
Abstract
Objectives
Deep neck infections (DNIs) are a common and intractable disease encountered in ENT clinics that impose a significant medical and financial burden on affected individuals and their families. However, insufficient data are currently available for predicting outcomes in cases of DNI. The present study thus sought to develop a novel model capable of predicting treatment outcomes of DNI patients just using indicators at the visit.
Methods
Patients with DNIs treated from 2010 to 2022 were included in the present study. Patient data were retrospectively collected from medical records. Risk factors associated with mortality were identified using logistic regression models. A predictive model was constructed based on odds ratios for factors calculated using a multivariate regression model.
Results
In total, 153 patients were enrolled in the present study. Risk factors associated with mortality included age >50 years, residence in a rural area, dyspnea at visit, the involvement of multiple infected sites, serum albumin<34 g/L, renal insufficiency, mediastinitis, pulmonary infection, and septic shock. A multivariate regression model revealed that mediastinitis (OR: 7.308, P < 0.001), serum creatinine>95 μmol/L (OR: 23.363, P < 0.05), and serum albumin<34 g/L (OR: 13.837, P < 0.05) were independent predictors of mortality in deep neck infection patients, with serum creatinine>95 μmol/L being particularly critical to the outcomes. Diabetes was not the predictor of mortality but was associated with long-term hospitalization (P < 0.001).
Conclusions
In summary, the model constructed in the present study was capable of estimating the potential for poor outcomes in DNI patients before the initiation of treatment. These findings may help improve doctor–patient communication, especially for those struggling financially.
Introduction
Deep neck infections (DNIs) refer to cellulitis or abscesses that develop in the deep cervical fascial space. These infections are commonly encountered in ENT clinical practice and can arise from progressive infections of the tonsils, odontogenic structures, pharynx, esophagus, trachea, or salivary glands. The neck contains several cavities and fascial recesses, including the retropharyngeal, peritonsillar, masseteric, pterygopalatine maxillary, parapharyngeal, and submandibular spaces, all of which are interconnected and filled with soft connective tissue, adipose tissue, muscles, blood vessels, and nerves. DNIs can spread to several of these tissue sites along interconnected soft tissues, potentially resulting in severe symptoms and poor health outcomes. Common presenting symptoms in DNI patients include odontalgia/pharyngalgia/cervicodynia, fever, dyspnea, restricted mouth opening, and the presence of a cervical mass.
Deep neck infections have the potential to induce serious complications. For example, infections involving the pre-tracheal, retropharyngeal, or parapharyngeal spaces can compress the airway and cause respiratory tract obstruction. Moreover, when infections spread downward into the mediastinum, which is also filled with soft connective tissue, mediastinitis can result, causing chest pain and fever. Descending necrotizing mediastinitis, which is often a consequence of the downward spread of deep neck infections, can result in high mortality rates of 10–30%.1-3 When these infections continue progressing, pericarditis and empyema may result, and bacterial toxins can enter the bloodstream, potentially causing life-threatening septicemia and multiple organ failure.
The rapid onset and progression of DNIs and their potential for high morbidity and mortality rates can impose significant physical, psychological, and economic burdens on affected patients and their families, in addition to placing a substantial financial burden on the government as a whole 4 . Prior evidence suggests that the duration of hospitalization for DNIs is generally approximately 2 weeks,5,6 with the exact duration being dependent upon whether complications develop and whether the infection involves multiple spaces within the neck,5,7 although these findings are not universal. 8 Overall DNI mortality rates range from 0 to 2.7%,4,9,10 with death often coinciding with the presence of significant co-morbidities. However, few studies have explored the prediction model for mortality before the treatment.
The potential for mortality may be an important consideration for patient decision-making. The present study was thus designed to construct a model capable of predicting the poor outcomes before treatment in patients with DNIs to promote better communication between doctors and patients in daily clinical practice.
