
Abstract
Keywords
Introduction
Empty nose syndrome (ENS) is caused by excessive resection of the nasal turbinate. 1 It presents with a variety of symptoms, including nasal obstruction, a burning sensation in the nose, dry nose, and painful nasal breathing. Due to the symptom severity, ENS is strongly associated with psychiatric disorders such as depression and may lead to suicidal attempts. 2 The surgical treatment for ENS is an inferior meatus augmentation procedure (IMAP) in which autologous tissue such as auricular cartilage, rib cartilage, or artificial material such as acellular dermis is transplanted into the nasal cavity. 3 Narrowing of the nasal cavity by means of the IMAP may increase airflow to the inferior meatus, 4 thereby improving the perception of nasal airflow. We used dermal fat, an autologous tissue whose volume can be freely adjusted. It is considered a safer option than rib cartilage because it is harvested from superficial tissue. Additionally, harvesting tissue from the inguinal region allows excellent cosmesis due to the discrete location of the donor site. Autologous fat has long been considered an option for implantation, albeit it appears it has not been extensively studied formally. 5 The purpose of this study was to investigate the efficacy and safety of the IMAP using ADF.
Patients and Methods
This study was conducted in full accordance with ethical principles and the Declaration of Helsinki. It was approved by the Ethics Committee of The Jikei University Hospital (Approval No. 33-506). All the participants provided written and verbal informed consent before inclusion.
The participants were nine patients with ENS who underwent an IMAP using ADF between December 2020 and January 2022. The patients comprised 8 males and one female, with an age range of 18-72 years (mean = 33.22 years). The ENS type 5 was ENS inferior turbinate in all patients.
ENS was diagnosed using nasal endoscopy and computed tomography (CT). The cotton test was used to confirm symptomatic changes. 6 The patients were examined by a preoperative psychiatrist to confirm the presence of psychiatric disorders.
Patient age, sex, previous nasal surgery, presence of inferior turbinate osteotomy, duration of ENS, comorbid psychiatric disorders, ENS type, Empty Nose Syndrome 6-Item Questionnaire (ENS6Q), 7 and the postoperative follow-up period were recorded. Changes in each item of the ENS6Q item before and after surgery were analyzed. The survey periods were preoperative and 1 week, 1 month, and 3 months postoperatively. All continuous variables were treated non-parametrically. Paired continuous variables were compared using the Wilcoxon signed-rank test. Values with two-sided P < 0.05 were considered significant. All data were analyzed using Stata 15.0 (StataCorp LP, College Station, TX, USA). The presence or absence of surgical complications was also noted.
Surgery
Surgery was performed under general anesthesia. In cases of severe nasal septal deviation, septoplasty was performed. A mucosal pocket was created by making an incision on the mucosa of the nasal floor. An incision of approximately 1.5 cm in the nasal floor is made at the anterior end of the inferior turbinate until the soft palate-hard palate junction. The incision was extended externally to the lateral nasal wall ridge (Fig 1a, b). ADF (3 × 8 cm) taken from the inguinal region was divided and inserted into the submucosal pocket (Fig 1c). ADF was implanted in the mucosal pocket until it was completely full. The incision layer was sutured, and the surgery was completed (Fig 1d). Schema of autologous dermal fat grafted to the floor of the nasal cavity. (a) Submucosal incision in the floor of the nose at the anterior end of the inferior turbinate. (b) Create a submucosal pocket to the posterior. (c) Transplant autologous dermal fat. (d) Suture submucosal incision.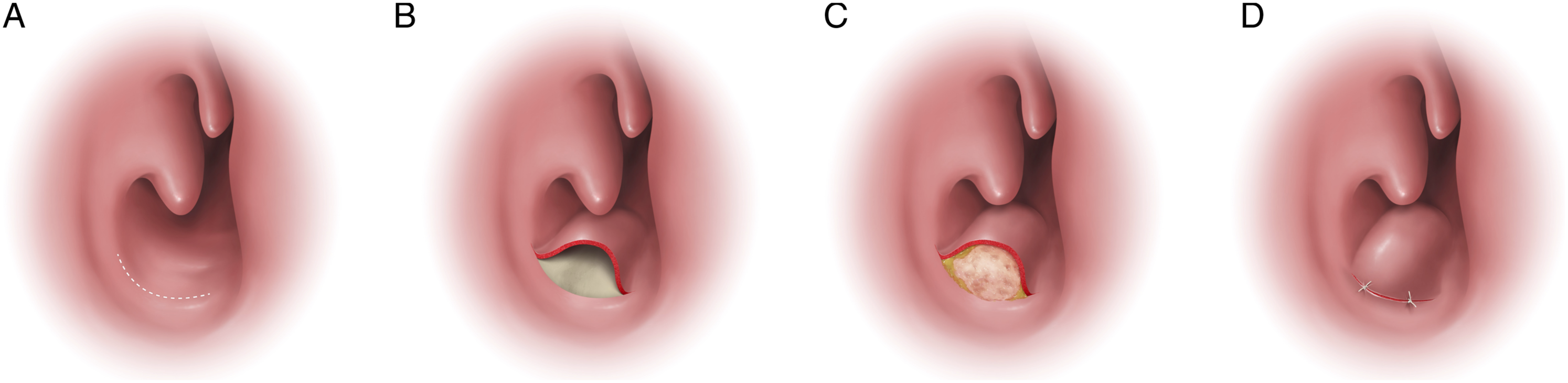
Results
Patient Background.
