
Abstract
Ewing-like sarcomas (ELS) are round cell mesenchymal neoplasms that are highly aggressive to bone and/or soft tissue. However, they rarely occur in the nose, with no reported such cases in the medical literature to date. Here, we reported the case of a two-year-old Chinese boy who presented with a mass in the left nasal cavity. Surprisingly, the final histopathological diagnosis of the nasal mass was determined to be a subtype of ELS, BCOR-rearranged sarcoma. Therefore, we retrospectively analyzed the clinical data of this case and reviewed the relevant literature on ELS and BCOR-rearranged sarcoma. The purpose of this article is to provide new insights into the clinical characteristics of children with BCOR-rearranged Ewing-like sarcoma and to improve the understanding of this disease.
Introduction
Ewing-like sarcomas (ELS) are an emerging family of small round cell sarcomas with varying degrees of clinical, morphological, and immunohistochemical similarities to Ewing sarcoma (ES), 1 which mainly invade bone or soft tissue and are common in the pediatric and young adult population 2 . However, ELS lack the classical fusion partners of ES and require specific genetic testing to distinguish these two types of tumors. 1,3,4 Recently, with the development of modern molecular sequencing methods, a series of novel molecularly-driven events have been discovered that have facilitated patient management and the differentiation and classification subgroups of Ewing sarcoma family tumors. 1,4,5 The new classification of ELS has been updated to include capicua transcriptional repressor (CIC)-rearranged sarcoma, BCOR-rearranged sarcoma, EWSR1 non-ETS rearranged sarcoma, and unclassified/undifferentiated small round cell sarcoma. 1,6 -8 Here, we described a rare case of a left nasal BCOR-rearranged Ewing-like sarcoma. We have also discussed the genetic, pathological, and therapeutic characteristics of this disease.
