
Abstract
Objective:
The purpose of this prospective, randomized, single-blinded, placebo-controlled study was to investigate the effects of radiofrequency ablation (RFA), diode laser, and microdebrider-assisted inferior turbinoplasty (MAIT) techniques on patients’ quality of life (QOL) and to compare the techniques with a placebo procedure.
Methods:
A total of 98 consecutive patients with enlarged inferior turbinates due to persistent year-round rhinitis were randomized into placebo, RFA, diode laser, and MAIT groups at a ratio of 1:2:2:2. All the procedures were carried out under local anesthesia with the patients’ eyes covered. Assessments were conducted prior to surgery and 3 months subsequent to the surgery. Quality of life was assessed with the Glasgow Health Status Inventory (GHSI).
Results:
The GHSI total score increased statistically significantly in all the groups, including placebo. There were no significant differences in the GHSI total score change between RFA, diode laser, and MAIT groups. The MAIT procedure improved the GHSI total score significantly more than the placebo procedure (P = .04).
Conclusion:
All inferior turbinate surgery techniques lead to a significant improvement in the patients’ QOL, and no significant differences were found between the techniques. The placebo treatment also improved the QOL significantly. Only the MAIT technique improved the QOL significantly more compared to placebo.
Introduction
The enlargement of the inferior turbinates is a common cause of chronic nasal obstruction. 1 There are several different surgical techniques to reduce the size of the inferior turbinates. Radiofrequency ablation (RFA) and microdebrider-assisted inferior turbinoplasty (MAIT) are the most commonly used and studied techniques. 2 The diode laser has also gained increasing popularity for its ease of use in the office setting.3,4 The literature supports that all 3 techniques are effective in treating chronic nasal obstruction caused by inferior turbinate enlargement.2,3 Nasal obstruction can cause problems such as difficulties with nasal breathing and impaired sleep quality. These symptoms may have an adverse effect on the quality of life (QOL) of sufferers both physically and mentally.5-7 The effect of inferior turbinate surgery on patients’ QOL has been studied in randomized clinical trials,8-11 nonrandomized controlled studies,12-15 and case series.16,17 According to most of these studies, inferior turbinate surgery improves the patients’ QOL. However, there has been a lack of placebo-controlled QOL trials.
The main purpose of this prospective, randomized, single-blinded, placebo-controlled study was to compare the effects of 3 common inferior turbinate surgery techniques (RFA, MAIT, and diode laser) and a placebo procedure on the patients’ QOL measured with the Glasgow Health Status Inventory (GHSI).
Patients and Methods
This prospective randomized study was carried out at Tampere University Hospital, Tampere, Finland, between February 2014 and September 2017. The institutional review board approved the study design (R13144), and all patients provided written, informed consent.
Patients
A total of 98 consecutive adult patients with enlarged inferior turbinates due to persistent year-round rhinitis were enrolled in this study. There is no determined minimal clinically important difference value for the GHSI questionnaire in the previous literature, which made it difficult to carry out reliable power analysis. We estimated the amount of approximately 100 patients to be adequate. The patients presented symptoms of bilateral nasal obstruction that had not responded to a 3-month trial of appropriate treatment with intranasal corticosteroids. Patients with significant nasal septum deviation, internal/external valve collapse/stenosis, chronic rhinosinusitis with or without polyposis, previous nasal surgery, sinonasal tumor, severe systemic disorder, severe obesity, or malignancy were excluded. Serum-specific IgE level measurements were used to identify the patients with an allergic sensitization. Allergic sensitization was defined as a specific IgE >0.35 for any common airborne allergen (cat, dog, horse, birch, grass, mugwort, Dermatophagoides pteronyssinus, and molds).
The definition of inferior turbinate enlargement was based on persistent bilateral symptoms, a finding of bilateral swelling of the inferior turbinate in nasal endoscopy, and the evident shrinking of both turbinates in a decongestion test. The nasal response to the topical vasoconstrictor 0.5% xylometazoline hydrochloride (Nasolin; Orion) in both nasal cavities 15 minutes before obtaining the second measurement was evaluated objectively using acoustic rhinometry (Acoustic rhinometer A1; GM instruments Ltd). An improvement of less than 30% in anterior nasal cavity volume (V2-5 cm) in one or both nasal cavities was considered normal and those patients were excluded from the study. The limit value of 30% was chosen according to previous literature.18-20
Randomization
Patients were consecutively randomized into placebo, RFA, diode laser, and MAIT groups at a ratio of 1:2:2:2 using Minim, an MS-DOS program that randomizes patients to treatment groups by the method of minimization. Proportional amounts of patients with allergic sensitization were kept similar for each group. Age and sex distributions were also kept similar for each group.