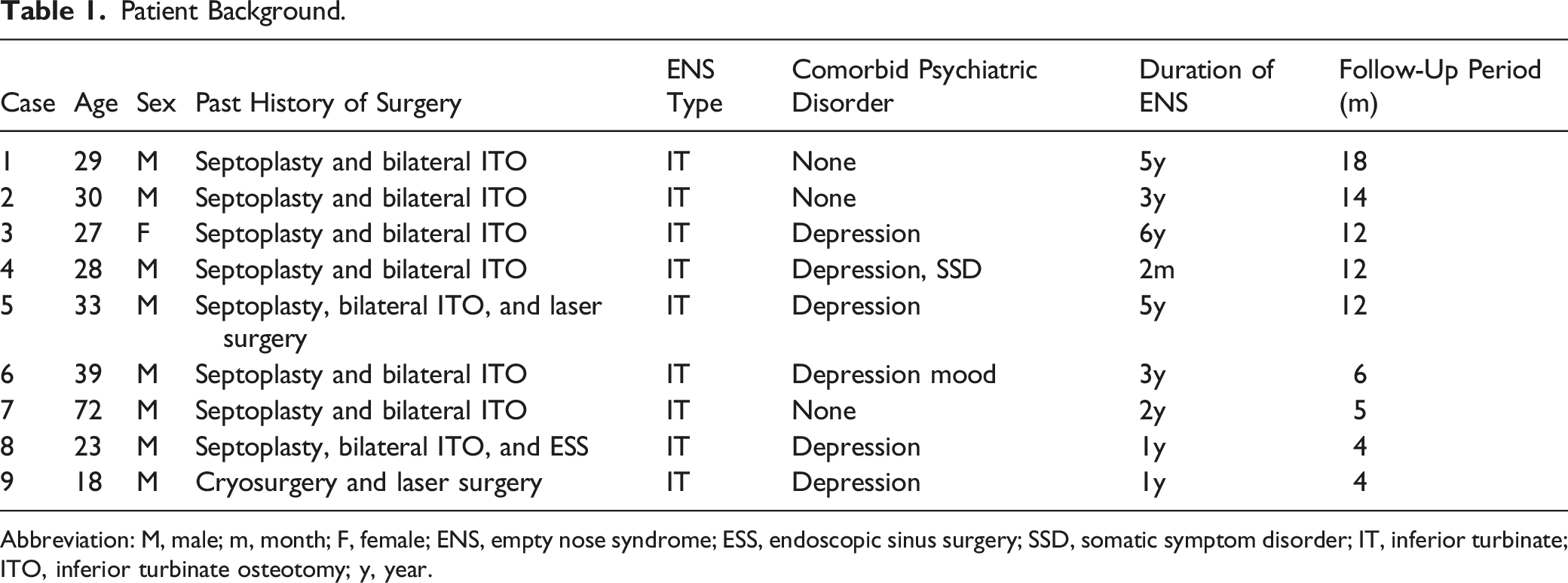
Abbreviation: M, male; m, month; F, female; ENS, empty nose syndrome; ESS, endoscopic sinus surgery; SSD, somatic symptom disorder; IT, inferior turbinate; ITO, inferior turbinate osteotomy; y, year.