Case presentation
General information
A two-year-old boy presented with a three-month history of a mass in the left nasal cavity. No swelling, pain, or epistaxis were detected. Anterior rhinoscopy revealed a localized round soft neoplasm in his left nasal cavity that was compressing the left nasal alar (Figure 1). The right nasal cavity was asymptomatic. No history of trauma or chronic diseases was reported. Physical examination of the ear, nose, and throat, showing a local and round soft neoplasm in the left nasal cavity, that was compressing the left nasal alar.
Imaging examination
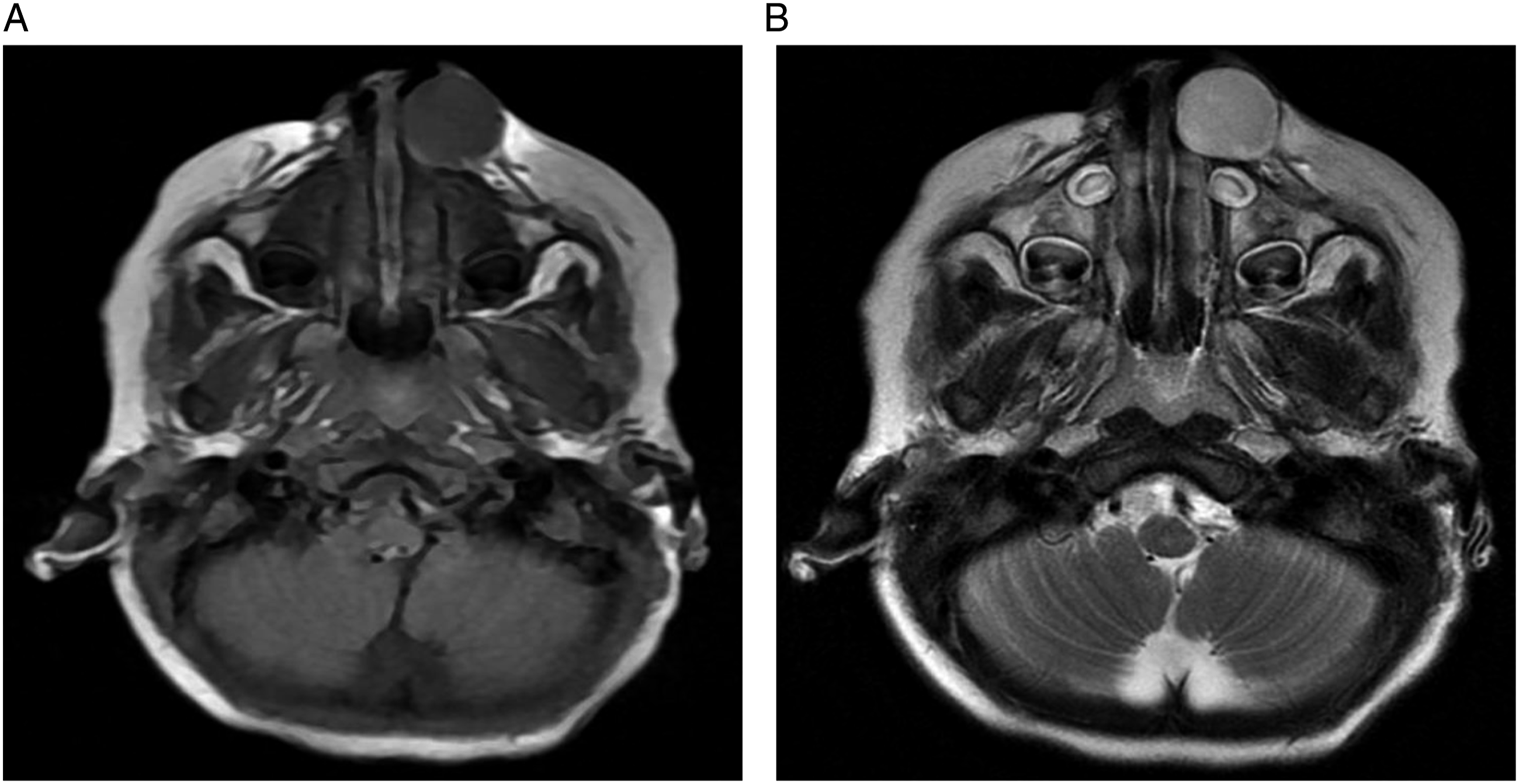
Computerized tomography (CT) and magnetic resonance imaging (MRI) revealed the presence of a round, 2.2cm-diameter mass in the left nasal cavity and the anterior maxilla. CT showed that the left nasal cavity was narrow, with a clear boundary and uniform density; and the anterior edge of the maxilla was compressed and deformed (Figure 2). MRI revealed that the lesion had slightly longer T1 and T2 signals with a clear boundary (Figure 3). CT image. (A). the left nasal cavity was narrow, with a clear boundary and uniform density; (B). the anterior edge of the maxilla was compressed and deformed (B). MRI showing that the lesion had slightly longer T1 and T2 signals with a clear boundary. (A). T1WI (B). T2WI.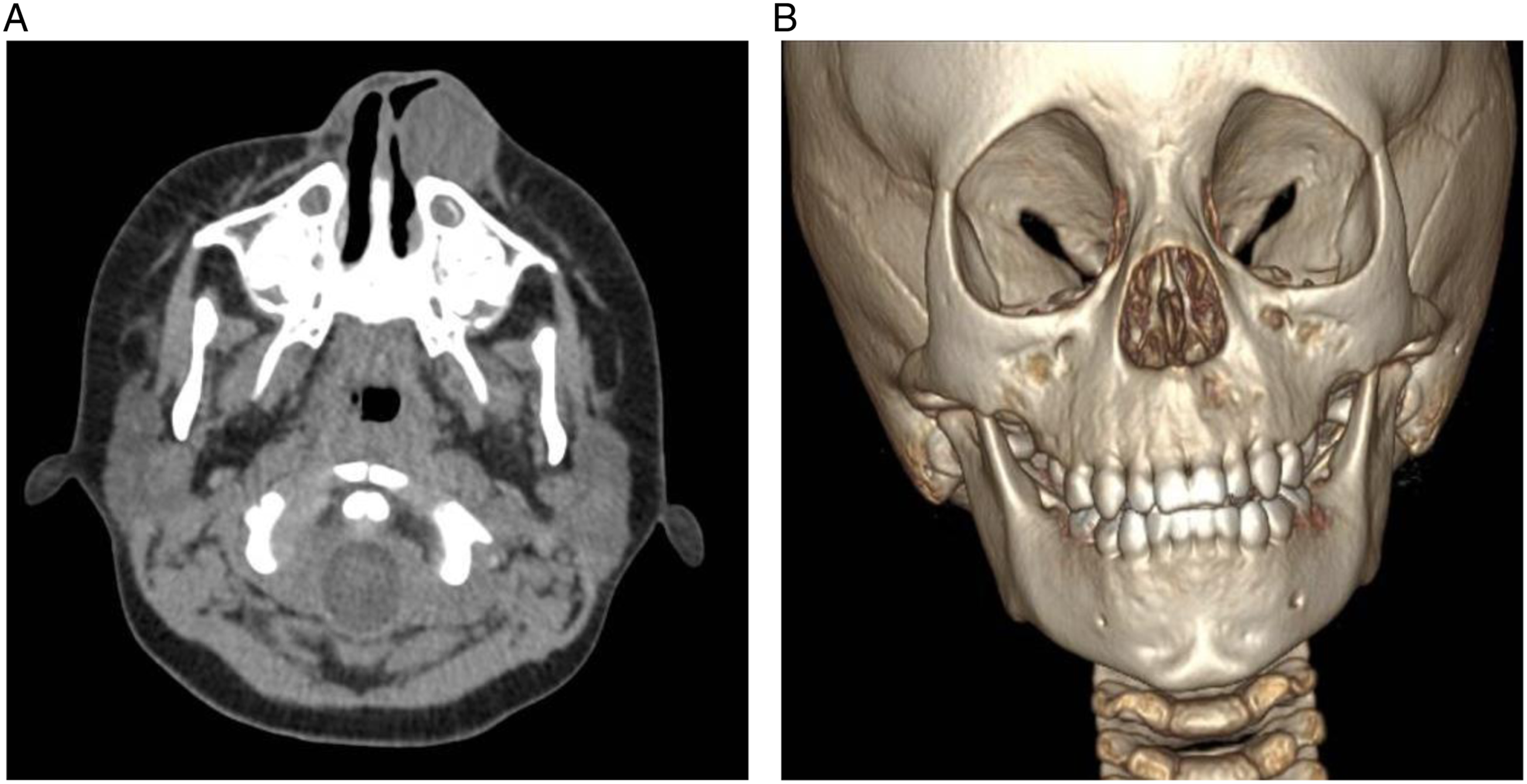
Treatment and follow-up period
To further clarify the nature of the tumor, this patient was subjected to ultrasound-guided fine-needle aspiration biopsy, whose pathological examination showed that it was a small round cell malignant tumor. Molecular pathological analysis was further performed, and the histomorphology and immunophenotype