
Abstract
Adenoid cystic carcinoma (ACC) is a malignant tumor arising from the salivary glands. While surgery is the mainstay of treatment for ACC of the palate, adjuvant radiotherapy and/or chemotherapy should be considered in high-risk cases. Oronasal fistula, a complication of palatal surgery, may cause speech disturbance and food regurgitation; the nasoseptal flap is a potential option to repair this defect as it is readily available and reliable. Here, we present a case of locally advanced ACC of the palate in a patient who underwent endoscopic-assisted transoral tumor excision with nasoseptal flap reconstruction postoperative chemoradiotherapy.
Introduction
Adenoid cystic carcinoma (ACC) accounts for approximately 10% of all salivary gland neoplasms and is the most common malignancy of the minor salivary glands. This tumor is characterized by slow growth, a high risk of local recurrence, and delayed distant metastasis, with an incidence rate of 40–50% for the latter. The lung is the most common organ of metastasis, followed by osseous metastasis.2,3 ACC further presents a strong neurotropism, and perineural invasion can be observed even in early-stage tumors.
ACC most frequently arises from the palate, followed by the tongue and oral mucosa.1,2 For palatal ACC, surgical resection is the primary treatment. However, the tumor location makes complete resection difficult. The tumor may recur locally along the surgical margin or disseminate from the large nerve trunk. Consequently, a multidisciplinary treatment plan, including combination therapy with radiotherapy and/or chemotherapy, should be considered. Furthermore, surgical resection of palatal malignant tumors often results in oronasal fistula, which is defined as a pathological connection between the oral and nasal cavities through the hard or soft palate. The fistula causes hypernasality and leakage of food or liquid into the nasal cavity, which can greatly affect quality of life. Different strategies have been introduced to reconstruct the defect, including the use of local oral cavity flaps and free tissue flaps. The nasoseptal flap technique, first described in 2006, has been widely used in endoscopic skull base surgery. 