
Abstract
Introduction
Facial trauma is the most common cause of facial fractures with the 2 leading etiologies being assault and motor vehicle collision (MVC). MVC is the most common cause of panfacial trauma and assault is the most common cause of isolated facial fracture. 1 Other mechanisms include falls, sports-related injuries, occupational accidents, and gunshots. The most common fracture types are nasal bone fracture followed by orbital floor, zygomaticomaxillary complex, mandibular ramus, and nasoethmoid orbital complex. 2 Diagnosis and treatment of facial fractures typically require a multidisciplinary team, with initial clinical assessment done in the emergency department. After confirmatory imaging of a displaced fracture, surgical reconstruction is the gold standard to optimize functional outcomes and cosmetic deformities. 3
As in many trauma-induced pathologies, healing after surgery is affected by a patient’s nutritional status, especially in cases of polytrauma or mandibular fractures.4,5 Multiple studies, mostly in orthopedic surgery, have demonstrated the adverse effect of malnutrition on mortality rate, length of hospital stay, and return of function. 6 Enhanced recovery after surgery (ERAS) protocols are designed to accelerate recovery time after surgery and have been implemented across many surgical subspecialties. 7 These guidelines emphasize immediate/early return to oral nutritional intake post surgery to help recovery and decrease length of hospital stay. 7 Both facial fractures and subsequent treatment impair oral nutritional intake, leading to weight loss and suboptimal healing. This is especially true for fractures requiring closed reduction with maxillomandibular fixation (MMF), necessitating a liquid diet to avoid unnecessary stress at the fracture site. 4
Although the impact of nutritional status and weight loss has been studied in mandibular fractures, 8 other types of facial fractures and their treatments have remained largely neglected. Furthermore, the clinical impact of weight loss on objective recovery has not been reported in recent literature. Not only is it unclear how much weight patients tend to lose after facial surgery following facial trauma, but whether the resulting malnutrition or lack of energy affects postoperative outcomes has also been overlooked. This study seeks to evaluate the impact of the type of surgical reconstruction after facial trauma on postoperative weight loss.
Patients and Methods
Setting and Patient Identification
This study was approved by the University of Cincinnati (UC) College of Medicine Institutional Review Board (MOD02_2021-0808). A retrospective, single-center, chart review of the electronic medical record (EPIC) at UC Health was performed to build the database. From February 2019 to September 2021, patients with facial fractures that required surgical intervention were included (Supplemental Appendix 1). Additional inclusion criteria included age greater than 18 years, at least one fracture requiring surgical management, and a complete operative note and anesthesia report available in the electronic medical record. Cases that involved head and neck cancer diagnoses, pathological fractures, an incomplete anesthesia report, or surgery at an outside institution were excluded.
Diagnoses and procedural codes for multiple facial traumas included, but were not limited to, mandibular fractures (condyle, angle, body, ramus, coronoid, parasymphysis), midface fractures (zygomaticomaxillary complex, nasal bone, nasoorbitoethmoidal, maxillary sinus, LeFort I-III), and orbital fractures (floor, wall) to isolate which patients to include. Patients with multiple different types of fractures were counted once in each applicable category. Demographic factors and medical history were collected from the hospital’s electronic medical records. Trauma laboratory values for hemoglobin, ferritin, thyroid-stimulating hormone (TSH), albumin, and prealbumin were obtained before and after trauma. Prior routine laboratory values were allowed to be used for pre-trauma values if collected within 6 months to a year from trauma, and post-trauma values were the first set of laboratory values found after surgery and before the first follow-up visit.
Trauma Characteristics and Clinical Outcomes
Traumas were grouped by location, which included subunits of bony involvement, and mechanism of injury. Locations were divided into the following categories: forehead, mandible, orbit, and midface. Forehead fractures were subdivided into anterior and posterior table. Mandible fractures were subdivided into condyle, angle, body, ramus, coronoid, and parasymphysis, and indications were made for sidedness, open versus close, simple versus comminuted, or changes in occlusion. Midface fractures were subdivided into zygomaticomaxillary complex, nasal bone ± obstruction, nasoorbitoethmoidal complex, maxillary sinus, and LeFort I to III. Orbital fractures were subdivided into floor, wall, and whether there were acute ophthalmologic concerns at the time of presentation, such as intraconic hematoma, globe injury, or blindness. Neurosurgery involvement, if any, was indicated. Dental avulsion during trauma or required extraction was recorded. Mechanisms of injury included motor vehicle crash, motorcycle crash, bicycle or pedestrian versus vehicle, assault/nonballistic weapon/fight, gunshot wound (GSW), or accident/organic fall.