were found to be consistent with the characteristics of BCOR-rearranged sarcoma (Figure 4). The results of the molecular pathological tests are as follows: BCOR (+), Ki-67 (30%+), Cyclin D1 (+), S-100 (+), CD99 (-), CCNB3 (-), INI-1 (-), CD34 (-), SMA (-), CK(AE1/AE3) (-), MUC-4 (-), Desmin (-), Myogenin (-), MyoD1 (-), ALK (-), SATB2 (+), MDM2 (+), TLE1 (+), ERG (-), GFAP (-), Calretinin (-), and WT-1 (-). After the diagnosis, the child underwent four rounds of VDC chemotherapy, followed by surgery through the Caldwell-Luc approach under general anesthesia to remove the nasal mass. Chemotherapy was continued after surgery. No alar abnormality or no recurrence was found during the four-month follow-up period (Figure 5). The pathological examination of the tumor in the left nasal cavity. (A). hematoxylin-eosin (HE) staining; (B). BCOR staining. The nasal shape at the 4-month postoperative follow-up examination.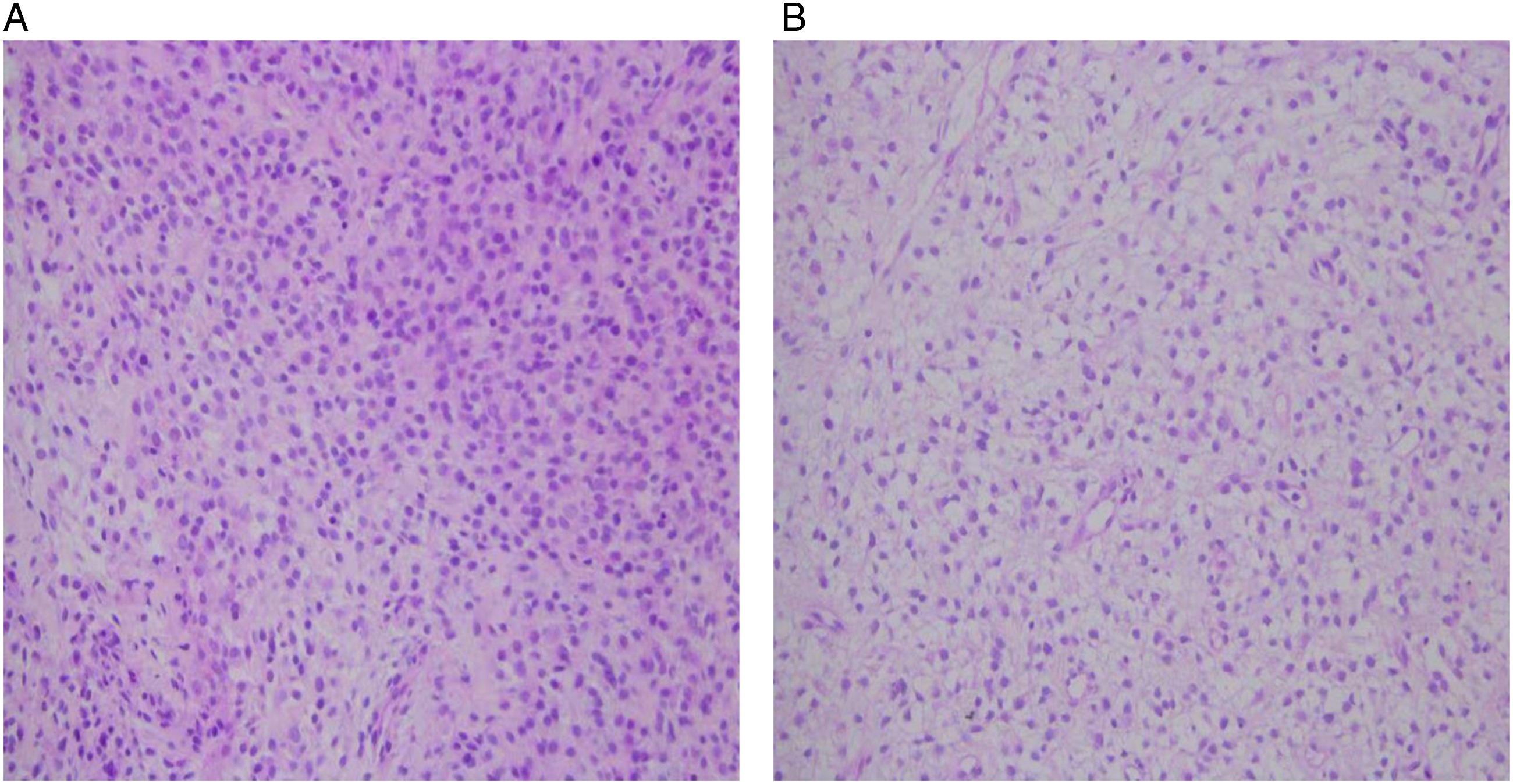

Discussion
Small round cell sarcomas are a group of rare, aggressive and poor-prognosis malignant entities, of which Ewing sarcoma (ES) occurs most frequently. Ewing-like sarcomas (ELS) are the second most common entities after ES (80%), accounting for 11% of all cases. 3,6 The clinical, morphological, and immunohistochemical characteristics of ELS overlap with those of ES, 1 making differential diagnosis challenging. In recent years, with the development of immunohistochemistry and molecular detection technology, an increasing number of fusion genes have been detected by specific genetic testing, such as fluorescence in situ hybridization (FISH), real-time polymerase chain reaction (RT-PCR), and next-generation sequencing, 1,9 enabling the identification of these small round cell sarcomas. 