Surgery
The surgical treatment was performed in similar circumstances at the day surgery department of the hospital’s ENT clinic. All surgical procedures were performed by the same surgeon (T.H.). The procedures were carried out under local anesthesia with the patient’s eyes covered. First, the inferior turbinate was topically anesthetized using cotton strips with a mixture of lidocaine 40 mg/mL (Lidocain; Orion) and 2 to 3 drops of epinephrine 0.1% in 5 to 10 mL of lidocaine. Some 1.5 mL of local anesthetic (Lidocain 10 mg/mL c. adrenalin 10 µg/mL; Orion) was then applied to the medial portions of both inferior turbinates. All the procedures were performed under the direct vision of a straight, 4 mm-diameter, 0-degree endoscope (Karl Storz). In all the groups with every technique, the treatment was performed on the medial side of the anterior half of the inferior turbinate.
The RFA treatment was carried out with a radiofrequency generator (Sutter RF generator BM-780 II). A “Binner” bipolar needle electrode was inserted into the medial submucosal tissue of the inferior turbinate. The upper and lower parts of the anterior half of the inferior turbinate were treated for 6 seconds at a 10 W output power in 3 areas.
The diode laser treatment was given with a FOX Laser (A.R.C. LASER GmbH). The settings were as follows: wavelength of 980 nm, output power of 6 W in continuous wave mode, and a laser delivery by a 600-µm fiber using “contact” mode. Four parallel stripes were made on the mucosa by drawing the fiber from the posterior to the anterior along the medial edge of the anterior half of the inferior turbinate.
In the MAIT treatment, a 2.9 mm-diameter rotatable microdebrider tip (Medtronic Xomed) was firmly pushed toward the turbinate bone until it pierced the mucosa of the anterior face of the inferior turbinate. Next, a submucosal pocket was dissected by tunneling the elevator tip in an anterior-to-posterior and superior-to-inferior sweeping motion. Once an adequate pocket had been created, resection of the stromal tissue was carried out by moving the blade back and forth in a sweeping motion, with the system set at 3000 rpm using suction irrigation.
In the placebo procedure, small (2-3 mm in diameter) nasal mucosal biopsies were first taken from the anterior medial portions of the inferior turbinates, causing minor bleeding. Next, a radiofrequency tissue ablation device was turned on repeatedly near the patient but without the needle electrodes of the device touching the patient; the patient could only hear the acoustic tone of the device. During this sound deception, a suction tube and a nasal endoscope were moved lightly in both sides of the nose for a couple of minutes in order to convince the patients that they had undergone surgery.