The weights of the patients were assessed before surgery and at 1, 2, and 3 month follow-up in the otolaryngology clinic. Presurgery weight was often collected on presentation to the emergency department. If not reported at that time, most recent weight was used if recorded within 6 months of trauma. Patients who sustained polytrauma and required admission to the intensive care unit (ICU) were further analyzed for the length of ICU stay, type of nutrition while in the ICU [nasogastric tube (NGT)], days with breathing devices or tracheostomy, duration of tube feeds, and last ICU weight.
We recorded surgical reconstruction approaches and noted patients who required MMF or the placement of a NGT. Different repair techniques for the following: osteotomies, bone grafts, forehead advancement and plating, percutaneous treatment of malar tripod or zygomatic arch, closed nasal bone fracture reduction, open treatment orbital floor fracture, complex treatment of frontal sinus fracture, or intraoral approaches were tracked. Specifically, mandible open reduction internal fixation (ORIFs) were specified as endoscopic approach or retromandibular incision. Postoperative diet was recorded, and indicated if patients were lost to follow-up, noncompliant, or had surgical complications. Complications were grouped into the following categories: infection, abnormal occlusion, persistent pain, nonunion or persistent bone mobility, persistent nasal obstruction, loss of vision or diplopia, cerebrospinal fluid leak, significant cosmetic concern, exposed hardware, or need for revision surgery.
Statistical Analysis
Anonymous data were transferred from the Health Insurance Portability and Accountability Act (HIPAA)-compliant REDCap database into a Microsoft Excel spreadsheet with anonymized demographic variables. Standard descriptive statistics were reported. Univariate comparison between the groups with and without MMF, with and without masseteric space involvement, with and without complications, were performed using the Fisher exact test for categorical variables and Wilcoxon rank sum test for nonparametric continuous variables. The multivariate logistic regression model was built to incorporate variables that were significant on univariate analysis, and other variables that appeared medically relevant based on literature review. Where multivariable regressions were performed, covariates were explicitly specified. Results were considered statistically significant when P value was <.05. Statistical analysis was performed using JASP (Version 0.16.2; SAS Institute Inc., 1989-2021).