ENS6Q total score
Preoperative ENS6Q total scores ranged from 14 to 25 on a 30-point scale (mean = 20). The mean scores at 1 week, 1 month, and 3 months postoperatively improved to 9.44, 5.56, and 5.00, respectively; the difference (P values) between those mean scores and baseline values was 0.0076, 0.0075, and 0.0076, respectively (Fig 2). Pre- and postoperative changes in the ENS6Q.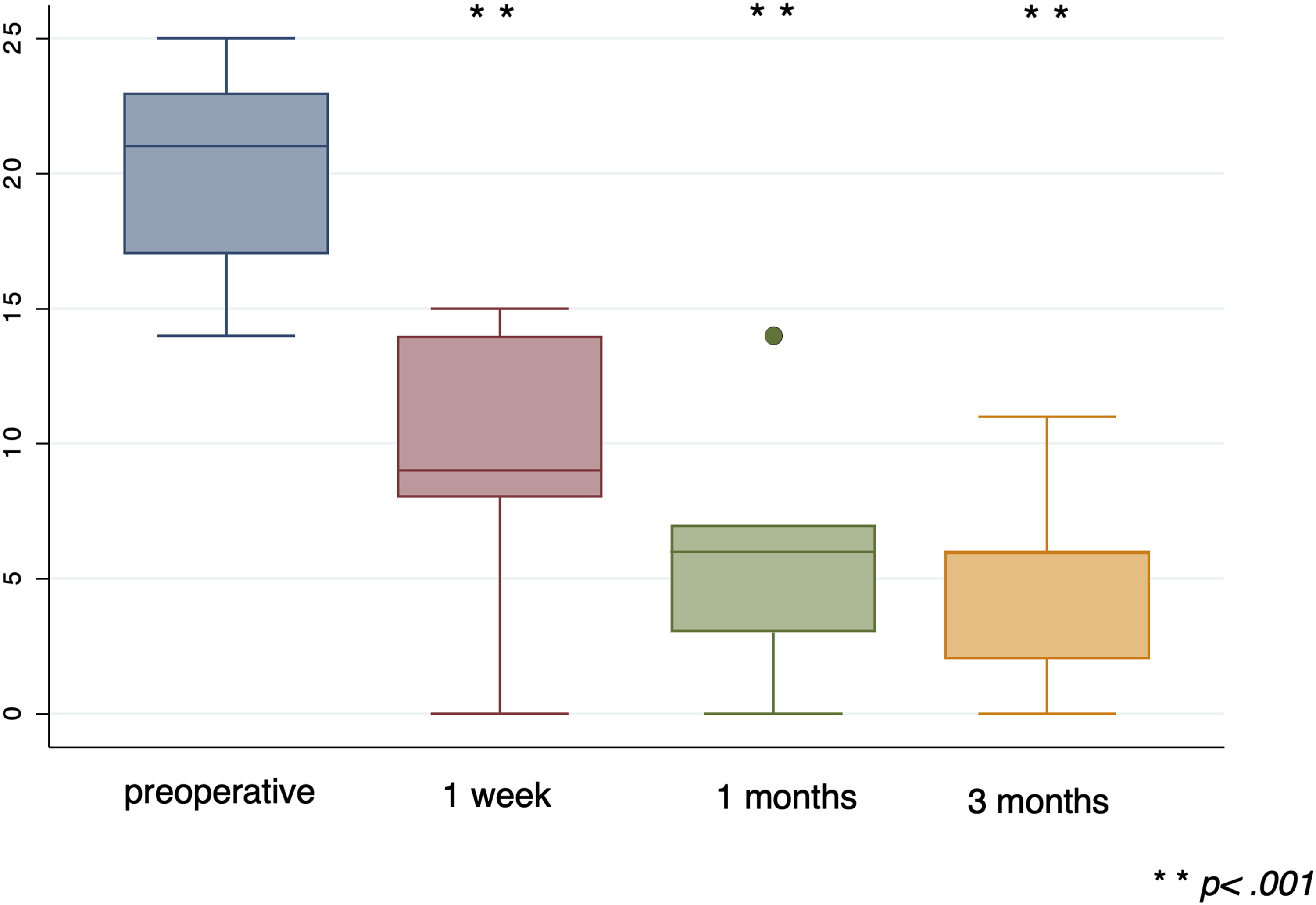
Dryness
Preoperative dryness scores ranged from 2 to 5 on a 5-point scale (mean = 4). The mean scores at 1 week, 1 month, and 3 months postoperatively improved to 2.89, 2.22, and 2.11, respectively; the difference (P values) between those mean scores and baseline values was 0.007, 0.0086, and 0.0065, respectively (Fig 3a). Pre- and postoperative changes in each item of the ENS6Q. (a) Dryness. (b) Nose feels too open. (c) Sense of diminished nasal airflow. (d) Suffocation. (e) Nasal crusting. (f) Nasal burning.