Glasgow Health Status Inventory
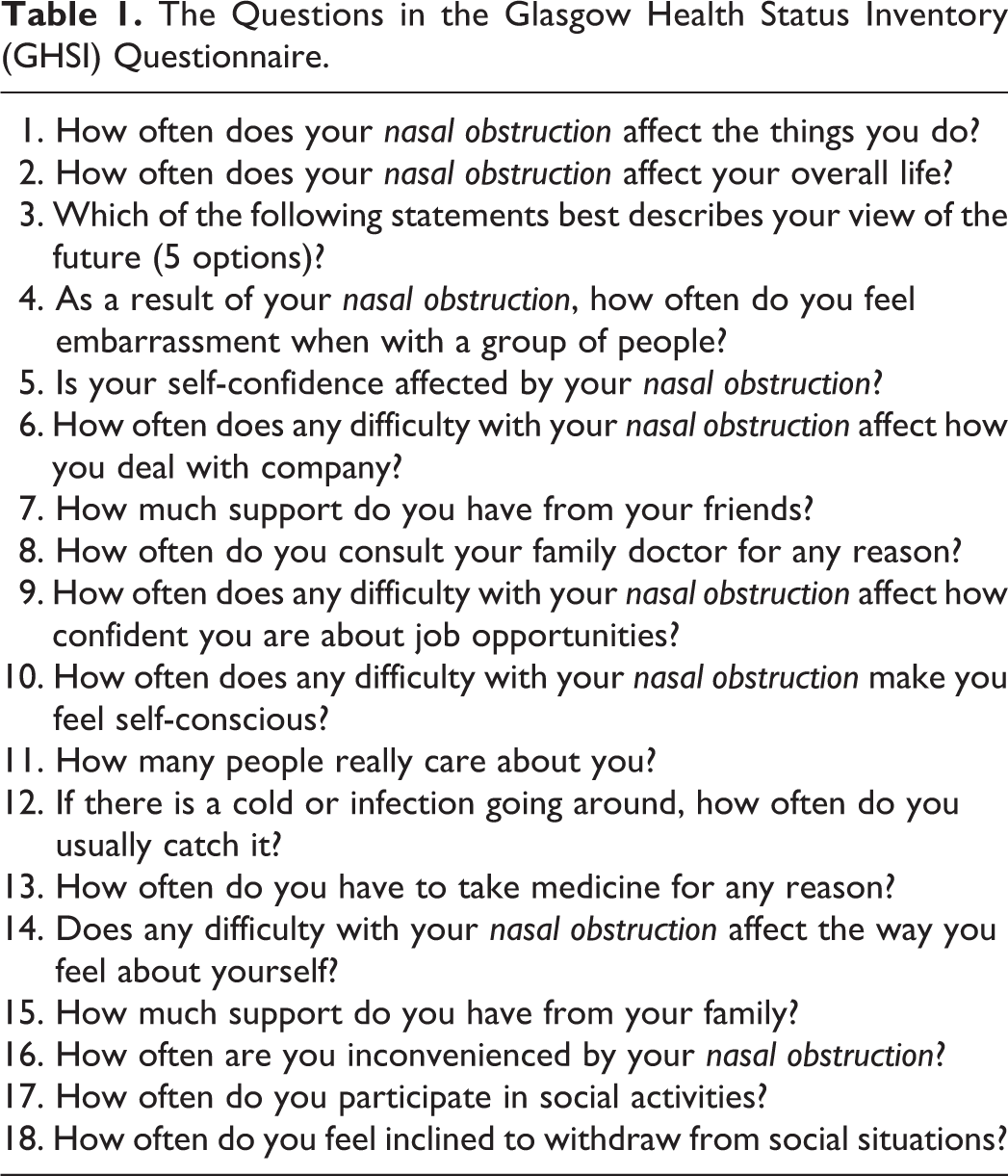
All the patients were evaluated prior to surgery and 3 months subsequent to the surgery. All clinical examinations were performed by the same examiner (T.H.) who was also the operator and not blinded to the patients’ group. During the visits, the patients filled the GHSI questionnaire (Table 1). The Glasgow Health Status Questionnaires—the GHSI and Glasgow Benefit Inventory (GBI)—are developed by the Medical Research Council’s Institute of Hearing Research in collaboration with the Glasgow Royal Infirmary, Scotland. 21 The GHSI is a state questionnaire measuring the effect of a health problem on the sufferers’ QOL. This all-purpose questionnaire is designed to measure especially otorhinolaryngological conditions and is adapted to a specific disease by replacing the words “health problem” in each question with the appropriate problem. The questionnaire contains 18 questions, and the responses are measured with a 5-point Likert-type scale. A score of 1 indicates a low health status and a score of 5 a high health status. In half of the questions, the answers range from 1 to 5 and in the other half from 5 to 1. This is done in order to receive as reliable answers as possible and thus reduce the response bias. In addition to the total score, there are 3 subscales: the general subscale (questions 1-6, 9, 10, 14, 16, 17, and 18), the social subscale (questions 7, 11, and 15), and the physical subscale (questions 8, 12, and 13). All raw scores are transformed to a scale from 0 to 100. The increase in the score indicates an improvement in the patient’s health status and QOL.
The Questions in the Glasgow Health Status Inventory (GHSI) Questionnaire.
