
Abstract
The occurrence of an isolated schwannoma in the olfactory groove is extremely rare. We herein present 2 cases of schwannomas in the olfactory groove that were treated with endoscopic excision. In these 2 cases, the tumor originated in the cribriform plate and cerebrospinal fluid rhinorrhea occurred after tumor resection, which was repaired using tissue grafts.
Introduction
The paranasal sinuses and nasal cavity are uncommon sites of schwannomas, accounting for only 4% of all cases of head and neck schwannomas. 1 Approximately 50% of all nasal schwannomas occur in the nasal septum, followed by the middle turbinate and lateral nasal wall. 1 Common clinical presentations of nasal schwannomas include nasal obstruction and bleeding. Nasal schwannomas are diagnosed histologically and their primary treatment option is surgical excision. Available literature on isolated schwannomas in the olfactory groove is scarce as it is an extremely rare condition. 2
We herein describe 2 cases of isolated schwannomas located in the olfactory groove that were treated with endoscopic excision. During surgery, the tumor was found to originate from the cribriform plate, and cerebrospinal fluid rhinorrhea occurred after tumor resection, which was repaired using tissue grafts. Importantly, no tumor recurrence was found during follow-up. The institutional review board approved publication of this case report.
Case 1
A 55-year-old man presented with progressive left nasal obstruction 1 year ago, followed by a purulent nasal discharge on his left side, orbital distending pain, and epiphora. Medical history was otherwise unremarkable. Physical examination revealed a smooth-surfaced mass in the left nasal cavity that extended to the nasopharynx. Imaging confirmed that the ethmoid sinus and left nasal cavity were occupied with a tumor that extended laterally into the intraorbital and maxillary sinuses and posteriorly through the posterior nostril into the nasopharynx. Thus, obstructive inflammation was observed in the left frontal sinus, ethmoidal sinus, and sphenoid sinus. Head magnetic resonance imaging (MRI) with gadolinium contrast