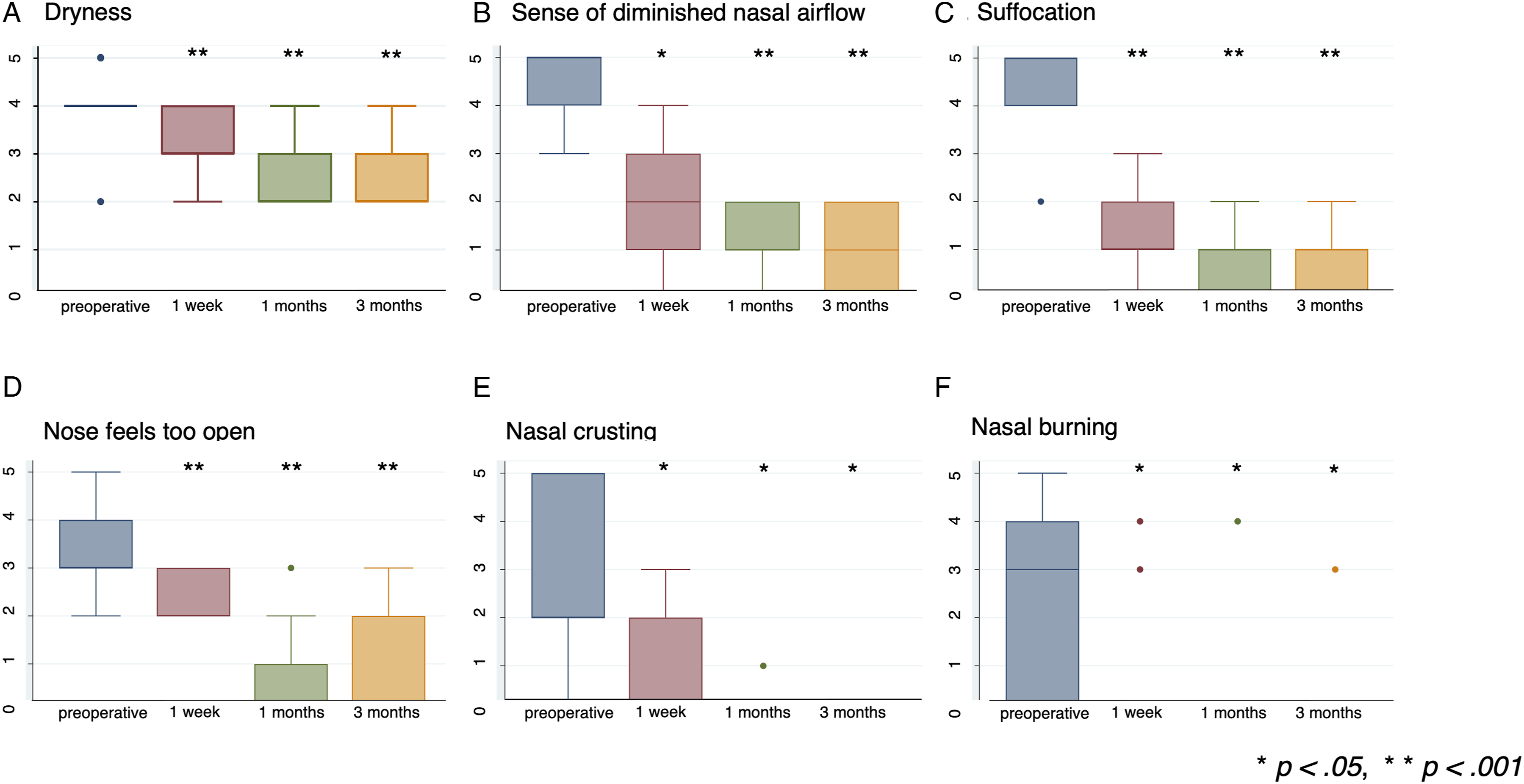
Sense of diminished nasal airflow
Preoperative sense of diminished nasal airflow scores ranged from 0 to 5 on a 5-point scale (mean = 4). The mean scores at 1 week, 1 month, and 3 months postoperatively improved to 1.77, 1.22, and 1.11, respectively; the difference (P values) between those mean scores and baseline values was 0.0116, 0.0085, and 0.0082, respectively (Fig 3b).
Suffocation
Preoperative suffocation scores ranged from 2 to 5 on a 5-point scale (mean = 4.33). The mean scores at 1 week, 1 month, and 3 months postoperatively improved to 1.33, 0.78, and 0.67, respectively. The difference (P values) between those mean scores and baseline values was 0.0071, 0.0073, and 0.007, respectively (Fig 3c).