Statistical Analysis
IBM SPSS Statistics 23.0 was used for the statistical analyses. All nonparametric data were statistically processed using the Wilcoxon signed-rank test, Mann-Whitney U test, and Kruskal-Wallis test. In the cases with parametric data, the paired samples t test and 3-way analysis of variance (ANOVA) were used.
Results
Patient characteristics are described in Table 2 and the changes in the GHSI scores in Table 3. The statistical analysis was carried out between the pre- and postoperative GHSI scores for each group separately, and the comparison of the GHSI score changes was also carried out. There were no statistically significant differences between the groups in the preoperative GHSI scores in any of the subscales. A 3-way ANOVA was run to examine the effect of sex, allergic sensitization, and procedure group on the GHSI total score change. Sex and allergic sensitization did not have any significant individual main effect on the change in the GHSI total score.
Patients’ Characteristics.a
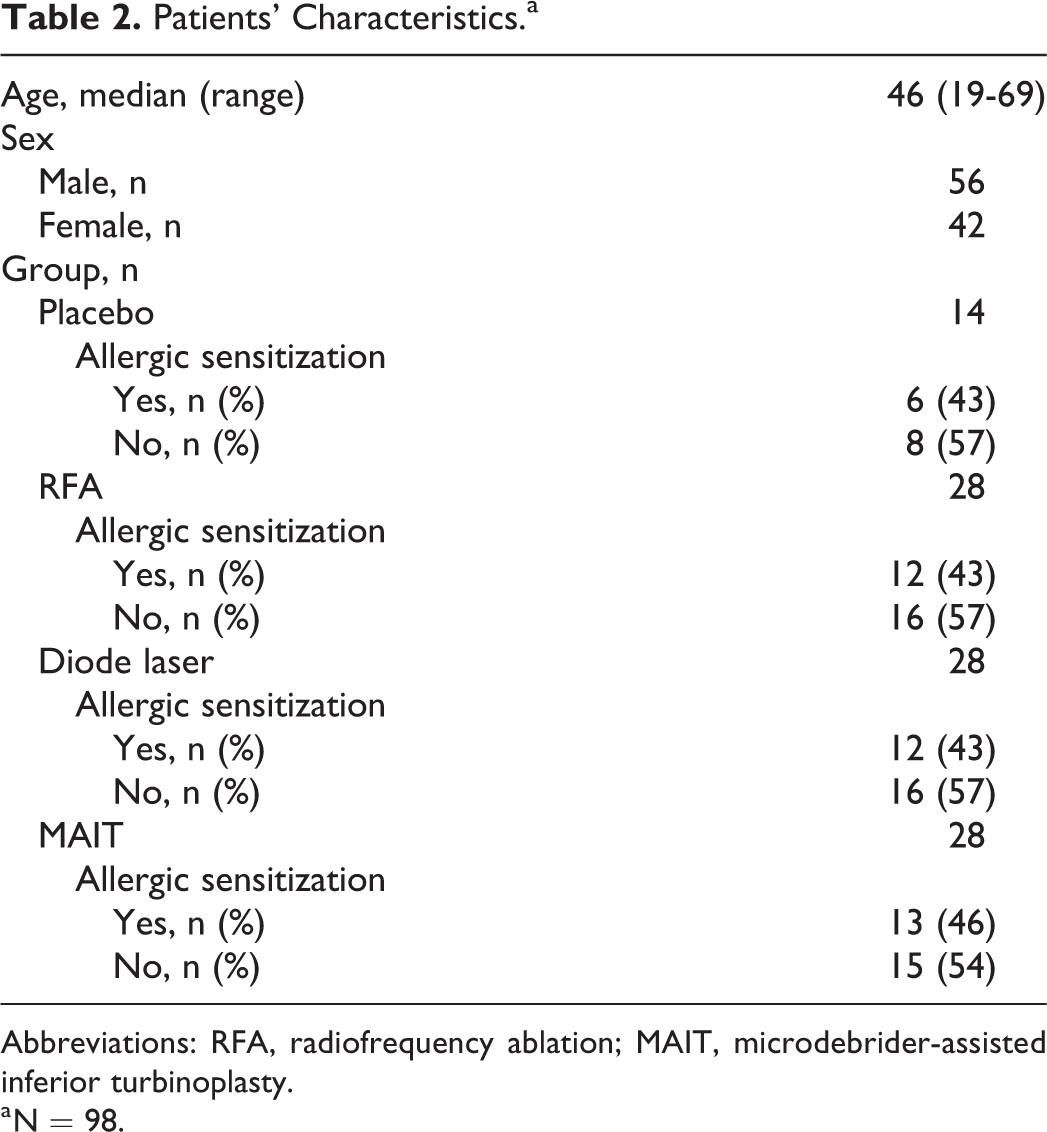
Abbreviations: RFA, radiofrequency ablation; MAIT, microdebrider-assisted inferior turbinoplasty.
a N = 98.