revealed a lesion of 5.9 × 2.6 × 4.8 cm in size that exhibited heterogenous enhancement and the mass presented as a local intracranial projection .In addition, computed tomography (CT) revealed thinning of the bone in the cribriform plate with absence of the local bone (Figure 1A-C). MRI and CT images. Cribriform plate thinning with absence of the local bone(arrow). The mass presented as a local intracranial projection (*). Magnetic resonance imaging (MRI), computed tomography (CT).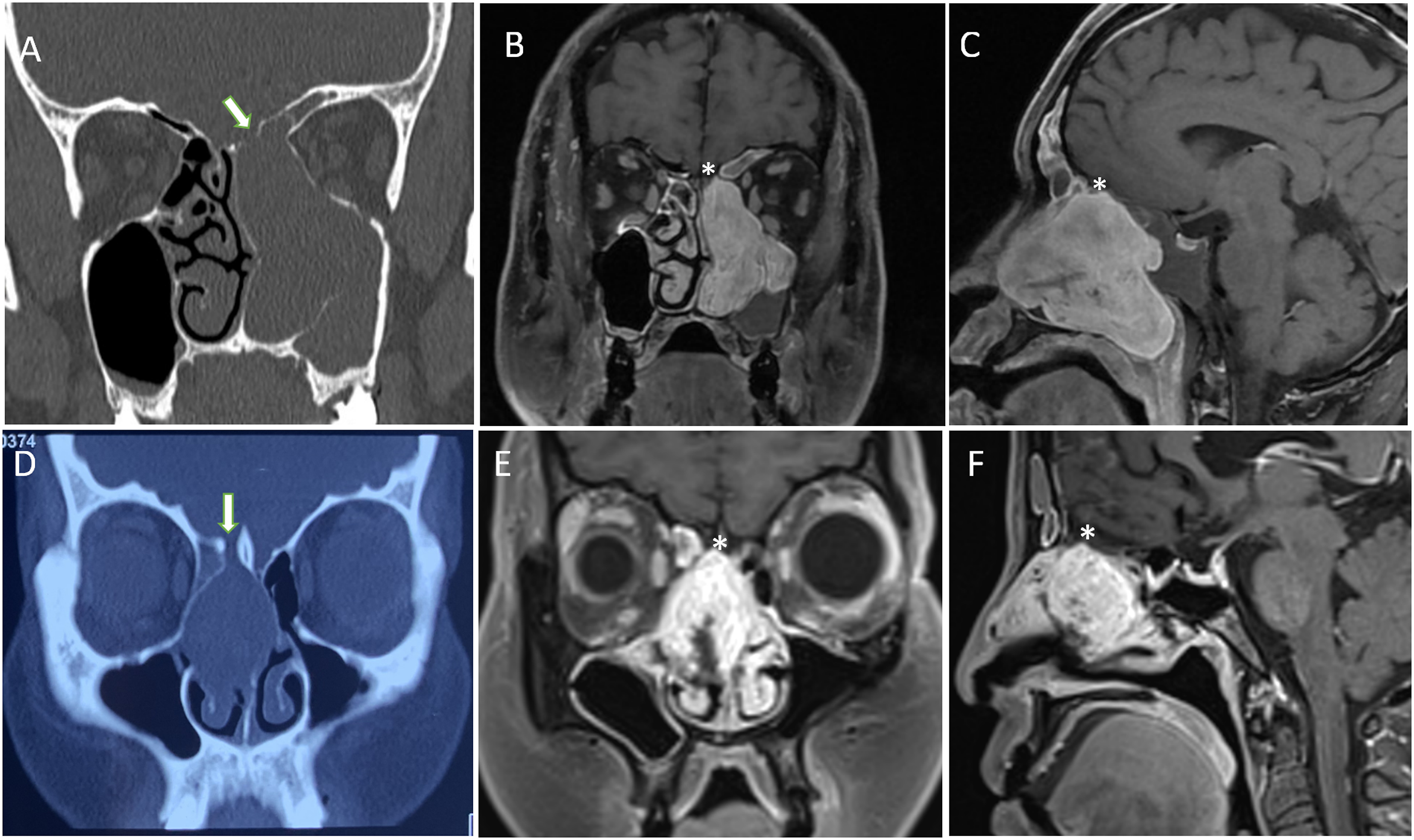
A nasal endoscopic approach under general anesthesia was used wherein the mass in the right nasal cavity was resected. As the tumor was large and had no obvious capsule, it was resected in blocks. During the procedure, a pedunculated mass that originated from the cribriform plate was observed but no nerve attachment was noted.
Cerebrospinal fluid leakage occurred after the removal of the radicular part of the mass, and the pedicled, vascularized mucosal flap of the nasal septum was repaired simultaneously. Pathological examination confirmed the lesion to be a schwannoma. No recurrence was observed during the follow-up period of 19 months, and the patient’s sense of smell remained unaffected.
Case 2
A 50-year-old woman experienced right nasal cavity obstruction, hyposmia, occasional ipsilateral hemorrhage, orbital swelling and pain, and nasal discharge for 4 months. She had undergone biopsy in an outpatient clinic, which had revealed a polyp. In addition, she had a 10-year history of hypothyroidism that was being treated with Levothyroxine sodium tablets.
Physical examination revealed a mass in the olfactory groove of the right nasal cavity. MRI revealed a mass in the right nasal cavity while contrast-enhanced CT revealed obvious heterogenous enhancement in a lesion measuring 2.5 × 2.6 × 3.3 cm, which presented as a local intracranial projection, along with right sinusitis. In addition, CT performed at another hospital revealed that the mass occupied the olfactory groove, that it displayed expansionary growth, and that there was partial bone loss in the right cribriform plate (Figure 1D-F).
