
Abstract
Chordomas are rare malignant bone tumors. Chordomas originate from notochordal elements. Chordomas have the phenotype of the embryonic notochord, characterized by the dual expression of cytokeratin and brachyury. Chordomas occur anywhere along the central axis. Rarely, chordomas occur in extra-axial structures. We could not find any reports on epiglottic chordoma. Here, we present a case of epiglottic chordoma to highlight this rare cause of laryngeal mass.
Keywords
Introduction
Chordomas are a rare malignant bone tumors with an annual incidence of 0.1 every 100 000 individuals, of which 30% occur at the skull base. 1 Chordomas originate from notochordal elements.2–5 Chordomas occur anywhere along the central axis but may also structures outside the central axis, such as skeletal muscle. 6 Computed tomography and magnetic resonance imaging are required to determine tumor localization and extent of tumor growth.
Case report
A 62-year-old female was admitted to the head and neck department of Shandong Second Provincial General Hospital for swallowing foreign body sensation in two months in April 2019 foreign body sensation with swallowing for the prior two month. Previously, the patient had no dysphagia, throat pain, cough, fever, or dyspnea.
Examination
Laryngoscopy performed in the outpatient department showed smooth cystic hyperplasia on the epiglottic laryngeal surface. The patient underwent plain and enhanced CT, which revealed an analogous round mass on the epiglottic laryngeal surface. The mass was well-defined with slight hyperdensity on the CT images. The mass showed no