Patients and methods
Study participants and ethical approval
The medical records of 198 DNI patients were examined between 2010 and 2022 in the Otorhinolaryngology Department of the first affiliated hospital of Anhui Medical University for the current retrospective analysis. Those patients diagnosed with cervical abscess/cellulitis were included in this study. Patients were excluded from these analyses when sufficient data were not available. The First Affiliated Hospital Ethics Committee of Anhui Medical University approved this study. Figure 1 outlines the general study design in detail. Enrollment, data collection, risk factor screening, and model construction approaches.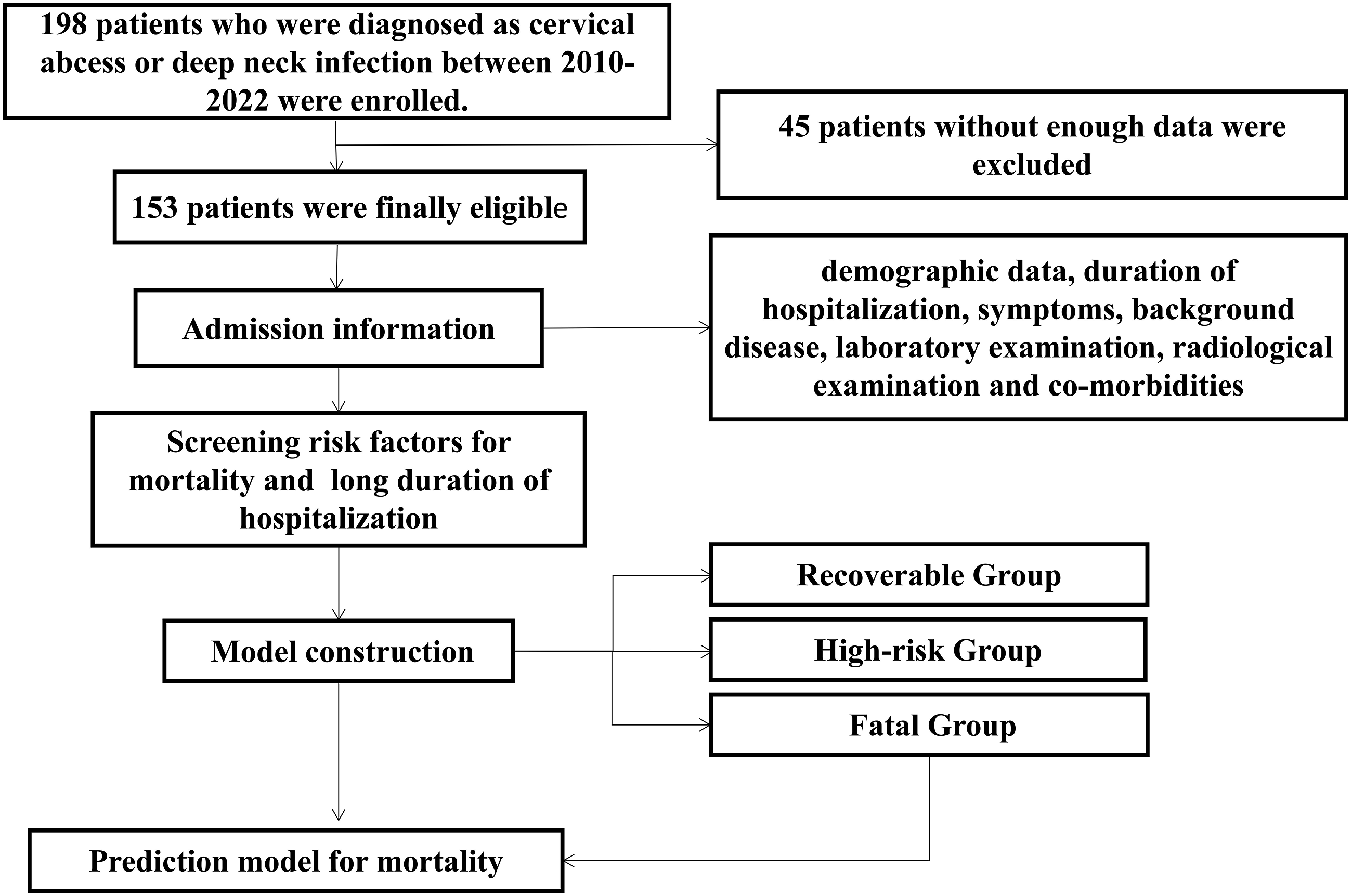
Of the 198 evaluated patients, 153 were enrolled in the final study, 48 were ruled out because insufficient data. Treatment approaches (pharmaceutical intervention, drainage, tracheotomy, etc.) were based on clinical findings. Variables extracted from patient medical records included demographic information, hospitalization duration, symptoms, laboratory examinations, radiological examinations, and co-morbidities corresponding to patient condition at presentation.
Statistical analysis
Continuous variables are given as means with standard deviations when normally distributed or medians with interquartile ranges when not normally distributed and were compared via Mann–Whitney U-tests. Categorical variables are given as frequencies with percentages and were compared via X2 tests.
Logistic regression models were utilized to explore the relationship between risk factors and mortality, with odds ratios (ORs) and 95% confidence intervals (CIs) calculated for each variable. Those significant risk factors in univariate logistic regression analyses were then incorporated into multivariate logistic regression models, with stepwise regression being used to filter out significant factors and adjusted ORs being calculated accordingly. Receiver operating characteristic (ROC) curves were then constructed and used to identify optimal cutoff points associated with predictors of high treatment costs. Area under the curve (AUC) values were additionally calculated for each predictor. Cutoff values for continuous variables were selected based on the maximal AUC. Model calibration was performed with the Nagelkerke R2. A P-value of < 0.05 was the significance threshold for this study, and all statistical analyses were conducted using SPSS 20.0 (IBM, NY, USA).
Results
Patient characteristics
In total, 153 patients (87 male, 66 female) were enrolled in this retrospective study, with a median age of 48.0 years (range: 1–89 years). The mean duration of hospitalization for these patients was 17 days, the mean white blood cell count in the overall patient population was 14.5 ± 1.1×103 cells/mm3, and the mean neutrophil ratio was 79.1 ± 2.4%. The mean serum creatinine was 72.0 ± 14.6 μmol/L, and the mean serum albumin (ALB) was 37.0 ± 2.5 g/L.