Results
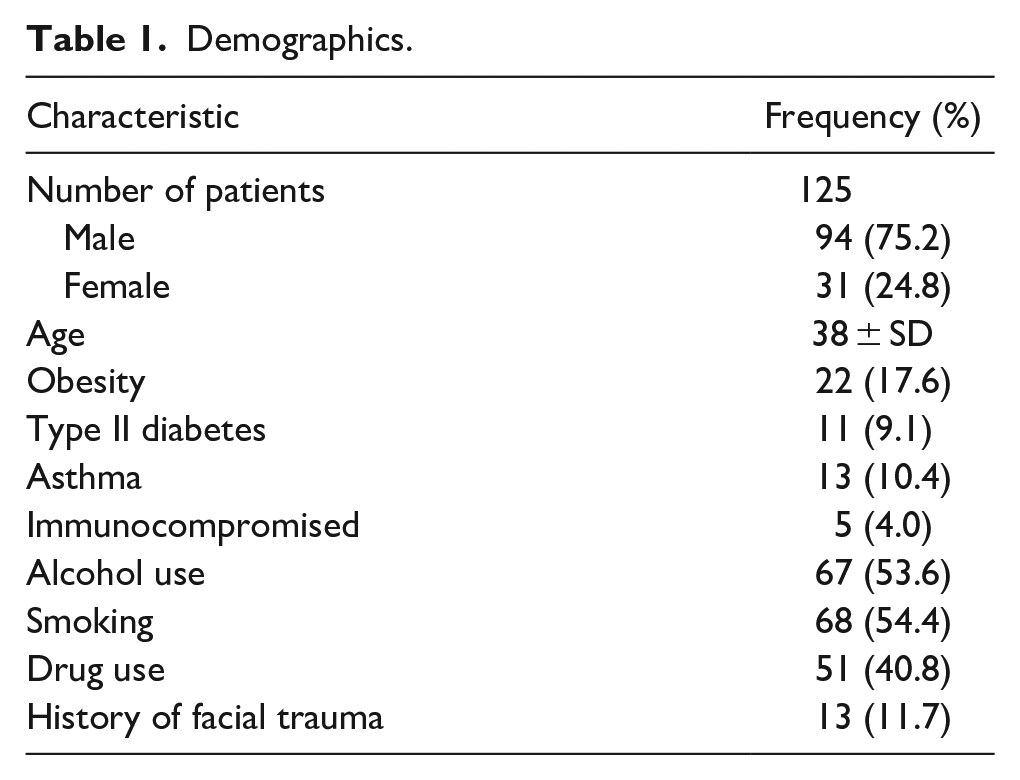
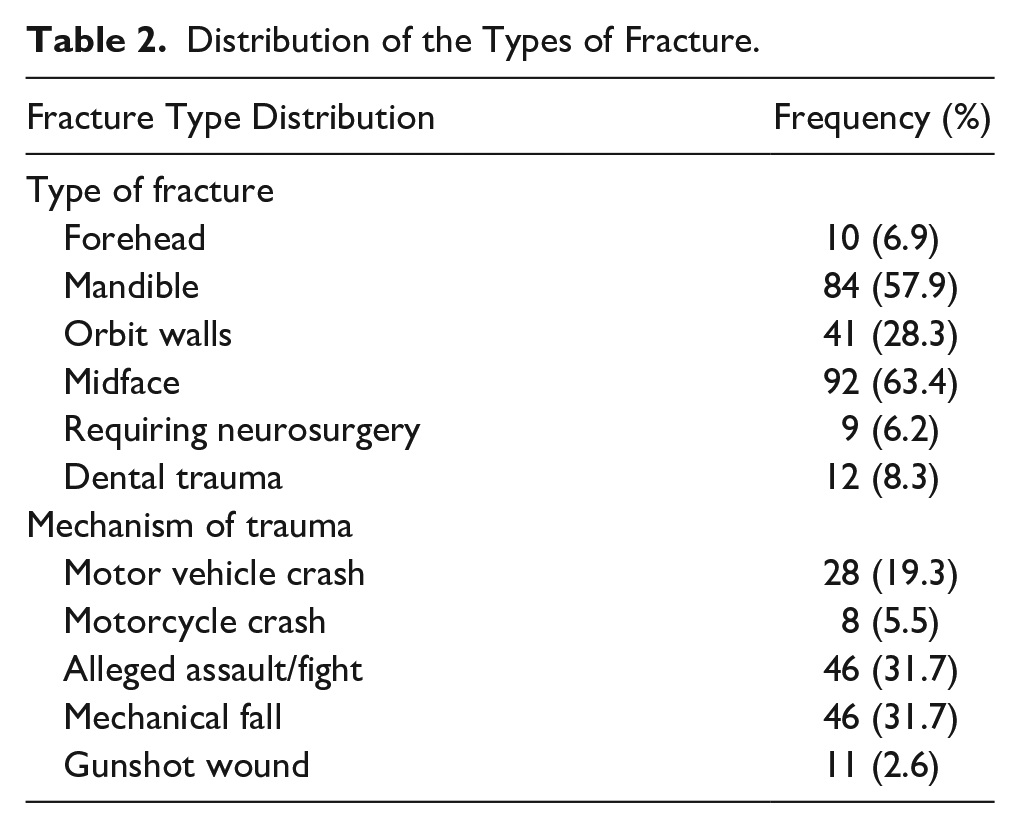
We identified 155 patients between February 2019 and September 2021 who had facial fracture surgical reconstruction. One hundred forty-five patients met inclusion criteria with 10 patients excluded due to facial fractures and reconstruction secondary to oral cavity cancer. Patient characteristics are summarized in Table 1. Location of fractures and mechanism of injuries are summarized in Table 2. Our population included more men (n = 110, 75.9%) than women (n = 34, 23.4%). Most patients were single (n = 91, 62.8%), others were married (n = 28, 19.3%), divorced (n = 13, 9.0%), or had a domestic partner (n = 7, 4.8%). Mean age at presentation was 38 years ± SD (42.3 years in women, and 37.2 years in men). Active tobacco smoking (n = 75, 52.8%), daily alcohol use (n = 79, 55.6%), and drug abuse (n = 59, 42.1%) were common. The comorbidities for our patient population are reported in Table 2. Among them, 66.7% (n = 10) required surgical reconstruction, 3.1% had chronic abnormal occlusion (n = 4), and 4.6% had poor dental hygiene (n = 6). The most common mechanisms of injury were reported assault (n = 46, 31.7%) and mechanical fall/accidental trauma (n = 46, 31.7%) followed by motor vehicle crash (n = 28, 19.3), gunshot wound (n = 11, 7.6%), motorcycle crash, and all-terrain vehicle accident (n = 8, 5.5%). The most common type of fracture among the 145 included patients was midface fracture (n = 92, 63.4%), which included isolated ZMC and maxillary fractures. This was followed by fractures of the mandible (n = 84, 57.9%) or orbital wall (n = 41, 28.30%). Frontal sinus fractures were the least common (n = 10, 6.90%).
Demographics.
Distribution of the Types of Fracture.
