
Abstract
Fibrous dysplasia (FD) is a rare benign disease that replaces a normal bone with abnormal fibrous and weak osseous tissue. It is usually detected in childhood and rarely occurs in old age. Although the disease is known to be caused by a genetic mutation, only a single case of FD secondary to surgery is reported in the literature. We report a case of monostotic FD of the maxillary sinus in a 70-year-old Asian woman who presented with incidental calcific lesion in the maxillary sinus on a brain computed tomography scan. At 32 months prior to presentation, the patient had undergone an endoscopic sinus surgery for a fungal ball of the same sinus. The lesion was removed by endoscopic surgery, and the histopathological evidence was consistent with FD. To the best of our knowledge, this is the second case of a postsurgical craniofacial FD, and a rare case that occurred in old age.
Introduction
Fibrous dysplasia (FD) is a slow progressing skeletal disorder, characterized by the replacement of normal bone and marrow by fibrous tissue and woven bone. FD is usually detected in children, expands during childhood and adolescence, and becomes quiescent by adulthood in most cases. It rarely occurs in the elderly.1-4
The etiology of abnormal growth in FD is known to be related to a mutation of the GNAS1 gene, which encodes the α subunit of a stimulatory G protein. However, the underlying pathophysiological mechanism remains still unclear.5,6 It has been suggested that trauma or infection might trigger the genetic mutation. 7 Despite its being a genetic disorder, only a single case of FD of the temporal bone secondary to ear surgery in a 16-year-old girl is reported in the literature. 8
Here, we report an extremely rare case of maxillary FD secondary to endoscopic sinus surgery in old age with literature review.
Case presentation
A 70-year-old Asian woman presented with dizziness, for which she underwent a brain computed tomography (CT) scan. A calcific shadow was incidentally detected in the right maxillary sinus. The patient was then referred to our hospital. Her history included an endoscopic sinus surgery for right maxillary fungal sinusitis at our hospital 32 months ago (Figure 1A and B). At that time, the surgical procedure went well without adverse events. The pathologic findings showed abundant septated hyphae with acute angles, which were emphasized by periodic acid Schiff (PAS) stain and Grocott methenamine silver (GMS) stain (Figure 1C and D). At 1-month follow-up, no sign of recurrence was noted. Radiology and pathology findings at the first surgery 32 months prior to recent presentation. Axial (A) and coronal (B) views of PNS CT showed soft tissue density with calcific shadow of right maxillary sinus. Histopathological examination showed abundant septated fungal hyphae with acute angles consistent with aspergillosis. (C) PAS stain (x400) and (D) GMS stain (x400). PNS CT, paranasal sinus computed tomography; PAS, Periodic Acid Schiff; GMS, Grocott methenamine silver.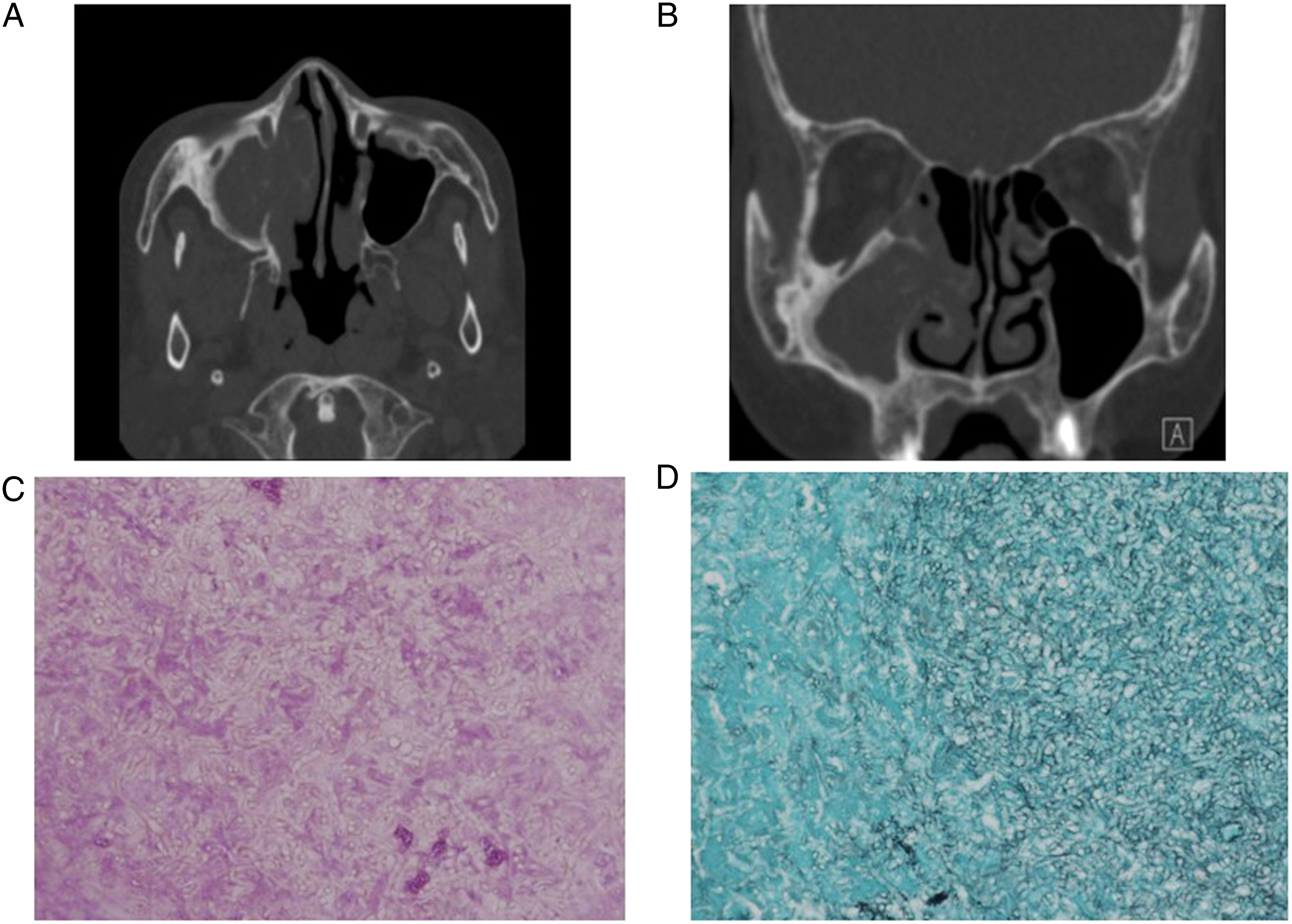
At her recent presentation, the patient had no sinusitis-associated symptoms such as facial pain, nasal stuffiness, rhinorrhea, or postnasal drip. The family histories and past histories were negative for diabetes, hypertension, endocrine disease, or facial trauma. On nasal endoscopic examination, no polyp, discharge, nor crust was found in the middle meatus. The widened natural ostium of the maxillary sinus was maintained, but the inside of the sinus was filled with tissue resembling fibrosis. A paranasal sinus (PNS) CT revealed a 22 X 15 mm sized inhomogeneous calcific lesion with soft tissue density in the right maxillary sinus (Figure 2A and B). Revision endoscopic sinus surgery was performed under the suspicion of recurrence of fungal sinusitis. In the operative finding, there was no evidence of fungal infection, but a large ossifying lesion with woven bone nature attached to the wall of the maxillary sinus was found. Middle and inferior meatal antrostomy were performed to remove as much lesion as possible. Histopathological examination showed irregularly structured bone trabeculae similar to Chinese characters in loosely arranged fibrous stroma without osteoblastic rimming (Figure 2C), which were consistent with FD. Postoperative recovery was uneventful, and no complaints were reported at follow-up after 9 months. Axial (A) and coronal (B) views of PNS CT at the time of revisit 32 months after the first surgery. Inhomogeneous calcific lesion sized 22 × 15 mm with soft tissue density was identified in the right maxillary sinus. PNS CT, paranasal sinus computed tomography. (C) Microscopic finding. Pathological examination showed irregular bony trabeculae in the background of loosely arranged fibrous stroma without osteoblastic rimming. These histological findings were indicative of fibrous dysplasia. Hematoxylin and eosin stain (x40).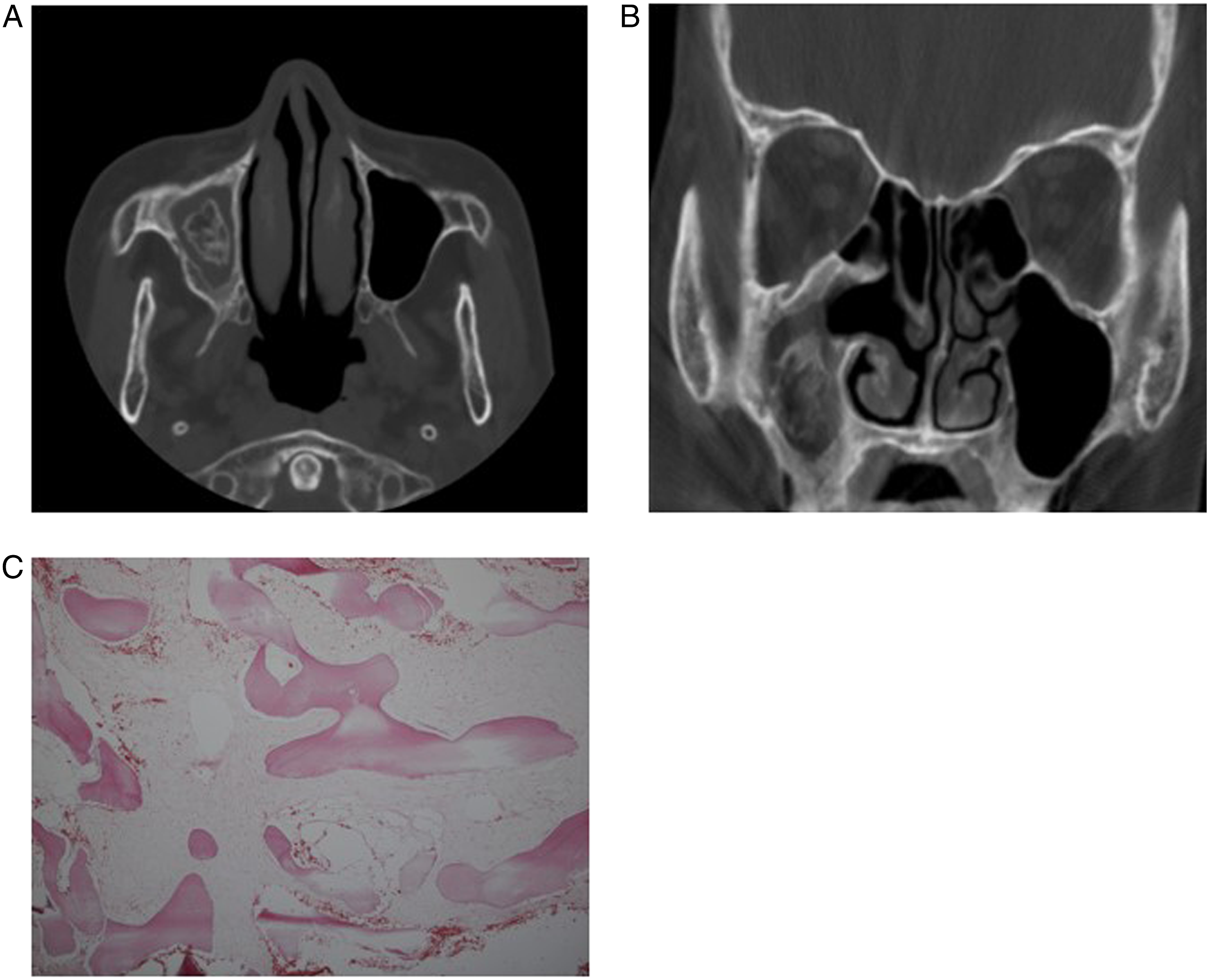