Demographics of deep neck infection patients at the time of clinical presentation.
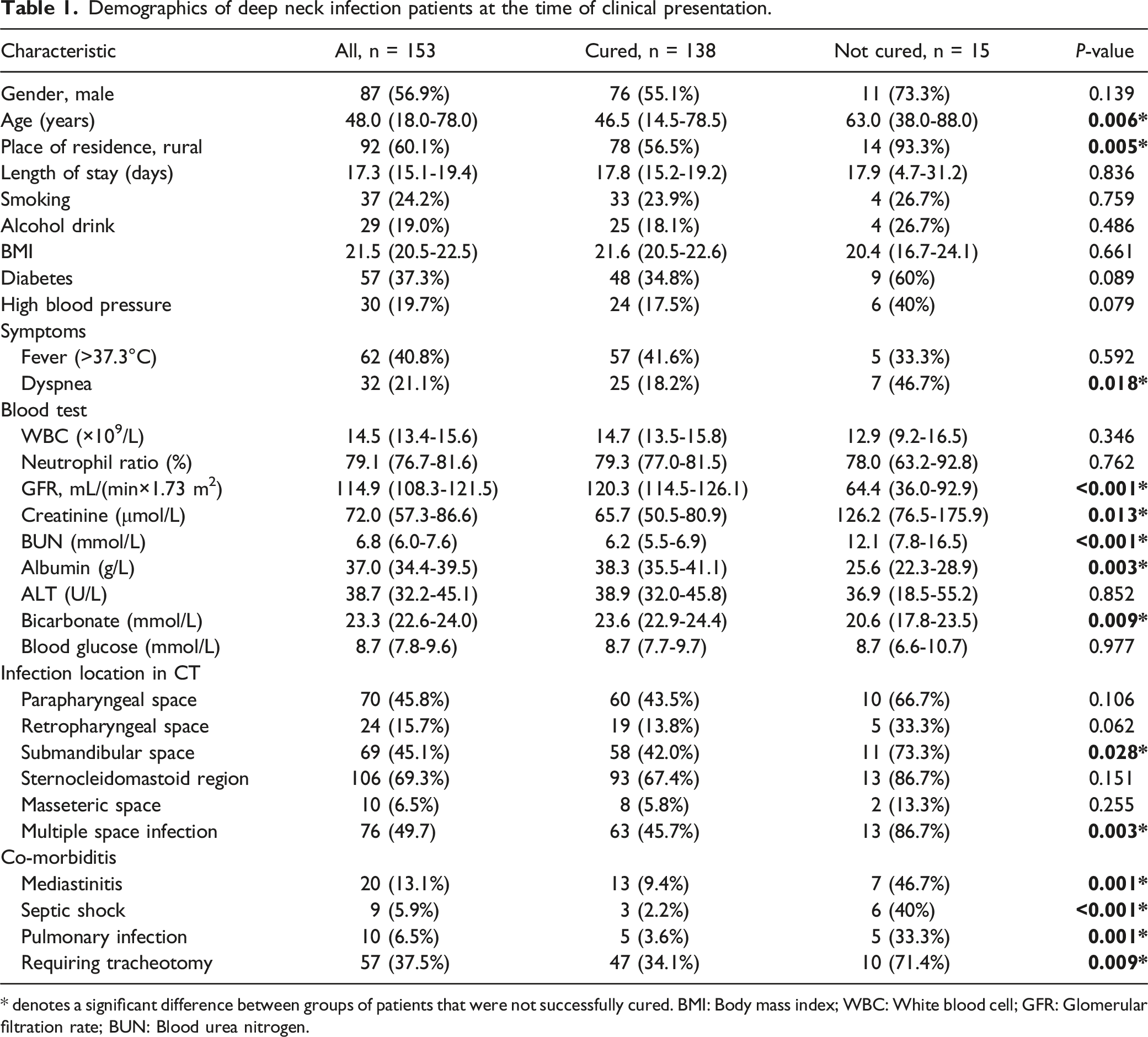
* denotes a significant difference between groups of patients that were not successfully cured. BMI: Body mass index; WBC: White blood cell; GFR: Glomerular filtration rate; BUN: Blood urea nitrogen.
Factors associated with mortality
Of the 153 patients involved in this trial, 143 underwent successful treatment and recovered or stabilized, while the remaining 15 underwent unsuccessful treatment and eventually worsened or passed away.
The average age of cured patients was 44.9 ± 3.5 years, significantly younger than those of uncured ones (60.4 ± 9.0 years). Of the cured patients, 78 lived in rural areas (56.5%), whereas 14 of the uncured patients (93.3%) were from rural areas, with a significant difference in these rates between groups (P < 0.05). Moreover, 46.7% of uncured patients presented with dyspnea, which is significantly lower than cured patients (18.2%). The serum creatinine (126.2 ± 49.7 g/L compared to 65.7 ± 15.2 g/L) and blood urea nitrogen (BUN) (12.1 ± 4.4 g/L compared to 6.2 ± 0.7 g/L) were significantly higher among uncured ones compared to cured ones.
