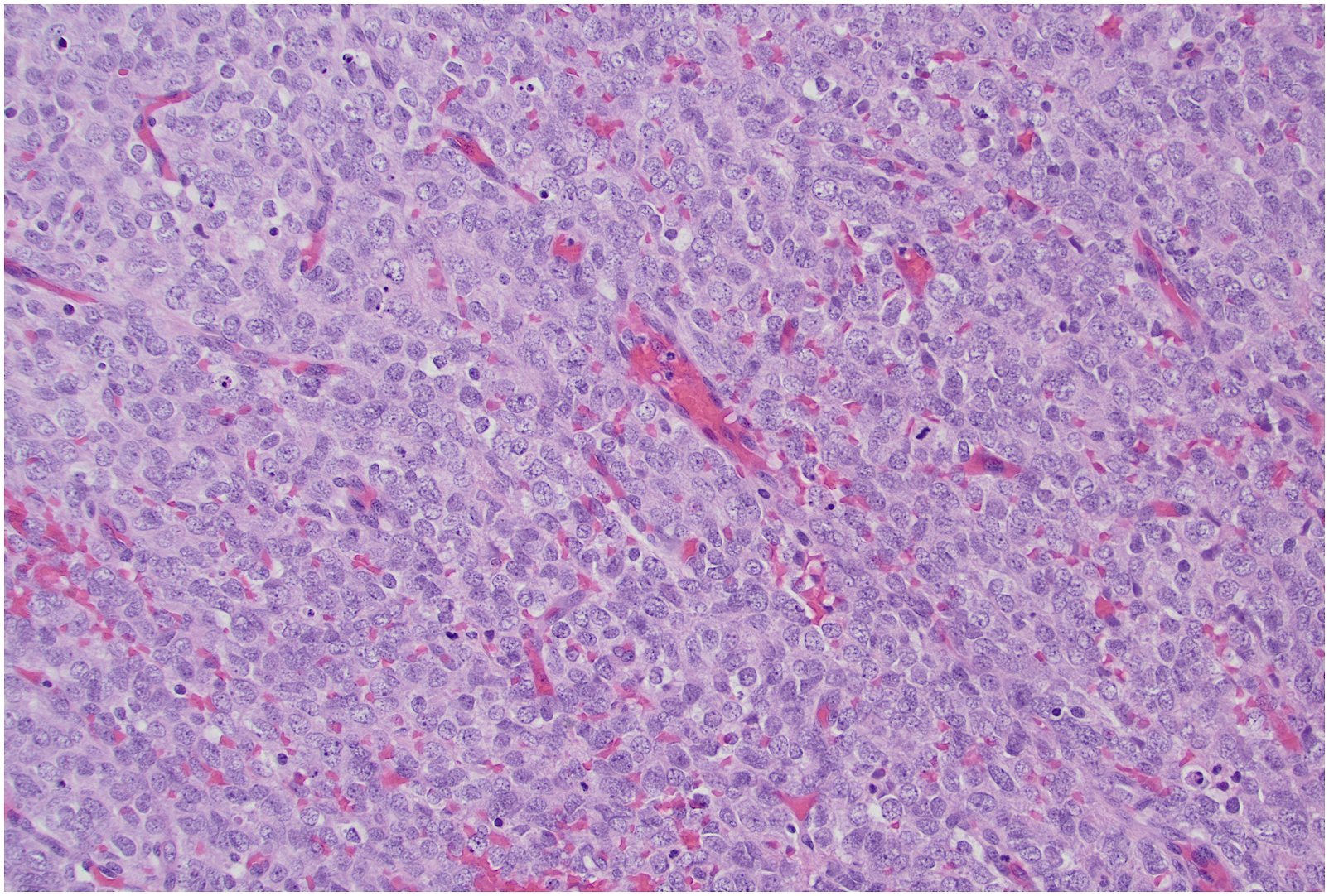
BCOR (encoding Bcl-2 interacting corepressor) sarcomas have emerged as a relatively newly defined category of sarcomas. The mean age of patients with BCOR sarcomas is 15 years, with a strong male predominance. The location for these tumors is most commonly bone, with the pelvis and long bones most commonly affected, followed closely by soft tissue, and rarely in visceral organs.1,2 The uterus is the most common site in the adult population, which is exceedingly rare.3,4
Histologically, these tumors are characterized by uniform small round cells with fine chromatin pattern, as well as short, spindle- or epithelioid-shaped cells, proliferating in multinodular and sheet-like patterns, and a rich vascular background. 5 BCOR is ubiquitously expressed in numerous tissues, but BCOR immunoreactivity is found just in the testis and weakly in the germinal centers of tonsils. 6 Grossly, these tumors exhibit evidence of hemorrhage and necrosis and the typical MRI features include heterogeneously enhancing lytic bone lesions with cortical destruction and associated infiltration of surrounding soft tissue. 7
BCOR-rearranged sarcomas are most commonly treated with Ewing sarcoma protocols, with induction chemotherapy followed by surgical resection, and response rate is similar. 7 A study of BCOR-CCNB3 positive sarcomas found the tumors to be very chemosensitive. 8 The 5-year overall survival for BCOR sarcomas is approximately 75%, similar to that of Ewing sarcoma. BCOR sarcomas in the axial skeleton and soft tissues show a significantly shorter survival time compared to long bone tumors. 7 To date, no studies have investigated the role of radiation therapy in the treatment of BCOR-rearranged sarcoma.
A tonsillar mass that does not fit the picture of an infectious process must have a broad differential. When the patient has non-specific symptoms, is non-toxic appearing, afebrile, with no leukocytosis or tonsillar exudates, neoplasm must be considered. More specifically, neoplasms other than lymphoma and squamous cell carcinoma must also be considered. Initial workup should include a CT neck with contrast and biopsy. BCOR-rearranged sarcoma is an extremely rare etiology for a tonsillar tumor and requires a multidisciplinary approach to achieve favorable outcomes.
Footnotes
Author Contributions
Concept and design: SB, TL, MS, AB, SZ.
Acquisition, analysis, and interpretation of data: SB, TL, MS, AB, SZ.
Drafting of the manuscript: SB, TL, MS, AB, CM, RB.
Critical revision of the manuscript for important intellectual content: SB, TL, MS, AB.
Accountability for all aspects of the work: SB, TL, MS, AB, SZ, CM, RB.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.