During plasma resection of the tumor with nasal endoscopy, the tumor could not be adequately demarcated and no capsule was found, although a stalk anchored the lesion to the cribriform plate. A local dural defect and cerebrospinal fluid leakage occurred after tumor resection, and the free flap of the middle turbinate was used for defect repair (Figure 2). As in the previous case, no nerve attachment was seen during surgery. Intraoperative images. A. Cerebrospinal fluid leakage (arrow) occurred at the site of a partial defect in the cribriform plate when the tumor was removed and B. Middle turbinate free flap (arrow) was used for repair.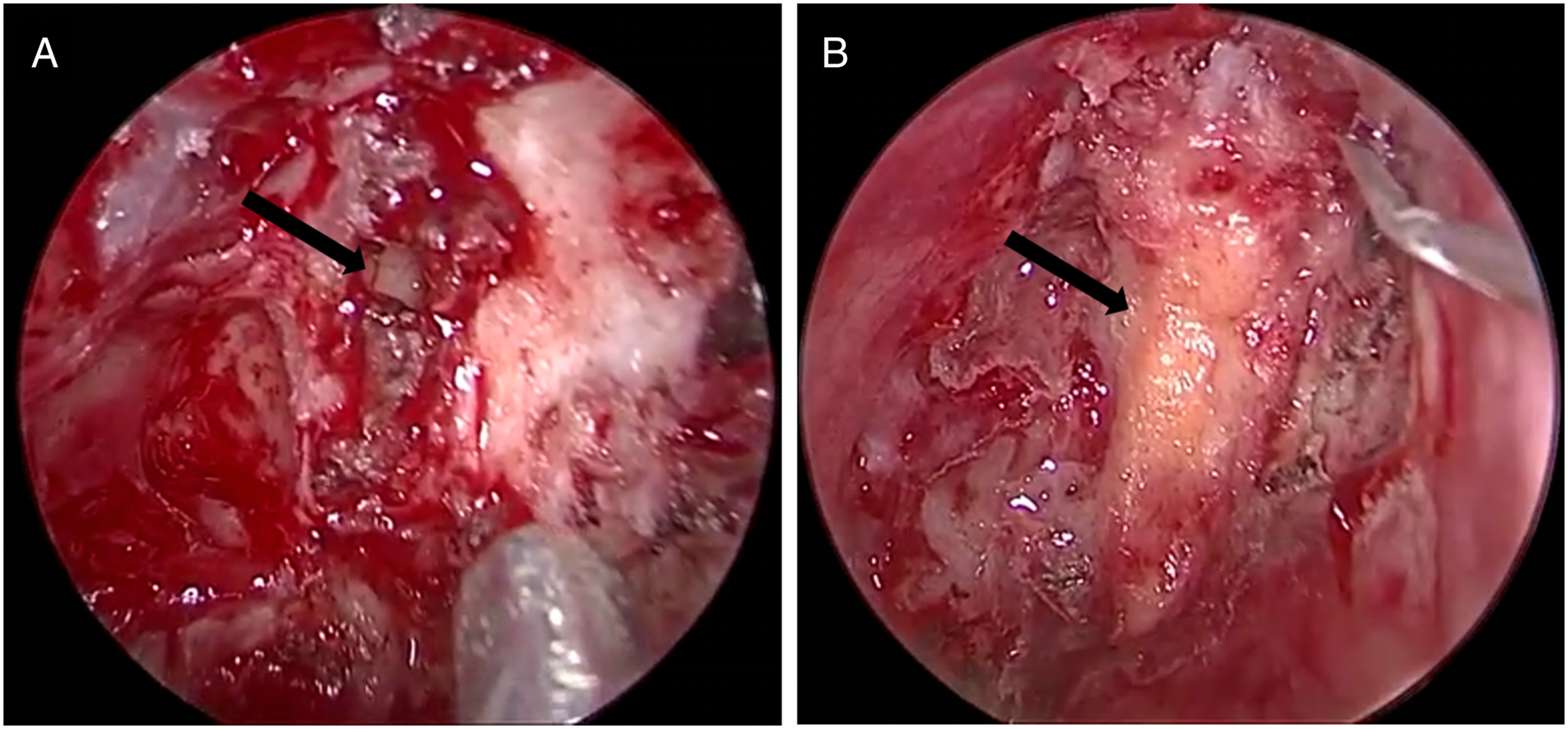
Postoperative pathology confirmed the lesion to be a schwannoma, and no recurrence was noted on CT 6 months after the procedure. However, no change in the patient’s anosmia was observed.