On average, patients lost 3.2 ± 4.9 kg (95% confidence interval = 2.7-4.1, P < .0001). When comparing location of facial fracture (mandible vs midface vs upper face), mandibular fracture was the only type associated with significant difference in weight loss. Patients with mandibular fracture lost an average of 4.8 kg (SD 5.4) compared to the 4.0 kg (SD 4.1) lost in patients without mandibular fracture (P = .0406). In comparison, patients with midface fracture lost an average of 3.4 kg (SD 4.5) while patients without midface fracture lost an average of 3.0 kg (SD 5.8, P = .6894). Patients with fracture of the upper face lost an average of 4.3 kg (SD 5.4) while patients without upper face fracture lost an average of 2.8 kg (SD 4.7, P = .1204).
Maximum amount of weight was lost between time of surgery and first follow-up appointment 1 month later. Most patients reestablished their presurgical weight at the third follow-up visit (3 months after surgery) regardless of fracture type. In univariate analysis, we found that admission to the ICU (5.9 kg, SD 5.4, P = .001), NGT placement (5.1 kg, SD 4.6, P = .012), and MMF (4.4 kg, SD 5.4, P < .0001) were risk factors associated with increased weight loss. In multivariate analysis, only MMF remained a significant risk factor for severe weight loss (2.7 kg, SD 0.9, P = .0024). Patients with dental trauma at time of surgery also lost more weight (1.4 kg, P = .001) at each follow-up visit compared to patients without dental trauma, regardless of fracture type.
There was no significant impact on severity of weight loss from age, mechanism of trauma, type of fracture, or type of surgery except for MMF. There was no relationship between degree of weight loss and frequency of complications. No specific correlation was established between the number of days spent in the ICU or number of days spent with feeding tube and weight loss.
Conclusion
Our work highlights the importance of nutrition for patients who require ICU care due to severe polytrauma or facial trauma and patients who require MMF for mandibular fractures. We reported the following: (1) factors such as ICU stay, NGT placement, and MMF are associated with severe weight loss; (2) patients experience an average loss of 3.2 kg between trauma and their first follow-up visit; and (3) patients regain most of the weight by 3 months after surgery. While it is unsurprising that patients experience weight loss after surgery, what is notable in our study are the risk factors that are associated with weight loss—especially MMF for mandibular fractures, as it requires wiring the jaw shut to allow for stability during the healing process.