Discussion
FD was first described by Lichtenstein in 1938 9 and subsequently divided into several types in further studies. 10 Monostotic and polyostotic FD are distinguished by the number of affected sites, and polyostotic FD sometimes manifest in syndromes such as McCune-Albright syndrome, which affect the bones, skin, and several endocrine tissues, or Mazabraud's syndrome, characterized by single or multiple intramuscular myxomas with FD. 11 Any bone of the skeleton may be involved, but zygomatic-maxillary complex is one of the most commonly affected sites in monostotic craniofacial FD. 12
Underlying cause of FD is not fully understood. A mutation of the GNAS1 gene that encodes the α subunit of stimulatory G protein (Gsα) in chromosome 20 is associated with this disease. This mutation leads to increased formation of cyclic adenosine monophosphate (cAMP) involved in the differentiation of osteoblasts and the osteoblastic/osteoclastic bone turnover. Inappropriate osteoblastic differentiation contributes to the overproduction of a disorganized fibrotic bone matrix. Higher levels of cAMP also lead to increased levels of interleukin-6 (IL-6), which may be responsible for the osteoclastic bone resorption in FD. The increased expression of c-fos proto-oncogene seen in fibroblastic cells obtained from FD lesions may contribute in the pathogenesis of FD.5,11 However, the presence of any triggering factor that could contribute to this genetic mutation remains unknown. Schlumberger reported a case of monostotic temporal bone FD in 1946 and hypothesized that the monostotic form of the disorder could be caused by a disturbance of the normal reparative processes following bone injury. 7 After exhaustive literature review, we found only one case of postsurgical FD of the temporal bone in 16-year-old girl with a history of tympanoplasty at the age of 7 years, 8 and three cases of posttraumatic FD, which developed at the site of head trauma.6,13,14 Head trauma has not yet been proven to be associated with FD pathogenesis, but its relation with the upregulation of the c-fos gene in the bone has been described. Contrastingly, FD pathogenesis has been related to the increased expression of the c-fos gene. Therefore, FD may be induced by trauma, including surgical trauma, via a c-fos gene-mediated mechanism. 13