However, the serum albumin (25.6 ± 3.3 g/L compared to 38.3 ± 2.8 g/L) and bicarbonate (20.6 ± 2.9 g/L compared to 23.6 ± 0.7 g/L) were significantly lower in the uncured group. In addition, rates of mediastinitis, submandibular space infection, the infection of multiple spaces, septic shock, and pulmonary infection were all higher among uncured patients relative to cured patients (Table 1).
Factors associated with long-term hospitalization
Mortality was not the only parameter used to assess the DNI's prognosis. The length of hospital stay for those who survived reveals the severity of the condition. For the present study, DNI patients were stratified based upon the length of hospital stay into a short-term group (< 2 weeks) and a long-term expense group (> 2 weeks). Patients in the long-term group were elder (52.1 ± 3.9 years compared to 37.3 ± 5.4 years, P < 0.001) and heavier in weight (60.4 ± 3.6 years compare to 53.6 ± 3.5 kg, P < 0.001) than those in the short-term group. Approximately 17.9% of patients in the short-term group presented with diabetes, whereas these rates were significantly higher in the long-term group (50.7%, P < 0.001). Just 9% of patients in the short-term group exhibited dyspnea at the time of presentation, compared to 27.1% of patients in the long-term group, with these latter rates being significantly higher (P = 0.007).
Factors associated with long-term hospitalization (Stay > 2 weeks).
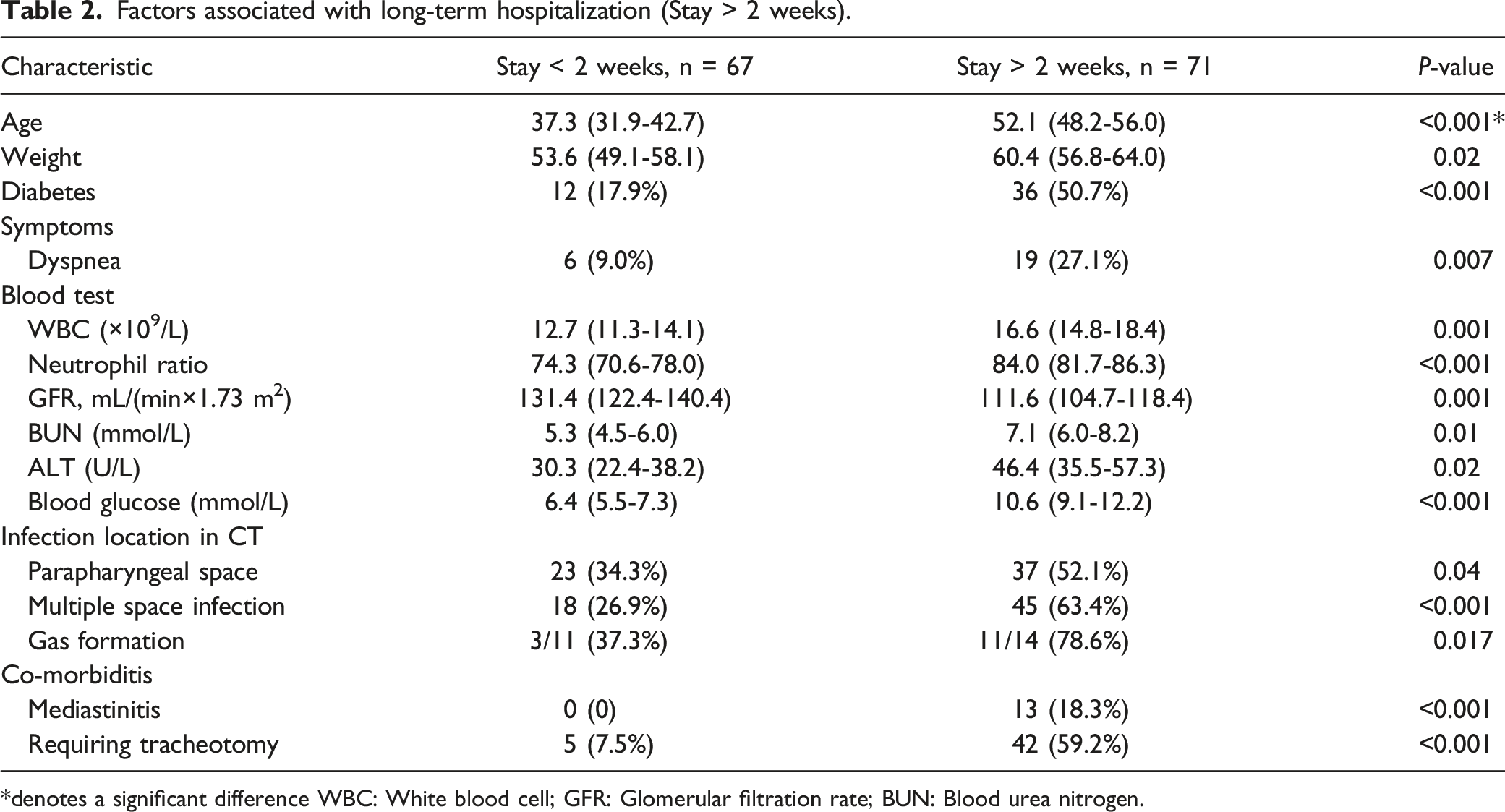
*denotes a significant difference WBC: White blood cell; GFR: Glomerular filtration rate; BUN: Blood urea nitrogen.
