
Abstract
Patients with petrous bone cholesteatoma most commonly present with hearing loss and facial paralysis. Other clinical presentations can include otorrhea, tinnitus, aural fullness, otalgia, and dizziness. Here, we report a patient with petrous bone cholesteatoma who presented with cerebrospinal fluid rhinorrhea. This patient was initially misdiagnosed with rhinogenic cerebrospinal fluid leakage, and was finally diagnosed with the supralabyrinthine type of petrous bone cholesteatoma. During the surgical repair through the transmastoid trans-superior semicircular canal approach, the fistula was found in the superior wall of the internal auditory canal. He had satisfactory outcomes after the surgery, with no recurrent cerebrospinal fluid rhinorrhea.
Keywords
Introduction
Most patients with cerebrospinal fluid (CSF) rhinorrhea have CSF leakage into the nose through the fistula in the floor of the anterior cranial fossa. A small number of patients have the fistula in the temporal bone. After reaching the temporal bone, CSF can further flow into the nasal cavity through the Eustachian tube to present as rhinorrhea, which is called otogenic CSF rhinorrhea. The causes of the otogenic CSF rhinorrhea include temporal bone fracture, lateral skull base surgery, inner ear malformation, ectopic arachnoid granulations, meningocele, and temporal bone cholesteatoma. The fistula can be located in the middle cranial fossa, posterior cranial fossa, internal auditory canal, vestibule window, and round window.1,2 Here, we report a rare case of congenital petrous bone cholesteatoma with CSF rhinorrhea through a fistula in the internal auditory canal.
Case study
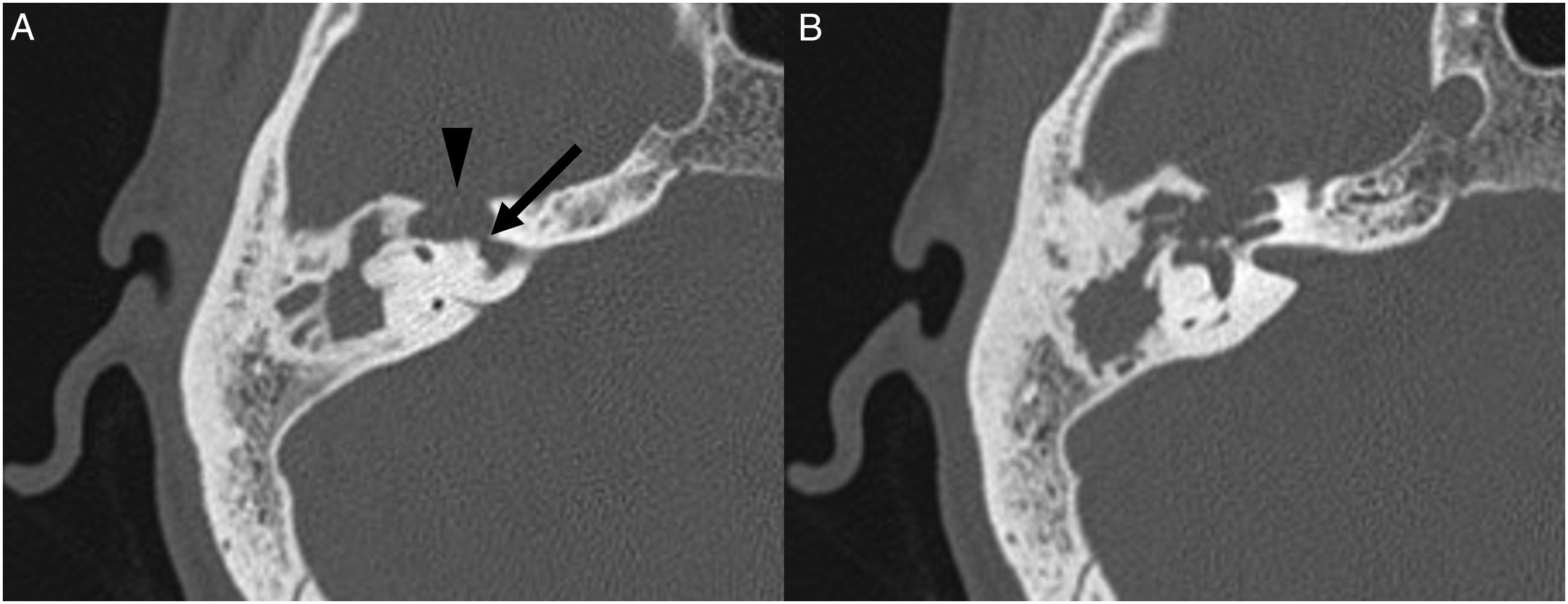
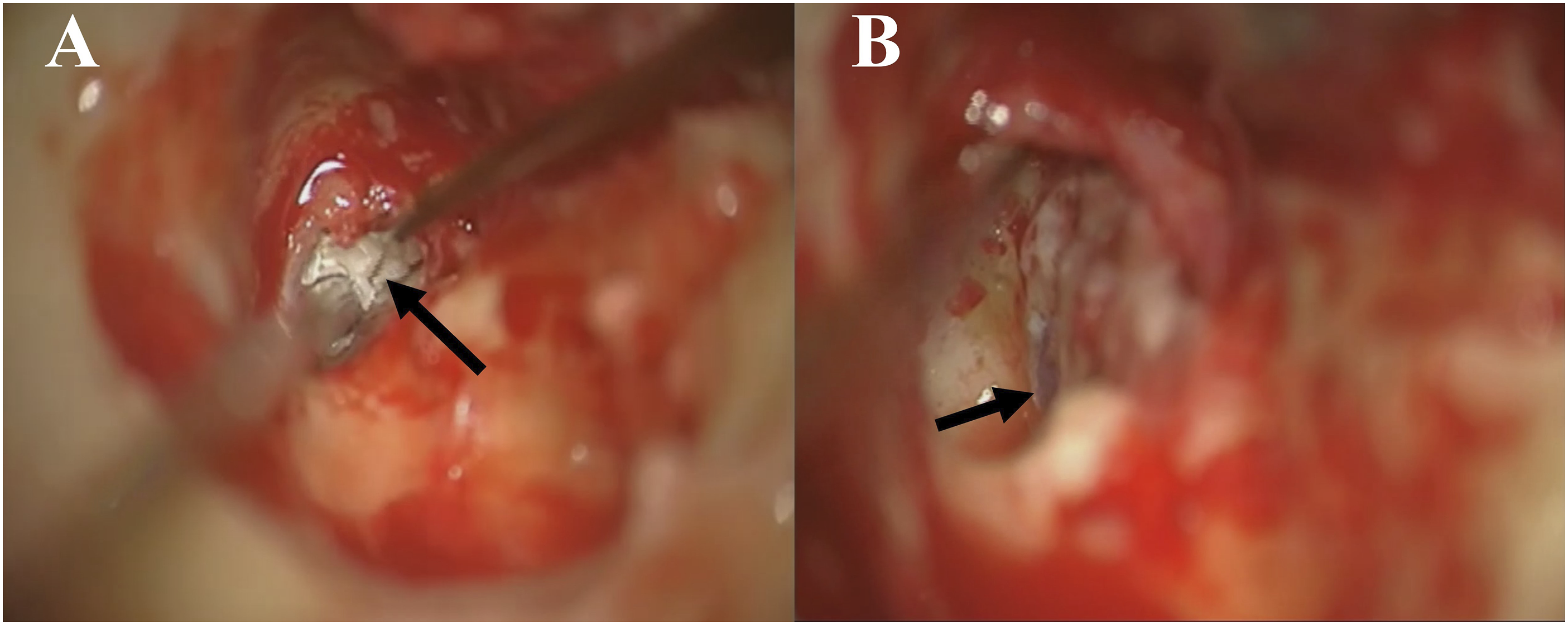