Vast majority of bone lesions are detectable within the first decade of life and do not develop after the age of 15 years. 2 Although most cases of monostotic FD are self-limiting and hamartomatous, some do not become dormant at the end of adolescence and may be activated or reactivated in adulthood in response to a life event, such as pregnancy. 4 Even though several cases of FD in elderly have been reported, most of them were slow growing over many years or quiescent stage lesions until middle age and manifested in old age, unlike in this case.3,4
The final diagnosis of FD is made through a biopsy. Histology shows irregularly shaped trabeculae of woven bone without osteoblastic rimming in a background of fibrous tissue. 13 Treatment is dependent on the patient’s age, the extent of disease, and the clinical behavior of the lesion. The FD lesions can be described as quiescent, non-aggressive, or aggressive. Patients with quiescent FD, lesions undergo observation with monitoring for changes consisting of clinical examination, patient photographs, sensory nerve testing, and periodic maxillofacial CT imaging. Patients with non-aggressive but active FD should wait until the lesion becomes quiescent and reach skeletal maturity to become eligible for surgery. Patients with aggressive and rapidly expanding FD must undergo immediate evaluation and biopsy prior to surgical management. Treatment may range from contour resection to en bloc resection depending on the diagnosis. Malignant transformation of FD has been reported in less than 1% of cases of FD.1,15
We experienced a case of FD of the maxillary sinus after endoscopic sinus surgery for fungal ball in an elderly patient. The absence of signs of FD in our patient’s first sinus surgery, as well as the typical pathological finding, suggest that this could be the rare case of FD secondary to sinus surgery.
Although the pathogenesis of FD is poorly understood, we suggest that surgical trauma might be a trigger factor for the development of this disease. Further studies should be performed to verify this postulation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional Review Board and Ethics Committee of Daegu Catholic University Medical Center (CR-22-129).
Informed consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Data availability statements
The datasets used in the current study are not publicly available since the medical records and data are the patient’s privacy, but are available from the corresponding author on reasonable request under the consent of the patient.