10 ELS were reported to lack the classical hallmarks of ES, namely, the rearrangements between EWSR1/FUS and the members of the E26 transformation-specific (ETS) family of transcription factors, but other newly identified fusion genes continue to expand the spectrum of ELS 1,3 . Thus far, ELS have been classified into four subtypes based on these specific fusions, that is, capicua transcriptional repressor (CIC)-rearranged sarcoma, BCOR-rearranged sarcoma, EWSR1 non-ETS rearranged sarcoma, and unclassified/undifferentiated small round cell sarcoma.
Such a rare and heterogenous group of tumor subtypes of ELS typically originate in the bone and/or soft tissue and affect pediatric and young adult patients, 2 characterized by distinct clinical and histological characteristics. CIC-rearranged sarcoma is the most common tumor of these ELS subtypes, presented mostly with CIC–DUX4 fusion, invasiveness, high-expression of ETV4 and WT1, and histological characteristics of undifferentiated round cells. 11 BCOR-rearranged sarcoma is the second most common variant, manifesting mainly with BCOR-CCNB3 fusion, arising from a paracentric inversion of the X chromosome; and males are highly susceptible to this subtype. 1 Both EWSR1 non-ETS rearranged sarcoma and unclassified/undifferentiated small round cell sarcoma have atypical clinical, morphological, and immunohistochemical characteristics which differentiate them from ES. 1 Therefore, any generalizations about clinical characteristics and optimal treatment strategies are uncertain and challenging. Molecular detection technology is clinically used to detect these characteristics, confirm the diagnosis, and facilitate the clinical differential diagnosis. The left nasal tumor of the two-year-old boy was histopathologically diagnosed as BCOR-rearranged sarcoma. To date, no such case has been reported in the available medical literature.