Historically, the effects of facial reconstruction on weight loss have been studied most extensively in mandibular fractures. A retrospective cohort study conducted by Christensen et al found that mandibular fractures and their treatments were associated with almost 5% weight loss with no significant differences between open and closed reductions, resulting both from direct functional impairment of mastication and likely from postoperative pain. 4 A subsequent prospective study also conducted by Christensen et al supported these findings, demonstrating an average percentage weight loss of 4.1% over the course of mandibular fracture treatment. Interestingly, this study did not demonstrate a change in biochemical markers of nutritional status. 6 In patients with isolated mandible fractures that required a soft diet after surgery, perioperative nutrition counseling by a registered dietitian was associated with a decrease in postoperative complications although it did not affect weight loss.8,9
We analyzed all facial fractures to assess whether midface surgery could affect weight loss, secondarily to masseteric contraction and difficulty chewing, persistent pain, or low appetite in the perioperative setting. In non-ICU patients, only MMF was associated with postoperative weight loss. Patients regaining weight within 3 months after surgery is attributable to improved ease of mastication and oral intake as they heal. Furthermore, patients with MMF usually have hardware removed after 1 month, allowing them to regain eating function. Those who had avulsions or other dental injuries had more weight loss than their counterparts, likely due to increased dental trauma.
Frontal sinus fractures tend to be associated with greater weight loss; however, only a few patients had that type of fracture which limited statistical analysis. Two patients required neurosurgical intervention and lost more than 3 times the average weight loss due to severe polytrauma, multiple surgical interventions, and prolonged hospital stay, including NGT, tracheostomy placement, and ultimately delayed per os intake. Patients with facial fractures resulting from high-impact trauma, such as frontal sinus fractures, can present with other fractures and are more likely to need acute care and surgery, losing more weight.
Yao et al describe the wound healing process and the impact of local inflammation, infection, hyperglycemia, or active tobacco smoking on the recovery process.10-12 The authors did not demonstrate a statistical impact of age, tobacco, drug abuse, or diabetes on postoperative weight loss and frequency of complications in their patients.13-16 This can be explained by a young population of patients with fewer overall comorbidities than the general population. Meaningful nutritional data, such as albumin, ferritin, or TSH, proved difficult to collect because these variables were not systematically assessed in the emergency room for this population. Due to lack of consistent recording, the authors were not able to analyze impact of facial fracture surgery on nutritional laboratory values.
Our study was conducted before discussing whether the authors would like to implement a specific postsurgery protocol, including nutrition consultation and a dedicated meal plan. 17 It is debatable whether a weight loss of 3.2 kg is considered clinically significant and requires prophylactic intervention. As most of the patients regained their weight 3 months after their surgery and considering the generally young age of the population, the authors do not believe that a 3.2 kg weight loss significantly affects outcomes. Proper counseling after surgery and ordering liquid dietary supplements (current protocol) is effective within the first 2 to 3 months after surgery to help prevent further weight loss and malnutrition. However, an argument could be made that during the critical window immediately after surgery, nutrition and weight maintenance are important with nutritional supplements starting immediately. Especially considering populations that stay in long-term health facilities that have a higher prevalence of poor nutritional status,18,19 there are reasons to believe deconditioned patients who may be prone to mechanical falls are a particular subset that may benefit from such changes.
Our results should be interpreted in the context of the limitations of the study, many of which are inherent to a single-institution retrospective analysis. A future multicenter analysis may provide more power and external validity. Moreover, a prospective analysis of the patient population who presents with facial trauma to the emergency department is challenging and associated with frequent loss to follow-up. In this study, patients lost to follow-up were considered both as a result and limitation since the missing data affects the overall power of the results. There is merit in investigating whether malnourished patients before trauma, such as immunocompromised status, liver disease, or even recent surgery, are prone to poorer outcomes. Nutritionally enhancing these patients before performing facial fracture repair, if such wait is permissive, as a prospective study may be worthwhile as prophylactic measures to optimize nutritional status may help maintain neutral weight and wound healing.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241241114 – Supplemental material for The Impact of the Post-Traumatic Facial Reconstruction on Postoperative Weight Loss
Supplemental material, sj-docx-1-ear-10.1177_01455613241241114 for The Impact of the Post-Traumatic Facial Reconstruction on Postoperative Weight Loss by Isabelle Gengler, Susie Min, Megan Jiang, Grace Zhang, Mekibib Altaye, Thomas Radulesco, Jerome R. Lechien and Tsung-Yen Hsieh in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.