A 46-year-old male presented to the Department of Neurosurgery with clear right nasal drip, headache, and recurrent fever having lasted 20 days. The fever began immediately after head trauma. The patient was diagnosed as CSF rhinorrhea and was treated conservatively for 2 weeks without improvement. He then received the lumbar cistern drainage, but his symptoms persisted. On carefully reviewing the sinus computed tomography (CT) images, we found a bony defect in the right middle skull base with a soft tissue density shadow in the right temporal bone (Figure 1). Therefore, otogenic CSF rhinorrhea was considered. The patient was referred to the Department of Otolaryngology for further evaluation. The patient reported a 20-year history of hearing loss without otorrhea in the right ear, which was never treated. One year ago, he developed right-sided peripheral facial palsy and received acupuncture, but his symptoms did not resolve. He did not seek further examination or treatment. Otoscopic examination showed an intact right tympanic membrane. Through the tympanic membrane, a white mass was observed inside the tympanic cavity. Pure tone audiometry showed mixed hearing loss in the right ear. High-resolution CT of the temporal bone showed the densities of soft tissue in the right petrous bone, mastoid air cells, and tympanic cavity. There were bony defects in the right internal auditory canal and middle skull base, with bony destructions in the right vestibule and cochlea (Figure 2). Magnetic resonance imaging (MRI) scans showed a lesion with iso-intense T1-weighted and hyper-intense T2-weighted signals in the right temporal bone. Based on the clinical presentation and images, this patient was diagnosed with congenital petrous bone cholesteatoma of the right temporal bone with otogenic CSF rhinorrhea. The cholesteatoma was removed through the transmastoid trans-superior semicircular canal approach. During the operation, the cholesteatoma was found in the petrous part of