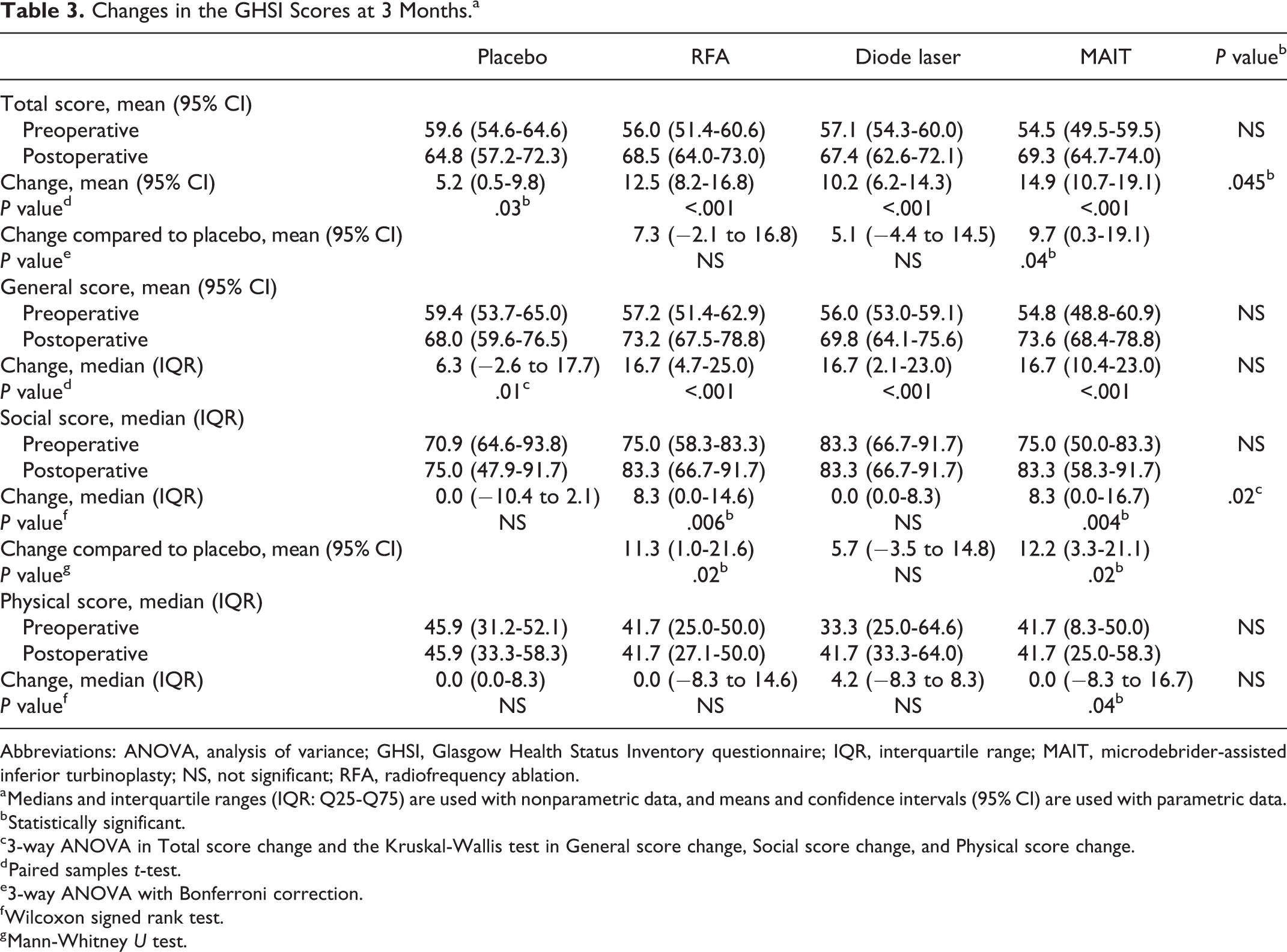
Changes in the GHSI Scores at 3 Months.a
Abbreviations: ANOVA, analysis of variance; GHSI, Glasgow Health Status Inventory questionnaire; IQR, interquartile range; MAIT, microdebrider-assisted inferior turbinoplasty; NS, not significant; RFA, radiofrequency ablation.