enhancement in the arterial phase and slight enhancement in the venous phase after injection of the contrast agent. (Figure 1) A 62-year-old woman presented with a 2-month history of swallowing obstruction. Plain CT scan and 3D reconstruction CT revealed an analogous round and slightly low-density mass on the epiglottic laryngeal surface (A, D, E). The mass showed no enhancement in arterial phase (B) and slightly nodular and enhancement in venous phase (C, F) after injection of contrast agent on enhanced CT image.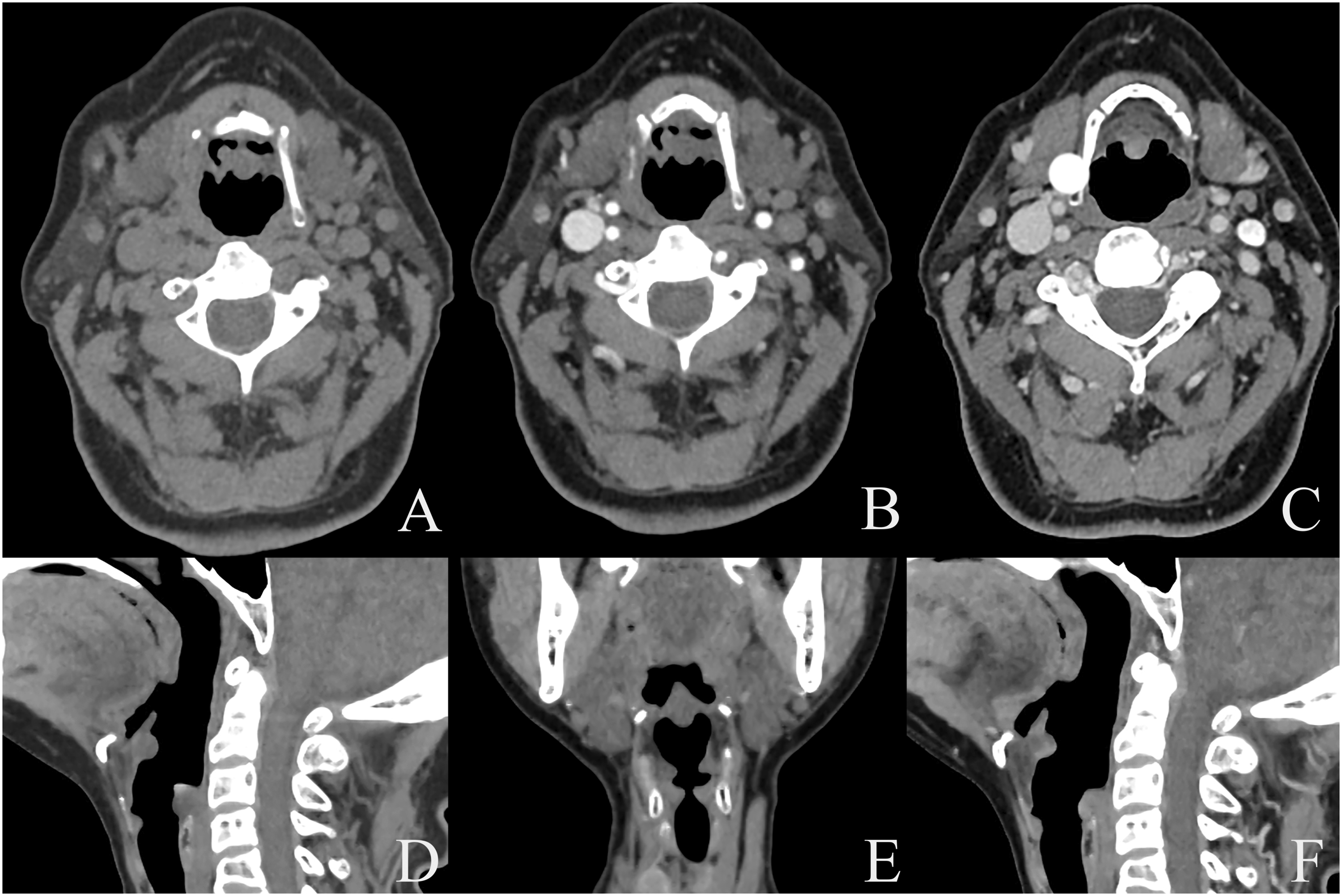
Treatment and histopathology
The patient underwent endoscopy with CO2 laser excision. The tumor was completely resected and the margins were negative. Combined with histopathological and immunohistochemical features, the patient was treated by adjuvant radiotherapy after surgery. The patient recovered well and was discharged on medical advice. Thirty-six months follow-up showed that the patient was recovering well, and so far there is no recurrence.
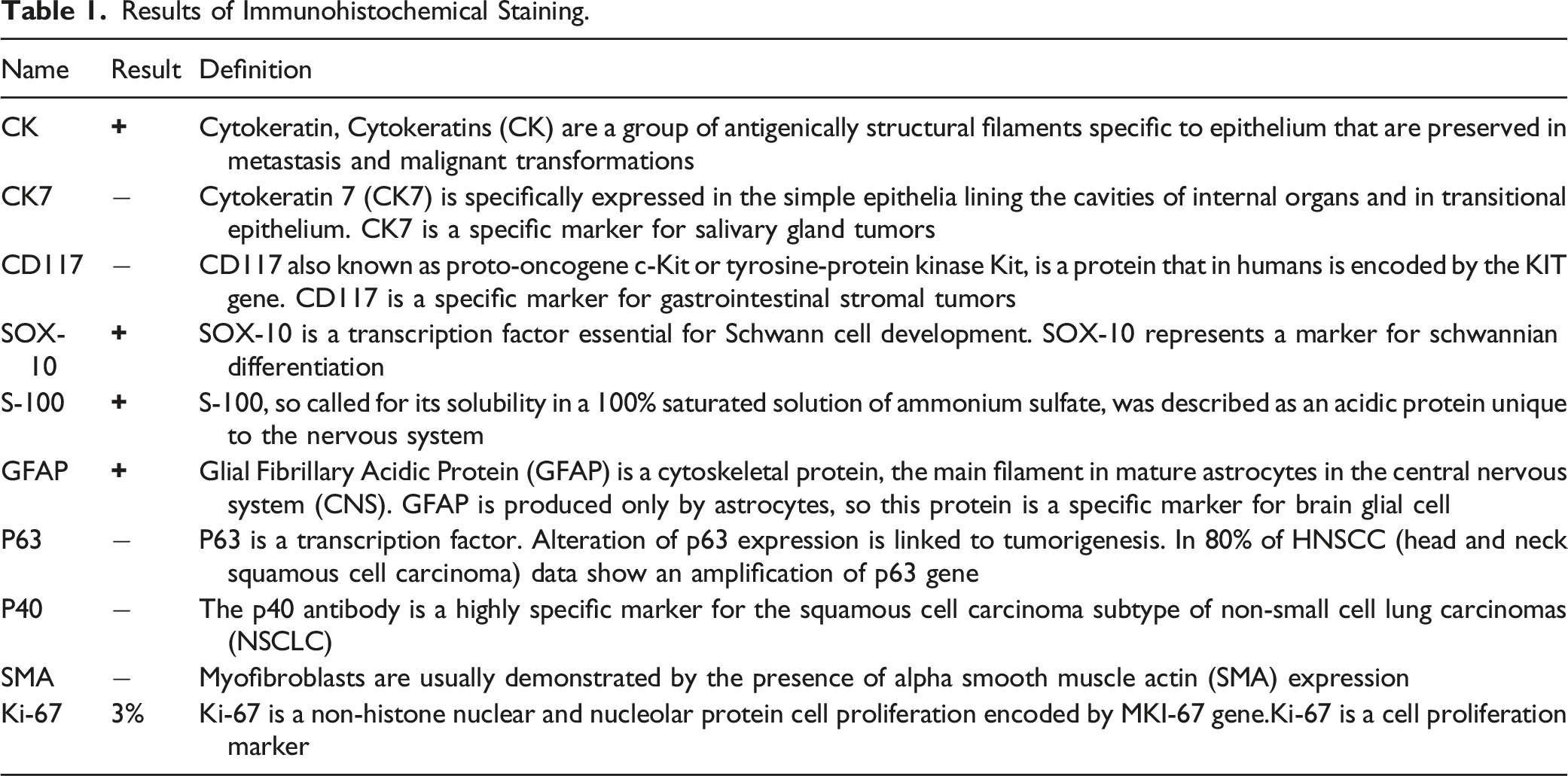
Based on histopathology (Figure 2) and immunohistochemical staining (Table 1), the patient was diagnosed with epiglottic chordoma. Tumor cells are typically arranged in cords (hematoxylin and eosin, ×10). Results of Immunohistochemical Staining.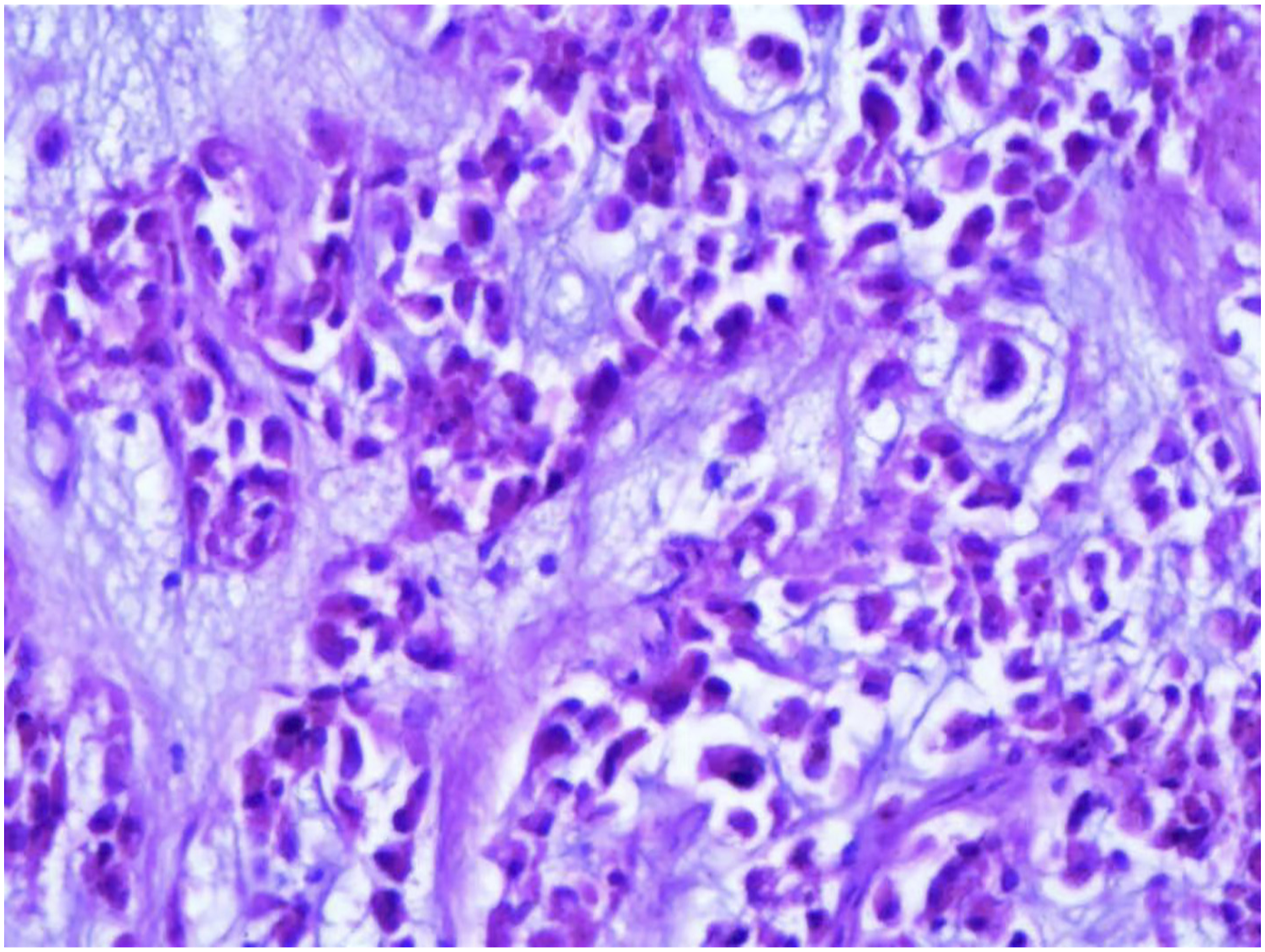
This case was misdiagnosed as an epiglottic cyst before surgery and as a lesion of small salivary gland by rapid intraoperative pathology.
Discussion