Discussion
Schwannomas are rare and benign tumors that grow at a slow rate. While they can occur at multiple sites in the neck and head, the most common site is the cranial nerve Ⅷ. 3 Available literature indicates that while schwannomas extend to the olfactory groove or paranasal sinuses, they are primarily located intracranially. Such lesions are called schwannomas of the anterior skull base, are often referred to as subfrontal or olfactory groove schwannomas, and commonly present with nasal and neurological symptoms. 4
Sinonasal schwannomas are rare, and those in the nasal cavity are mainly located in the nasal septum. 1 Thus, schwannomas of the olfactory groove that are located only in the nasal cavity are quite rare and can be typically distinguished from olfactory groove meningioma, hemangiopericytoma, esthesioneuroblastoma, and metastatic disease. 4
It is well known that determining the origin of nasal cavity tumors from imaging studies can be difficult, and as the nerves in the nasal cavity are slender, it is challenging to identify the neurogenic site of the tumor and origin of the schwannoma during surgery. 1 The origin site is defined as the location of the attachment of the tumor and identification of the origin site may be an useful method in clinical practice.
Here, we describe 2 cases of isolated schwannomas in the nasal cavity that were histologically confirmed. Notably, while there was no evidence of nerve attachment during surgery, careful observation of the images from both patients revealed compression and thinning of the cribriform plate with local bone defects. In particular, MRI revealed local intracranial protrusion of the tumor, suggesting that the origin of the tumor might be located near the cribriform plate of the olfactory groove.
Schwannomas originating in the olfactory groove are rare because the olfactory bulbs, as a part of the central nerve, are devoid of Schwann cells. Hence, descriptions of the origin of schwannomas of the olfactory groove remain uncertain. Among various hypotheses on the origin of these lesions, the most probable hypothesis is thought to be hyperplasia of the Schwann cell that occurs in the perivascular nerve plexus, fila olfactoria, or anterior ethmoidal nerves surrounding the sieve plate. Such hyperplasia of the Schwann cell is characterized by the formation of 0.5 mm Schwann cell sheath around the olfactory bulb, 5 and available literature deems the meningeal branch of the anterior or trigeminal ethmoid nerve to be the most probable site of origin of schwannomas. 2
Complete resection is the treatment strategy used for nasal schwannomas and an appropriate surgical approach is selected based on tumor location, size, and other factors. Importantly, there is generally no recurrence after surgery. 1 In both of our patients, we used a nasal endoscopic approach with plasma debulking followed by exposure of the tumor origin and complete resection as there was limited space for the olfactory cleft under endoscopic visualization. During surgery, cerebrospinal fluid leakage occurred at the site of the partial defect in the cribriform plate when the tumor was removed; hence, transnasal repair was simultaneously performed. No recurrence was observed during postoperative follow-up.
Conclusions
Schwannomas of the olfactory groove that are located only in the nasal cavity are very rare. The origin of tumor can be inferred by carefully observing the cribriform plate structure in the images acquired before surgery. Cerebrospinal fluid leakage after total resection is common and can be corrected by simultaneous transnasal repair. There was no recurrence after resection.
Footnotes
Authors’ contributions
Conception and design, CAP and WYZ; Data collection, LSY, LSF, and LQ; Writing -Original Draft, LSY, YL, and YP; Writing -Review & Editing, SL, SSJ, and CAP. And all authors read and approved the final version of the manuscript and ensure this is the case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Data availability
Data openly available in a public repository.