4 Some recent studies have indicated the nasoseptal flap as a good resource to repair oronasal fistula with minimal donor site morbidity, a short harvest time, and a short recovery period.4,5
Herein, we present a case of ACC of the palate with locally advanced staging. The aim of this study is to share our experience of the treatment of palate ACC and to review the literature on the management and prognosis of this cancer.
Case Report
A 36-year-old Asian man visited our ear-nose-throat outpatient unit with the chief complaint of progressive swelling of the right palate for 4 months. The patient presented with right nasal obstruction, dysphagia, and odynophagia. He had visited another hospital 1 month prior, where biopsy revealed a pleomorphic adenoma. At this prior hospital, maxillectomy with free flap reconstruction was suggested; however, the patient refused and visited our hospital for a second opinion. Clinical examination revealed a 4 cm, firm, and immobile tumor in the right soft palate, with tenderness on palpation. There were no palpable lymph nodes bilaterally in the neck. Magnetic resonance imaging revealed a well-enhanced tumor originating from the soft palate, extending anteriorly to the hard palate, posteriorly to the posterior pharyngeal wall, upward to the nasopharynx, and laterally to the right parapharyngeal space (Figure 1). The palatal tumor extended to nasopharynx and right parapharyngeal space, which was well enhanced in T1-weighted image.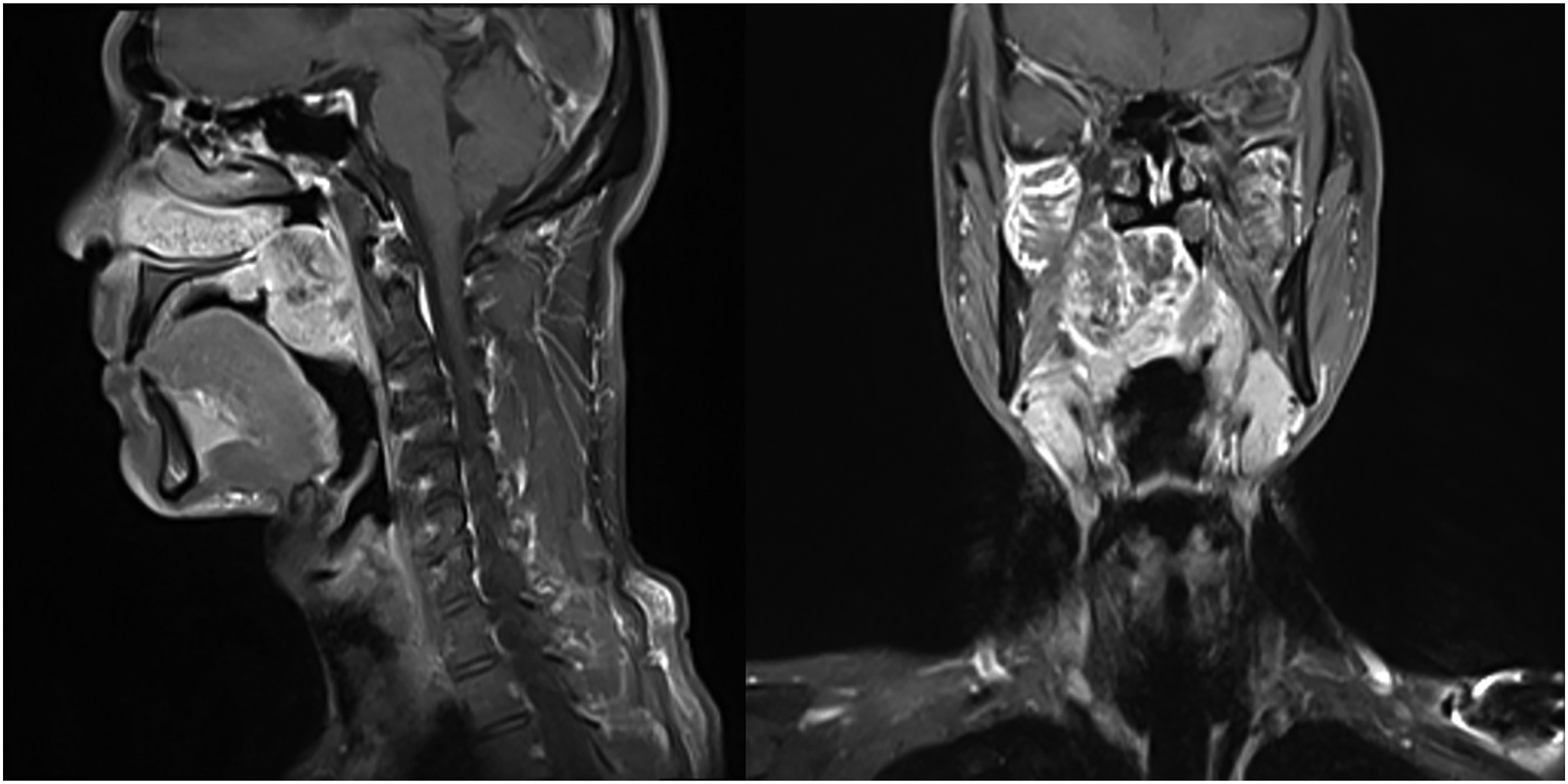