“Nose feels too open”
Scores for the preoperative sensation of the “nose feels too open” ranged from 2 to 5 on a 5-point scale (mean = 3.56). The mean scores at 1 week, 1 month, and 3 months postoperatively improved to 1.89, 0.78, and 0.78, respectively. The difference (P values) between those mean scores and baseline values 0.0085, 0.0084, and 0.0074, respectively (Fig 3d).
Nasal crusting
Preoperative nasal crusting scores ranged from 0 to 5 on a 5-point scale (mean = 2.66). The mean scores at 1 week, 1 month, and 3 months postoperatively improved to 0.78, 0.11, and 0, respectively. The difference (P values) between those mean scores and baseline values was 0.0173, 0.0117, and 0.0115, respectively (Fig 3e).
Nasal burning
Preoperative nasal burning scores ranged from 0 to 5 on a 5-point scale (mean = 2.33). The mean scores at 1 week, 1 month, and 3 months postoperatively improved to 078, 0.44, and 0.33, respectively. The difference (P values) between those mean scores and baseline values was 0.0282, 0.0282, and 0.0282, respectively (Fig 3f).
There were no surgical complications.
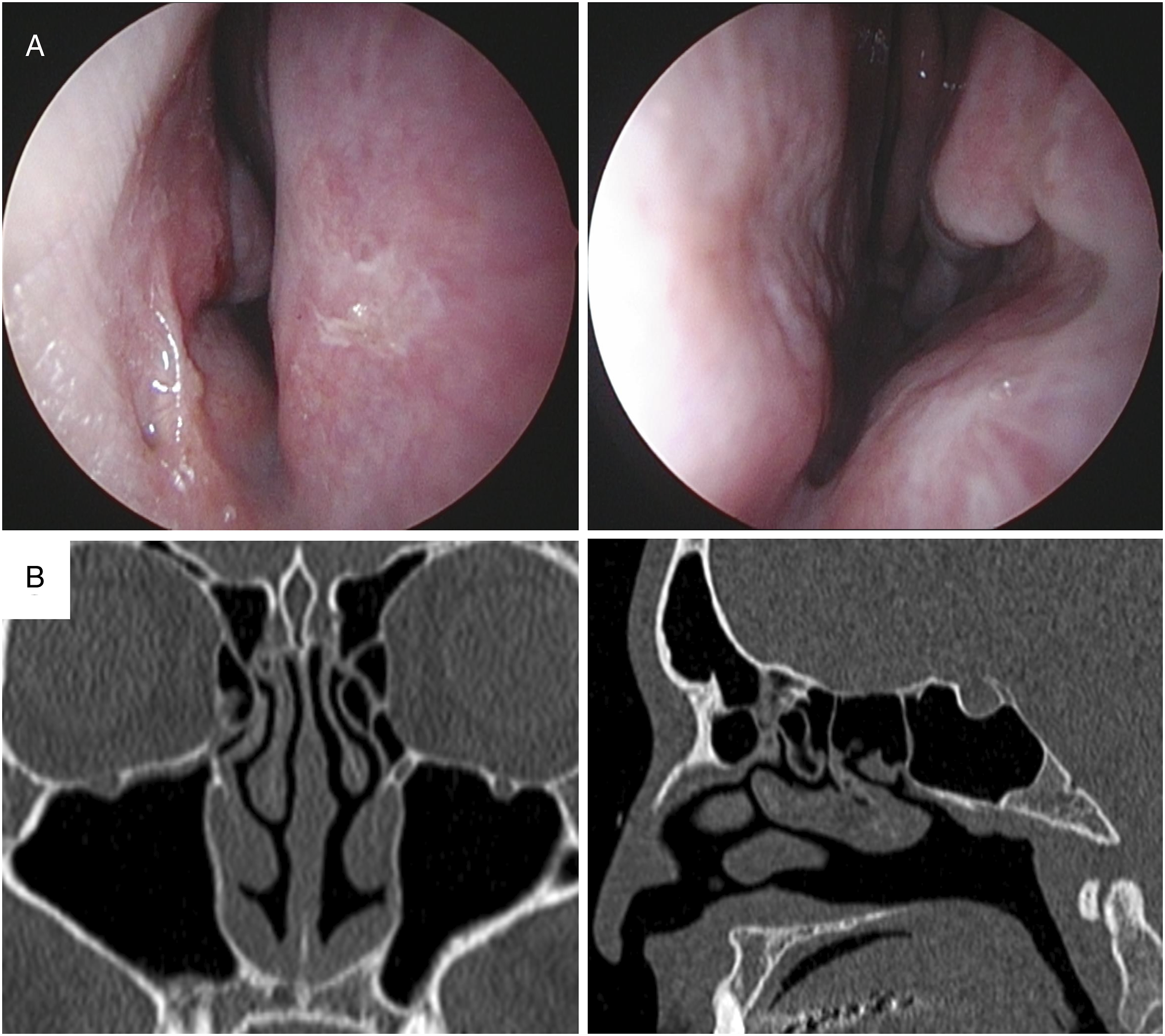
The preoperative endonasal endoscopic and CT findings are shown in Figure 4. The inferior turbinate was partially missing, and the nasal cavity was greatly enlarged. The 3-month postoperative endonasal endoscopic and CT findings are shown in Figure 5. The nasal cavity was narrowed from anterior to