The development of a mortality prediction model
To establish a model capable of predicting mortality for patients at the time of clinical presentation, we incorporated the factors identified above into a logistic model. Factors in the univariate model included age >50 years (OR 4.903), rural residence (OR 10.768), dyspnea (OR 3.920), GFR <94 mL/(min×1.73 m2) (OR 33.250), creatinine >95 μmol/L (OR 28.571), BUN >7.86 mmol/L (OR 14.274), parapharyngeal space infections (OR 6.067), ALB <34 g/L (OR 30.049), Bicarbonate <18.8 mmol/L (OR 11.844), submandibular space infections (OR 3.793), the infection of multiple spaces (OR 7.738), mediastinal infections (OR 8.413), septic shock (OR 30.00), pulmonary infections (OR 13.300), and requiring tracheotomy (OR 4.840).
When these factors were incorporated into a multivariate model, only creatinine >95 μmol/L, ALB <34 g/L and mediastinal infections were retained for the final predictive model (Table 3). This model was constructed based on the factors we screened. Under this model, condition 1 applied to patients with creatinine >95 μmol/L, while condition 2 applied to patients with mediastinitis and ALB <34 g/L (both match) (Figure 2). The prediction model for mortality in deep neck infection patients. Condition 1 applies to patients with creatinine >95 μmol/L, while condition 2 applied to patients with mediastinitis and ALB <34 g/L (both match).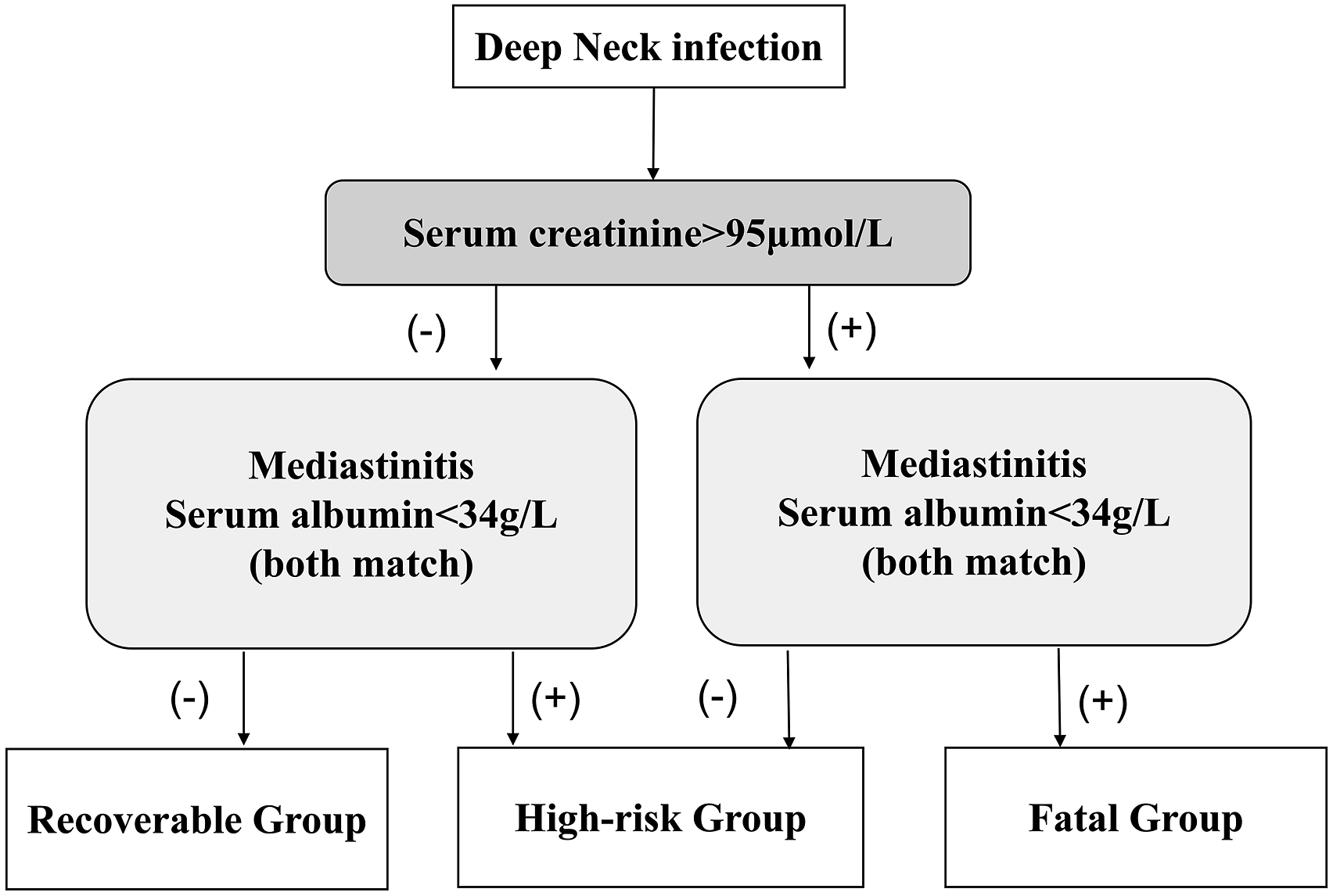
Based on condition 1 and condition 2, patients were stratified into three groups. In the Recoverable group (neither condition 1 nor condition 2 fits), 98.4% of patients survived. While in the High-risk group (either condition 1 or condition 2 fits), roughly half of the patients eventually deteriorated or died, and in the Fatal group (both of the 2 conditions fit), two-thirds of these patients died (Figure 3). The area under the ROC curve for this model is 0.896, with an 86.67% sensitivity and a 92.03% specificity. The Nagelkerke R2 value is 0.552 for this model. The distribution of mortality rate in different groups of the model, the number in the column means how many cases in each group.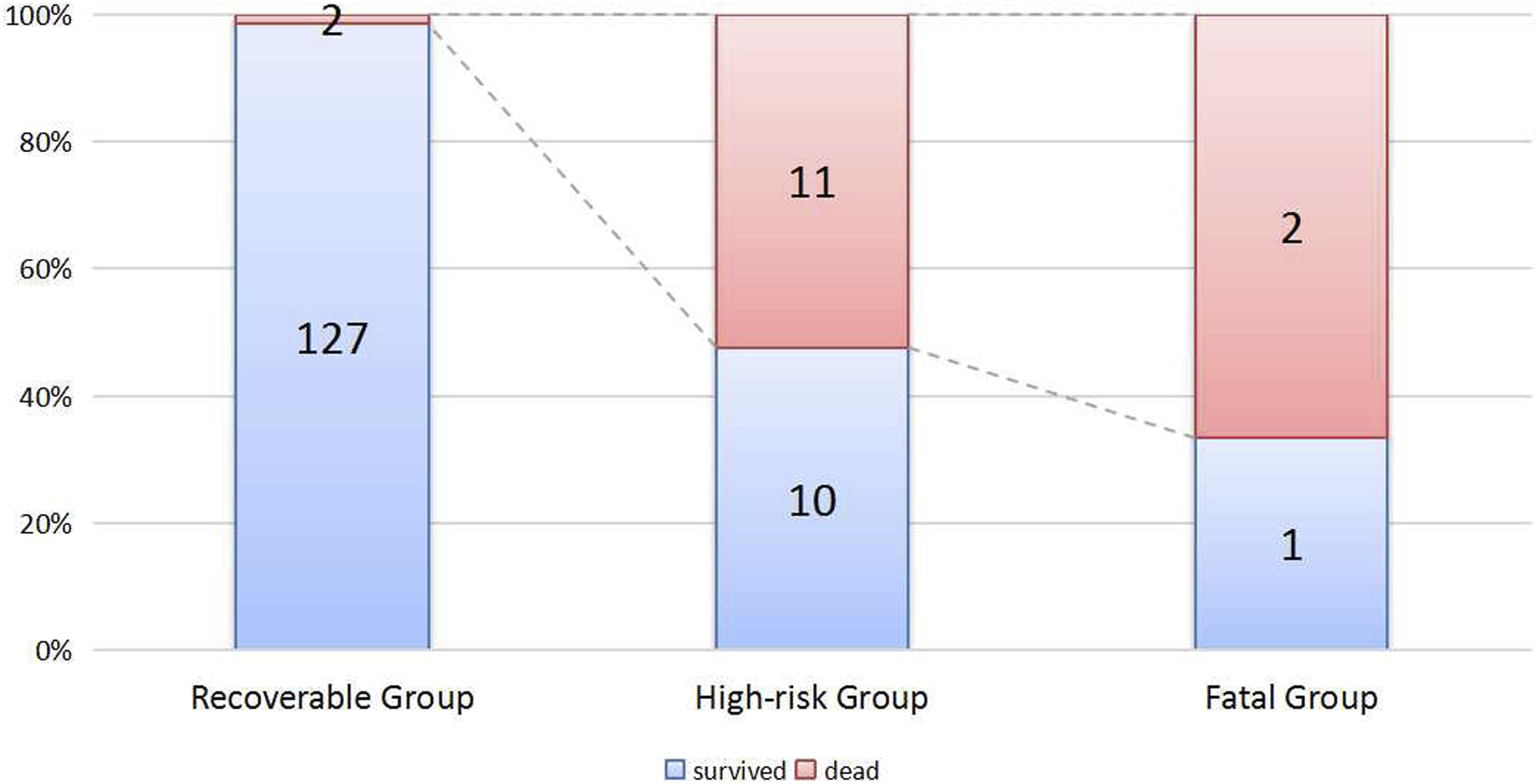
Discussion
Odds ratios for mortality-related risk factors.