the temporal bone, mastoid air cells, and tympanic cavity, with bony defects in the middle skull base and the superior wall of the internal auditory canal. There was no damage to the dura mater of the middle cranial fossa. The dura mater of the superior wall of the internal auditory canal was ruptured with CSF leakage (Figure 3). The dural defect in the internal auditory canal was repaired by the temporal muscle fascia. Abdominal fat was used to fill the surgical cavity. Postoperatively, the patient recovered uneventfully. No CSF leakage occurred during the 23-month follow-up period. (A) Sagittal CT scan showing no bony defect in the nasal skull base. (B) Coronal CT scan showing a bony defect in the right middle skull base with a soft tissue density shadow in the right temporal bone. (A) Bony defect in the right middle skull base (arrowhead) and internal auditory canal (arrow). (B) Bony defect in the right vestibule and cochlea. (A) Cholesteatoma locating in the petrous part of the temporal bone. (B) The dural defect in the superior wall of the internal auditory canal.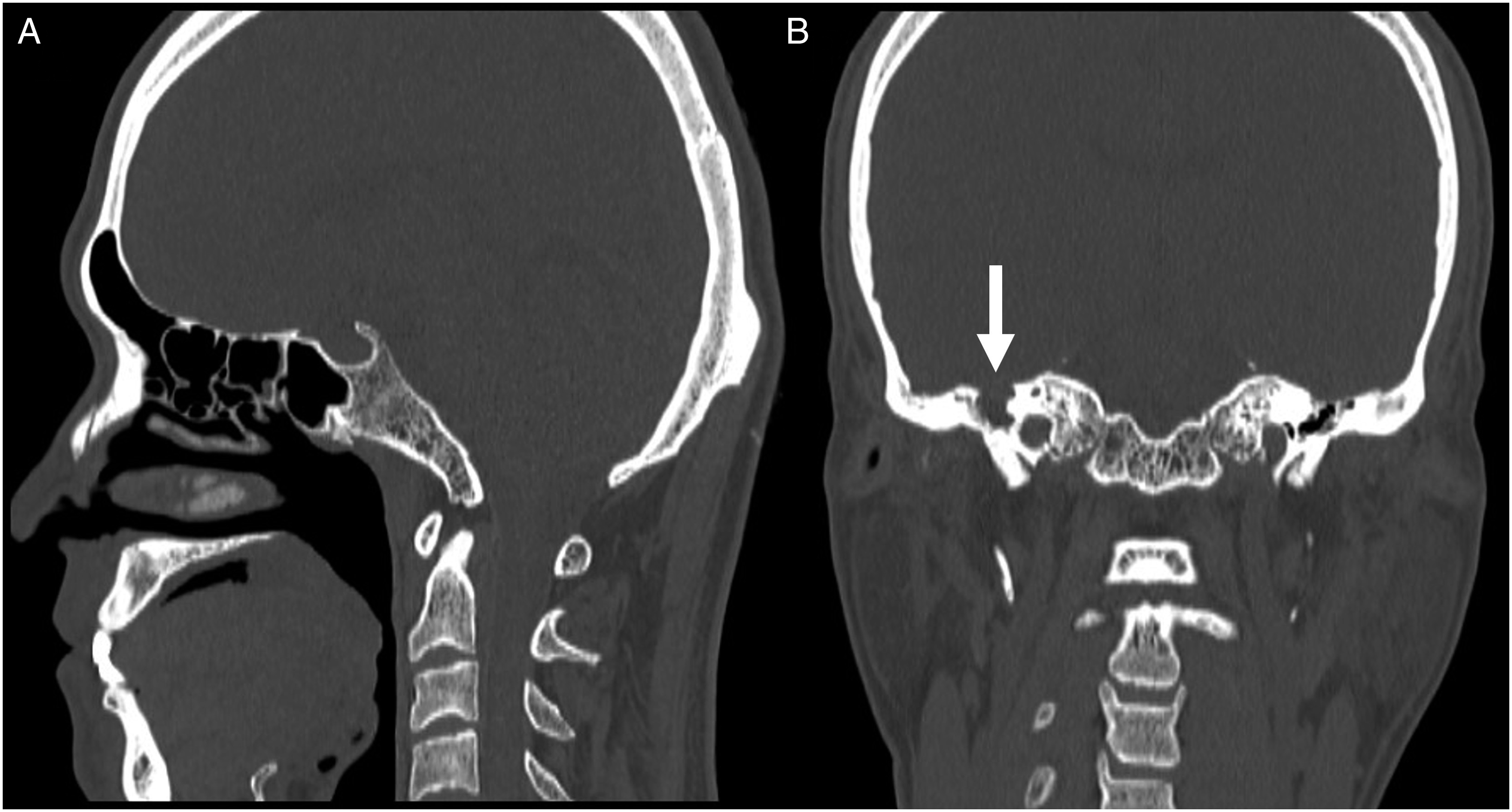
Discussion
Because otogenic CSF rhinorrhea is relatively rare, its diagnosis is challenging, and misdiagnosis and missed diagnosis are frequent. The possibility of otogenic CSF rhinorrhea should be ruled out in patients with CSF rhinorrhea and ear symptoms. Our patient was initially misdiagnosed with a CSF rhinorrhea through a fistula in the anterior base of the skull despite his history of hearing loss and peripheral facial palsy, and no bony defect was observed in the anterior skull base bone on the CT images. After careful review of the CT results, some destruction of the bone in the middle cranial fossa was identified. He was referred to ENT and finally diagnosed with CSF rhinorrhea secondary to a congenital petrous bone cholesteatoma.