posterior with ADF implanted in the nasal floor. Inferior turbinate is partially missing, and the nasal cavity is greatly enlarged. (a) Preoperative endonasal endoscopic findings. (b) Preoperative computed tomography findings. Nasal cavity is narrowed from anterior to posterior with autologous dermal fat implanted in the nasal floor. (a) Endonasal endoscopic findings at 3 months postoperatively. (b) Computed tomography findings at 3 months postoperatively.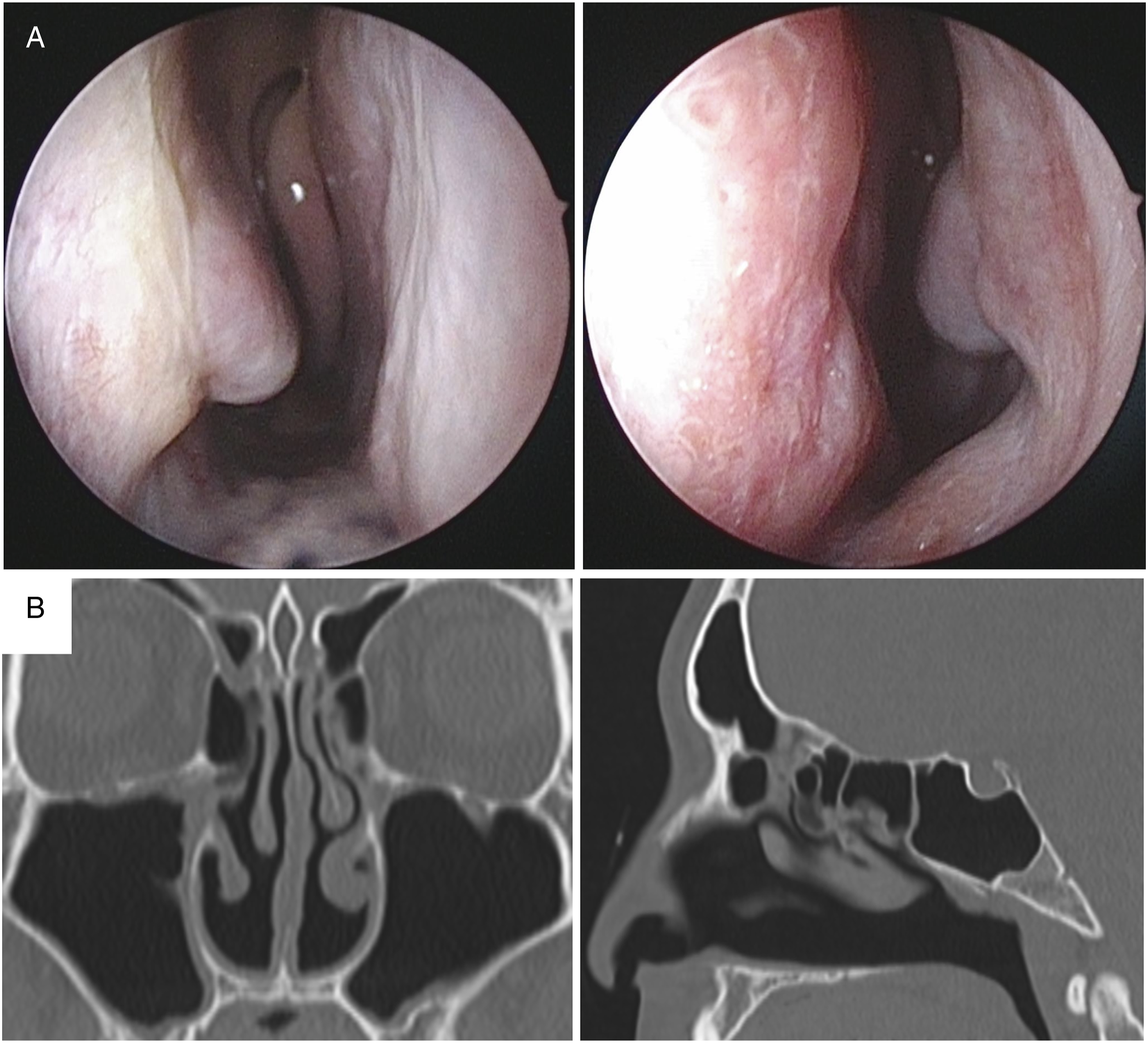
Discussion
Inferior turbinate surgery to improve nasal obstruction is widely used because of its efficacy. 8 Courtiss and Goldwyn reported that 8% of patients have dry nose after inferior turbinate surgery, 9 and this is estimated to be the incidence of ENS after inferior turbinate surgery. 5
The nasal concha regulates the quantity, velocity, and quality of air passing through the nose. 10 Excessive loss of the nasal turbinate due to nasal surgery results in excessive expansion of the nasal cavity, loss of nasal respiratory jet airflow, and increased nasal temperature. This causes a decrease in the activity of transient receptor potential melastatin 8 (TRPM8), which senses nasal respiration. This is the presumed pathogenesis of ENS. 11
Several surgical treatments have been attempted; these include narrowing the nasal cavity by placing an implant into the nasal cavity. The IMAP technique has been used in many of these cases.