Chordomas are rare, accounting for approximately 1–4% of all bone malignancies. 1 Chordomas originate from embryonic remnants of the primitive notochord.2-5 In the third week, the notochord was attached cephalally to the oropharyngeal membrane. As the notochord degrades, it may remain or dislocate adjacent structures around it, and the remaining notochord tissue can develop chordoma.2,3 Chordomas can occur anywhere along the mid axis. Rarely, chordomas can occur in extraxial structures such as skeletal muscle.5,7 Chordomas in the larynx are rare. We believe that the epiglottic chordoma was caused by residual or dislocated notochord in the epiglottis. This may be caused by the cephalic proximity of the notochord to the oropharyngeal.
Chordomas should be differentiated from chondrosarcomas and myoepithelial neoplasms. Microscopically, chordomas appeared as lobulated structures with fiber bundles composed of densely packed spindle-shaped fibroblast-like cells encased in a population of highly vacuolated (eosinophilic) epithelioid tumor cells. Eosinophilic cells are loosely arranged and embedded in a unique and complex extracellular matrix. In some chordomas, the characteristic myxoid matrix may have hyaline cartilaginous features similar to hyaline chondrosarcoma. However, conventional hyaline chondrosarcoma may have “vacuoles” within the stroma, which at low power may mimic physaliferous cells; however, the tumor cells reside within lacunae, rather than having corded appearance. The myoepitheliomas , with their corded neoplastic cells set in a chondromyxoid stroma, can be confused with chordomas however physaliferous are not present. Since chondrosarcoma and chordoma have similar imaging features, neither