The patient underwent endoscopic-assisted transoral tumor excision and nasoseptal flap reconstruction of the palate defect. First, the nasoseptal flap was harvested, and the nasal floor mucosal flap was carefully elevated and protected. The tumor was resected transorally, and the right tonsil was resected to achieve adequate posterolateral surgical margins. A defect connecting the oral and nasal cavities was observed after tumor removal. The nasoseptal flap was transposed and sutured to repair the defect, and free mucosal grafts harvested from the inferior turbinate were used to cover the bare bone area in the nasal cavity. The wounds in the oral cavity and oropharynx were primarily closed (Figure 2). The surgery was performed smoothly without complications. Histological examination confirmed the diagnosis of ACC, 4.3 cm in size. Microscopically, the tumor showed a predominantly cribriform structure with admixed tubular and solid components. Intratumoral perineural invasion was also observed. The tumor was close to the deep surgical margin (1 mm) while negative frozen section margins have been obtained at the same direction. Tumor staging was pT3 cN0M0, stage III according to the AJCC 8th edition. (A) The tumor located at right soft palate, about 4 cm in size. (B) A defect developed after the tumor removal, causing the connection between oral and nasal cavity. (C) The nasoseptal flap (arrow) was employed to repair the defect, and the bare donor site was covered with a free mucosal graft (asterisk) harvested from the resected inferior turbinate. (D) The wound in oral cavity and oropharynx was primarily closed.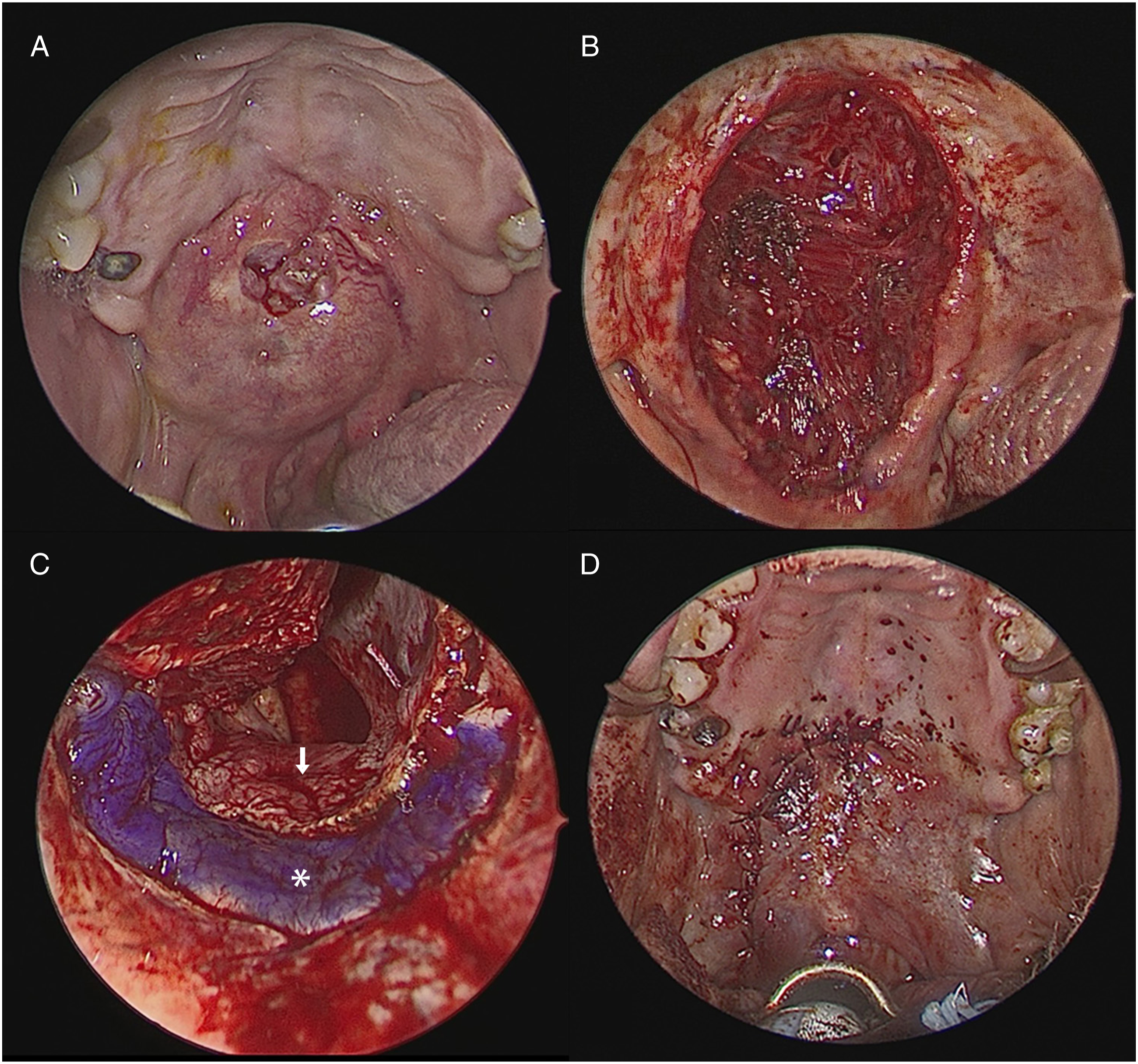
Considering the risk factors, including locally advanced staging, close margins, and perineural invasion, 66 Gy of adjuvant intensity modulated radiation therapy with concurrent cisplatin-based chemotherapy was applied. The right parapharyngeal space and adjacent skull base were covered in the radiation field to prevent recurrence along the cranial nerves. No local recurrence or distant metastasis was observed one year after treatment.