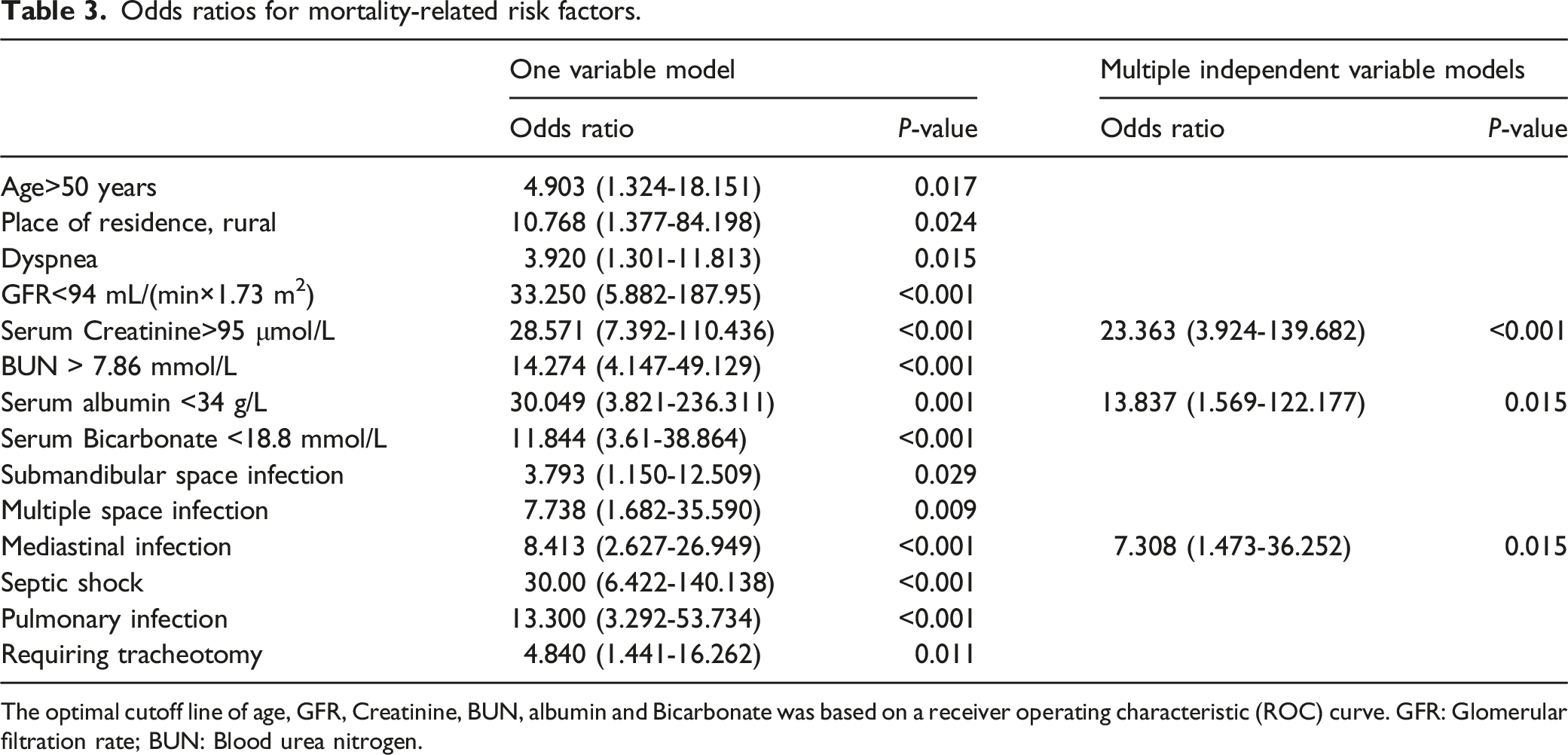
The optimal cutoff line of age, GFR, Creatinine, BUN, albumin and Bicarbonate was based on a receiver operating characteristic (ROC) curve. GFR: Glomerular filtration rate; BUN: Blood urea nitrogen.
The model developed in this study was established through multivariate logistic regression analysis and incorporated three factors: mediastinal infection status, ALB <34 g/L and creatinine >95 μmol/L. This model was constructed using the ORs associated with these variables, among which creatinine >95 μmol/L was found to be a key determinant of the final overall treatment cost for DNI patients.
First, Patients with mediastinitis have been previously reported to exhibit high mortality rates of 10-30%.1-3 Severe mediastinitis can induce tissue necrosis, contributing to subsequent septicemia and multiple organ failure that can rapidly lead to death without sufficient treatment. In our cohort, 35% of the DNI patients with mediastinitis turned out dead, confirming the close relationship between mediastinitis and mortality.