An increasing number of studies on BCOR-rearranged sarcoma are have been now conducted, and the characterization of their clinical, morphological, and immunohistochemical properties continues. Previously, Pierron et al. 9 identified for the first time 24 BCOR-CCNB3-positive tumors out of 594 sarcomas, showing that CCNB3 immunohistochemistry analysis is a powerful diagnostic marker for the detection of this subtype of ELS. Accumulating evidence has revealed that BCOR-rearranged sarcoma primarily originates in the bone (e.g., the limb bones and pelvis), with less common soft tissue involvement. 3,12,13 The median age of onset is usually within of the first two decades of life. 14,15 BCOR-rearranged sarcoma is more likely to occur in males, 1 which may be associated with an X-chromosomal paracentric inversion. 2,15,16 Additionally, the typical radiographic features (CT/MRI) of BCOR-rearranged sarcoma are characterized by aggressive bone lesions with large soft tissue masses. Conversely, the CT and MRI findings of the bone and soft tissue with BCOR-rearranged sarcomas are rather nonspecific, with no clear features distinguishing it from ES. 12,17 However, possible distinct manifestations may include a more heterogenous appearance on MRI and the presence of soft tissue calcifications in BCOR-rearranged sarcomas. 12 Morphologically, the cells of BCOR-rearranged sarcoma have round, short fusiform, or sheet-like arrangement. The nucleoli are monomorphic and inconspicuous, and the stroma is rich in fine capillary networks, myxoid or collagenous degeneration. 14,18 Immunohistochemical examination showed that BCOR-rearranged sarcomas mainly expressed BCOR and/or CCNB3, whereas BCOR is also expressed in synovial sarcoma 19 ; thus, the former is not as specific as the latter. 20,21 Moreover, other markers, such as CD99, CD117, Ki-67, BCL-6, BCL-2, TLE1, SATB2, and cyclin D1, can be expressed to varying degrees in BCOR-CCNB3 sarcomas, but not specifically. 15,20,22,23 Prior studies have reported that the overall survival of BCOR-CCNB3 sarcoma was 72% during the 5-year follow-up, which was similar to that in ES (79%) and better than the one of CIC–DUX4 sarcomas (43%). 1,15,18
From a clinical point of view, the treatment of ELS is comprehensive, requiring a combination of surgery, chemotherapy, radiotherapy, and immunotherapy. 1 Unlike other subtypes of ELS, patients with BCOR-rearranged sarcomas have survival rates similar to those of ES patients and are more sensitive to classical ES chemotherapy regimens. 15,18 Currently, although most of BCOR-rearranged sarcomas are treated with ES chemotherapy protocols, non-Ewing treatment strategies can also be considered a safe approach, which can provide new treatment opportunities and challenges for treatment. 24 In the future, more research is needed on the genetics, pathology, and treatment of small round cell sarcoma, especially ELS.
Conclusion
BCOR-rearranged sarcoma is one of the subtypes of ELS. It is more common in male patients and usually involves the limb bones, pelvis, and/or soft tissues, but the nasal BCOR-rearranged sarcoma is relatively scarce. Here, we report a rare case of two-year-old boy with the left nasal BCOR-rearranged sarcoma who received a combination of ES chemotherapy and Caldwell-Luc surgery. Until the point of the preparation of this manuscript, a four-month postoperative follow-up period has been completed, with no recurrence or nasal alar abnormality. Nevertheless, a longer follow-up period is required for obtaining more comprehensive, objective, consistent, and representative information on the exact treatment effects.
Footnotes
Author contributions
Prof. Ni Xin, Prof. Wang Shengcai, and Prof. Zhang Jie designed the case study and revised the manuscript; Dr. Li Yanzhen, Dr. Zhang Xuexi, and Dr. Liu Qiaoyin collected clinical data and completed the follow-up period examinations of this case; Dr. Sun Nian, Dr. Liu Zhiyong and Dr. Liu Yuwei searched for relevant literature sources; Dr. Tingting Ji and Dr. Xiaodan Li composed the original manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the grants as follows: National Natural Science Foundation of China (82000991), Beijing Hospitals Authority Youth Programme (QML20201206), and Capital Funds for Health Improvement and Research (2018-1-2091).
Ethics approval
This study was approved by the Medical Ethics Committee of Beijing Children’s Hospital. A piece of written informed consent was obtained from the parents of the child for publication of this case report and any accompanying images.
Data availability statements
The information and images for this article are available online and completely open to the public.