Discussion
ACC is a rare malignant tumor that most often arises in the minor salivary glands (approximately 50%). 6 Other locations include the major salivary glands, aerodigestive tract, lacrimal glands, and adnexal skin glands. 7
The 5-year survival rate of patients with ACC ranges from 67 to 73%. However, due to the characteristics of delayed locoregional recurrence and distant metastasis, the 10-year and 20-year survival rates are much worse. Adverse prognosis factors have been reported in previous studies, including the histologically solid subtype, major nerve involvement, positive surgical margin, and advanced staging.2,8
Different treatment modalities have been established for ACC, including surgery, radiotherapy, chemotherapy, and combination therapy, although surgical resection is generally accepted as the primary treatment modality. A combination of surgery and radiotherapy is a common choice to obtain a better locoregional control rate. Chen et al. reported a significant improvement in local control in patients who underwent surgery combined with radiotherapy, although no benefit of postoperative radiotherapy was found for distant metastasis. 9 Concurrent use of postoperative chemotherapy and radiotherapy is generally considered in patients deemed to have a higher risk of recurrence. However, the response rates and durations were variable and inconsistent. 10 In our case, multiple risk factors were present, including close margins, advanced T staging, and perineural invasion. Therefore, after a thorough discussion with the patient, we decided to administer adjuvant chemoradiotherapy.
In this case, to avoid the oronasal fistula, a nasoseptal flap was elevated before tumor resection. Oronasal fistula is a major complication of palatal surgery, which may cause hypernasality and nasal regurgitation of food. Therefore, different methods have been introduced to repair these defects. Local palatal flaps, with or without costal cartilage grafts or dental obturators, are commonly used to treat smaller defects. Buccal and tongue flaps are used for larger defects but require a second-stage operation to divide the pedicle. The facial artery myomucosal flap, temporoparietal galeal flap, turbinate flap, and free tissue flap have also been reported for closure of oronasal fistulas.11,12 Nasoseptal flap is widely used in endoscopic reconstruction of skull base defects. Recently, several attempts have been made to apply nasoseptal flaps for the reconstruction of palatal fistulas. Several advantages of this pedicle flap have been reported. First, it is convenient to harvest, with minimal donor site morbidity and a short recovery period. Second, the flap can be harvested at a sufficient size for most oronasal fistulae smaller than 2.5 cm. Third, the well vascularized tissue flap is sufficiently strong to endure radiation therapy and heals well without necrosis.4,5
The patient is followed at our clinic tri-monthly, and no locoregional recurrence could be found by physical examination and nasopharyngoscopy one year after treatment. MRI of oropharynx and chest X-ray showed no recurrence or distant metastasis. The condition of nasoseptal flap was excellent without necrosis or perforation. The patient did not experience any other sequelae from the treatment, except for mild dysgeusia, which continued to improve. Long-term surveillance by annual chest X-ray for at least 10 years is essential owing to the tendency of late pulmonary metastasis. In conclusion, our experience showed that the nasoseptal flap is a feasible solution for reconstructing oronasal fistulas following palatal tumor resection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
We had got the approval from MacKay Memorial Hospital Institutional Review Board Approval of Clinical Trail. IRB number: 22MMHIS165e.