Reported grafts include autologous tissues such bone, cartilage, muscle, and fat, as well as artificial materials such as acellular dermis.5,12 The high absorption rate of grafted autologous fat is a problem. It has been reported that fat can be retained by centrifuging fat aspirated with a syringe, separating it into adipose tissue only, and then grafting it. 13 Furthermore, Ibrahim et al. reported that transplantation of fat and stem cells regenerated the nasal mucosa in the treatment of ENS. In addition to improvement of nasal morphology, improvement of nasal physiology using stem cell transplantation is an ideal prospect in the treatment of ENS. 14 This is a very useful method, but it requires a centrifuge and can be performed in only few facilities. Cartilage is the most useful graft 15 because it is autologous tissue that stays in place and is not absorbed. Defects in nasal structures in ENS can be large or small. Auricular cartilage has fewer complications from harvesting and a less noticeable wound than rib cartilage. Auricular cartilage grafts are considered suitable for small defects of the turbinate. If the defect is large, a voluminous tissue graft such as rib cartilage may be necessary. 16 However, rib cartilage harvesting not only carries the risk of medically induced pneumothorax 16 but also poses cosmetic problems due to chest scarring. Dholakia et al. reported the usefulness of IMAP using cadaveric rib cartilage. Although cadaveric rib cartilage is not legally available in some countries such as ours, it is very innovative and useful. 17 Acellular dermal grafts are easy to simulate preoperatively and can be sized, but they also have the risk of infection 1 and a certain rate of resorption. 3 Additionally, some countries, such as Japan, have difficulty in obtaining insurance coverage for these procedures. ADF can be harvested in abundance, enough to narrow the nasal cavity, and can easily be adjusted in size. In addition, it can be harvested from the groin or other areas where scarring is less noticeable, making it superior in terms of cosmetic appearance. 18 The rib cartilage harvesting site in the chest can be exposed when certain types of clothes are worn, such as swimsuits. However, dermal fat can be harvested from less exposed areas such as the inguinal region. The axilla is also considered an appropriate site for dermal fat harvesting because the wound is not easily visible. However, it was not used in this study because of its frequent postoperative mobility, the risk of infection due to excessive perspiration and relatively poor ventilation in this part of the anatomy, and the risk of scar contracture. The inguinal dermis is thin but can be easily harvested simultaneously with the fat. In addition, the inguinal region was chosen for dermal fat collection because the collection wound can be concealed by underwear. The transplanted dermal fat postoperatively fuses with the surrounding tissue and is biodegradable. The advantage of autologous tissue is the low risk of infection and rejection and the low cost of medical care. 19 ADF is very soft and smooth. This is an advantage during the IMAP as it is easier to insert and can compactly be packed without gaps, which may reduce the surgical difficulty of the IMAP itself. If the inferior turbinate defect is large, a large graft is required, and ADF is considered an appropriate option for such cases as the graft size can be easily adjusted. Niechajev discussed the results of postoperative biopsy tissue results of both fat grafts and dermal fat grafts with respect to lipoplasty grafts for cleft lip. Dermal fat grafts are considered more resistant to infection than fat grafts. The dermis was also integrated with the adjacent lip as neovascular tissue, and fat tissue was also ingrown. 20 IMAP using ADF may be replaced in the nasal cavity by soft tissue that binds strongly to the nasal mucosa. Nasal tissue is inherently soft, and IMAP with ADF may be more physiologic than hard grafts such as cartilage.