Petrous bone cholesteatoma is an epidermoid cyst located in the petrous part of the temporal bone. It has been rarely reported in clinical settings, accounting for only 3.3% of temporal bone cholesteatomas. 3 Petrous bone cholesteatoma can be classified as congenital or secondary. Congenital petrous bone cholesteatoma is relatively rare and has been reported in 14–35% of patients with petrous bone cholesteatoma.3,4
Due to the deep location and slow growth of petrous bone cholesteatoma, affected patients usually have no readily visible clinical symptoms in the early stage. The most common clinical presentation is hearing loss, which is followed by facial paralysis. Other presentations include otorrhea, tinnitus, aural fullness, otalgia, and dizziness.4,5 Patients with congenital petrous bone cholesteatoma rarely have otorrhea since they usually have intact tympanic membranes.
Because of the close relationship between the petrous part of the temporal bone and the middle and posterior cranial fossae, petrous bone cholesteatoma can easily destroy bone at the base of the skull and cause meningeal adhesions. If the petrous bone cholesteatoma adheres tightly to the meninges, intraoperative removal of the cholesteatoma may tear the meninges and lead to the CSF leakage. Sanna et al 5 reported an incidence of intraoperative CSF leakage of 19%. However, petrous bone cholesteatoma with preoperative meningeal rupture and CSF rhinorrhea is very rare. After a thorough literature review, we identified only one previous patient with CSF rhinorrhea due to petrous bone cholesteatoma reported by Dzaman et al in 2015. 6 To the best of our knowledge, the present patient is the second case report of CSF rhinorrhea due to petrous bone cholesteatoma. Both the first case and our present case had congenital supralabyrinthine type petrous bone cholesteatomas based on the Sanna classification. 7 Supralabyrinthine petrous bone cholesteatomas can invade upward to affect the middle cranial fossa dura, expand inward to involve the internal ear canal, and move backward to compress the posterior cranial fossa dura. Approximately 14% of supralabyrinthine petrous bone cholesteatomas can affect the internal auditory canal. 8 The meninges of the internal auditory canal are relatively weak and tear easily. Senn et al 9 reported that 29% (6/21) of patients had intraoperative rupture of the meninges of the internal auditory canal with CSF leakage. Both the first case and our case involved the meninges of the middle cranial fossa and the internal auditory canal. During surgical exploration, the fistula responsible for CSF leakage was found in the internal auditory canal but not the middle cranial fossa. We believe that the cause of the preoperative CSF rhinorrhea in these 2 patients was tearing of the relatively weak meninges of the internal auditory canal from elevated intracranial pressure. The CSF entered the temporal bone and flowed into the nasal cavity via the Eustachian tube to present as CSF rhinorrhea.
In terms of the surgical approach, most patients with supralabyrinthine type of petrous bone cholesteatoma can be treated with subtotal petrosectomy. If there is any internal auditory canal involvement, a translabyrinthine approach can be selected. 3 If the patient has serviceable hearing and the lesion does not involve the inner ear, a cranial middle fossa approach with or without a transmastoid pathway is indicated to preserve the hearing. 10 In the case reported by Dzaman et al, the patient had profound hearing loss but still underwent the cranial middle fossa approach initially in order to determine whether the dura mater of the middle cranial fossa was damaged. This was followed by the transmastoid approach. In our present case, the patient had no serviceable hearing, and the lesion involved the inner ear and the internal auditory canal. Therefore, we selected the transmastoid trans-superior semicircular canal approach to explore both the middle cranial fossa and the internal auditory canal. We achieved a satisfactory treatment outcome.
Conclusions
CSF rhinorrhea caused by the petrous bone cholesteatoma is extremely rare. We selected the transmastoid trans-superior semicircular canal approach and achieved a satisfactory treatment outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.