MRI nor CT can be used to distinguish chordoma from chondrosarcoma preoperatively. The essential diagnostic immunoprofile of chordoma is the co-expression of cytokeratins(CK) and brachyury.8-12 Based on histopathology and immunohistochemical staining, the differential diagnosis of chordoma, chondrosarcoma, and myoepithelial neoplasms can be made.
Surgical procedures play the key role in the treatment of chordoma. When total en-bloc resection or gross total resection is not feasible, radical or near total intralesional resection is recommended. The patients were then treated by radiotherapy after surgery. 1
Chordoma was mainly confirmed by combining histopathology and immunohistochemical staining. In particular, the diagnosis of chordoma in rare areas such as the epiglottisdepends on histopathology and immunohistochemistry. Preoperative diagnosis of chordoma is very difficult. This case was misdiagnosed as an epiglottic cyst before surgery and as a lesion of small salivary gland by rapid intraoperative pathology. Based on the no expression of CK7, salivary gland tumors were excluded. Based on histopathology and immunohistochemical staining, this patient was diagnosed with epiglottic chordoma. The patient was then treated by adjuvant radiotherapy after surgery.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Medical and health Science and Technology Development Project of Shandong Province and Developing Project (grant no. 202009011530).
Patient Consent
We have obtained the consent.
Ethics Approval
We have obtained the consent and the local research ethics committee approved the study.