Secondly, our present research highlights the role of renal insufficiency in affecting DNI patients’ treatment outcomes. Previous research has reported a higher incidence rate of DNIs in early-stage renal disease patients.13,14 In a study on the correlation between the mortality rate of DNI and renal insufficiency, the result showed that the mortality rate of patients with DNI in the early-stage renal disease group was more than 2-fold higher than that in the control group. A recent study in 2021 supports this standpoint, 15 but no specific cutoff point values of kidney function indicators were set up for high-risk DNI patients. However, Park et al 16 declared that renal failure is a risk factor for necrotizing fasciitis, mediastinitis, and CRP >20 mg/dL but not for clinical outcomes.
Our current investigation proved that renal insufficiency is fatal for DNI patients. We set up a cutoff value of serum creatinine for high-risk DNI, with more than half of the patients finally dying if the serum creatinine is more than 95 μmol/L at the visit. This might be because patients with renal insufficiency may have poor immunologic function, causing infections to spread. Furthermore, when antibiotics are poured in, the kidney must bear a significant weight of drug metabolism, causing severe impairment to kidney function.
Thirdly, our research indicated that low serum albumin is also an important factor for poor treatment outcomes, which was seldom mentioned in previous research. Park et al 16 reported that serum albumin level <3.0 g/dL contributed to a higher rate of simultaneous mediastinitis, necrotizing fasciitis, greater extent of infection, higher initial CRP, and delayed treatment response, and longer duration of hospitalization. Our report herein strengthens the role of hypoalbuminemia in decreasing the survival rate of DNI. Albumin is thought to play an important role in mediating inflammatory response 17 and; hypoalbuminemia could be both the reason and result of systemic inflammation.
The present study explored other risk factors associated with poor patient prognosis. The analyses revealed that age >50 years, residence in a rural area, dyspnea at time of presentation, submandibular space infection, the involvement of multiple sites, serum bicarbonate <18.8 mmol/L, septic shock, and pulmonary infections at the visit were all associated with patient outcomes. In our cohort, age >50 was a predictor of poor outcomes. The negative impact of advanced age on prognosis may be related to more complications in elderly people, but not to age itself. 18 Residence in a rural area is an interesting predictor we found.
According to the previous reports, 6 almost all DNI patients were of low socioeconomic status, with roughly 70% being illiterate. Many of these patients also exhibited poor oral hygiene and presented with dental infections. Primary healthcare facilities are also lacking in rural areas, so treatment may be delayed when infections arise in these regions, leading to further deterioration. The finding that infections with multiple sites of involvement,10,19 and dyspnea13,20 are associated with greater risk is consistent with other reports indicating the presence of a wide range of lesions at the time of treatment initiation, potentially complicating treatment efforts. Patients with septic shock 21 have also previously exhibited high mortality rates, which is now confirmed in our study. However, septic shock is relatively rare compared to mediastinitis.
It is worth mentioning that diabetes is not the risk factor for mortality, according to our research, but would prolong the length of hospital stay, which is in line with previous reports.22,23 One recent study reported the average postoperative hospitalization duration for DNI patients with and without diabetes was 7 and 3 days, respectively. 22 Additional treatments to normalize blood sugar levels can contribute to prolonged hospitalization duration. Mediastinitis is a life-threatening complication of such infections and may necessitate prolonged observation in the ICU. In addition, the mediastinum is located in a deep, low location that can be difficult to drain thoroughly, further prolonging the length of hospitalization. Tracheotomy is often critical to managing DNIs, particularly in patients with airway obstruction. Older age, multiple infected spaces, mediastinitis, and gas formation have all been identified as tracheotomy-related risk factors in DNI patients in the past.19,24 These characteristics are frequently linked to a more severe clinical presentation, which could lengthen the hospital stay and call for more difficult medical procedures.
The present study has several advantages. For instance, all patients were treated in the same tertiary hospital using the same medications and surgical equipment, reducing the possibility of treatment approach-related bias. Moreover, the sample size was sufficient to permit robust statistical analyses. In our study, we set up a series of the cutoff value for mortality-related continuous variables, which could be used immediately for daily practice. Even so, there are some limitations to this study. For one, all data were collected retrospectively from medical records, which has the potential to introduce certain inaccuracies. Secondly, patients were from a single center, resulting in the potential for selection bias towards more severe or complicated cases.
Conclusions
In summary, the present study successfully identified risk factors associated with poor prognosis for patients suffering from deep neck infections. The predictive model developed herein may aid in efforts to forecast the potential for mortality before the therapeutic intervention, thereby enabling better communication between doctors and patients, particularly for patients faced with economic hardship.
Footnotes
Acknowledgments
The authors would like to thank the Medical Records and Statistics Room of the First Affiliated Hospital of Anhui Medical University for its technical support and statistical advice
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethics Committee for Research and Publication of The First Affiliated Hospital of Anhui Medical University. Written informed consent was waived owing to the use of deidentified retrospective data.