In this study, the mean ENS6Q total score significantly improved postoperatively, with significant improvement in all ENS6Q parameters; however, dryness improved slightly lower than the other parameters. Narrowing of the nasal cavity by means of the IMAP may increase airflow to the inferior meatus, 4 thereby improving the perception of nasal airflow. This may be the reason why the sense of diminished nasal airflow and “nose feels too open” are improved in the ENS6Q. Patients with ENS suffer from viscous nasal discharge. Wu et al. analyzed biopsy specimens of the inferior turbinate mucosa of 17 patients with ENS and reported squamous epithelialization of the mucosa, fibrosis of the submucosal tissue, and goblet cell metaplasia in about 35% of the cases. 21 The optimal temperature for TRPM8 is approximately 22-27 °C. 22 An ENS nasal cavity, which is unable to maintain a moist environment due to decreased serous secretion and create jet airflow, is probably unable to maintain the optimal temperature for TRPM8. The IMAP only changes the morphology and is unlikely to completely improve the collapsed nasal clearance 23 of ENS. Therefore, the symptoms of dryness are unlikely to improve with the IMAP. The treatment of ENS patients requires not only an IMAP but also nasal irrigation and adequate humidification with saline sprays. 24
Various methods of inferior turbinate surgery have been reported. We use submucosal resection (SMR) at our hospital, a procedure in which only the mucosa-specific layer is reduced using a micro debrider. In this study, 8 of nine patients underwent inferior turbinate osteotomy. 25 The inferior turbinate artery (ITA), which feeds the inferior turbinate, enters from above at approximately 7.87 mm from the posterior edge of the inferior turbinate. 26 The ITA branches into 2-4 branches and runs parallel to the inferior turbinate bone, but in about 12% of cases, it runs through the bone. 27 In patients with ITAs traveling within the inferior turbinate, we hypothesized that one of the causes of ENS development may be that the main trunk of the ITA is severed by the inferior turbinate osteotomy, resulting in disruption of nutrition to the inferior turbinate. The percentage of ITA running within the inferior turbinate bone 27 and the incidence of dry nose after inferior turbinate surgery 9 are approximately equal.
It has been reported that to prevent the development of ENS, the reduction of the inferior turbinate should be less than 50%. 24 The following surgical techniques have been considered appropriate: radiofrequency ablation, laser, electrocautery, or SMR with a microdebrider. 24 However, at this time, it is not possible to predict the risk of developing ENS by the amount of inferior turbinate resection. 28 The key to preventing ENS is to avoid performing inferior turbinate surgery hastily. Surgical indications for inferior turbinate surgery should be limited to (1) highly symptomatic patients with nasal congestion, (2) moderate-to-severe inferior turbinate tissue hypertrophy clearly obstructing the upper airway and resulting in symptoms, (3) dynamic changes through the day and night and left-to-right alternating nasal obstruction (implying an inferior turbinate etiology), and (4) nasal congestion symptoms and turbinate hypertrophy that both improve after decongestant application (thus proving that tissue reduction is pleasing to the patient). 10
Many patients with ENS suffer from depression and other psychiatric disorders. 29 Awareness of ENS is low and patients are undiagnosed or misdiagnosed by their healthcare providers, resulting in multiple hospital visits. The symptoms are perceived by physicians as incomprehensible. Symptoms such as quitting work, avoiding social relationships, and withdrawing to one's room due to ENS symptoms are consistent with somatic symptom disorder (SSD). Tian et al. reported the effectiveness of psychiatric intervention for ENS patients with SSD. 30 The IMAP can also improve the physical and psychiatric symptoms of ENS.3,31 In our hospital, psychiatric intervention is performed in all cases before surgical treatment of ENS. As otolaryngologists, we believe that it is imperative to not only prevent the development of ENS after inferior nasal sinus surgery but also to understand the disease concept, accept the various symptoms of ENS patients, and reassure patients.
Our study had the following limitations: the small number of participants and the short follow-up period. ADF has been reported to be less resorbed in lipoplasty, 32 but the long-term results in the nasal cavity in ENS cases are still unknown. In future, we would like to increase the number of participants, follow-up the patients long-term, and report the results. We would also like to compare the results of using different IMAP materials.
Conclusion
Our study showed that IMAP using ADF for ENS was an effective method for improving ENS symptoms. As a graft, it is larger than auricular cartilage and has less risk of complications than rib cartilage. Autologous tissue is less prone to infection and rejection. Symptoms related to nasal airflow improve, but physiological function is difficult to improve, and dryness tends to persist.
Footnotes
Author Contribution
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.