a Medians and interquartile ranges (IQR: Q25-Q75) are used with nonparametric data, and means and confidence intervals (95% CI) are used with parametric data.
b Statistically significant.
c3-way ANOVA in Total score change and the Kruskal-Wallis test in General score change, Social score change, and Physical score change.
d Paired samples t-test.
e3-way ANOVA with Bonferroni correction.
f Wilcoxon signed rank test.
g Mann-Whitney U test.
The GHSI total score increased statistically significantly in all the procedure groups, including placebo. There were no significant differences in the change in the GHSI total score between RFA, diode laser, and MAIT groups. Only the MAIT procedure improved the GHSI total score statistically significantly more than the placebo procedure (P = .04).
A statistically significant increase was detected in all the procedure groups in the general score subscale. However, there were no statistically significant differences between the groups.
In the social subscale, the scores increased statistically significantly in the RFA and MAIT groups. When the real treatment groups were compared separately with the placebo group using the Mann-Whitney U test, RFA (P = .02) and MAIT (P = .02) were found to have improved the GHSI social subscale score statistically significantly more compared to the placebo procedure.
In the physical subscale, only the MAIT group increased the score statistically significantly. There were no statistically significant differences between the procedure groups.
Discussion
The QOL of nasal obstruction patients can be measured with several different questionnaires. The most frequently used instrument in the current literature seems to be the Nasal Obstruction Symptom Evaluation (NOSE) scale.9,12,13 The scale is especially developed to assess the nasal obstruction before and after septoplasty. This brief questionnaire containing 5 questions has been proved to be reliable and responsive. 22 However, the NOSE scale is developed and validated only for septoplasty patients, and since it evaluates only one symptom, it is not actually a pure QOL instrument. 23 These were the main reasons for not using the NOSE scale in the present study. Other popular QOL questionnaires concerning sinonasal diseases include the Sino-nasal Outcome Test (SNOT-20) 24 and its newer modification, SNOT-22. 25 Since these questionnaires are developed for chronic rhinosinusitis, they do not purely measure nasal obstruction. Consequently, these questionnaires were not used in the present study. The Rhinoconjunctivitis Quality of Life Questionnaire and its modifications, which are instruments designed for allergic rhinoconjunctivitis patients,23,26 have been used in some nasal obstruction studies.8,14,15 A few studies have also used the GBI,13,27 which is developed together with the GHSI and measures the change in the patient’s health status after an otorhinolaryngological intervention. 21 In some studies, the patients’ QOL has been measured with general instruments, such as One the Short form health survey (SF-36)23,28 and the World Health Organization Quality of Life.9,11,29
In the present study, the QOL of the nasal obstruction patients was measured with the GHSI. We did not find any previous inferior turbinate surgery studies using the GHSI. The main reason for choosing the GHSI instead of the GBI was that we believed the effect of the intervention would be easier to detect and more reliable with a questionnaire carried out pre- and postoperatively. In a recent study, the clinimetric properties of the GHSI and the GBI were assessed. The study concluded that of the 2 subjective outcome measurement tools, the GHSI received preferable results in the 3 quality domains (validity, reliability, and responsiveness). 30
The RFA and MAIT techniques have previously been studied individually in 3 long-term studies (follow-up ≥1 year)8,14,16 and in one short-term study (follow-up < 1 year). 15 In all of these studies, both RFA and MAIT were found to improve the patients’ QOL statistically significantly. In a recent prospective, randomized study, Stözel et al studied the effect of 3 different inferior turbinate surgery techniques on the patients’ nasal obstruction and QOL, namely, turbinectomy with lateralization, submucosal electrocautery, and laser cautery. Using the SNOT-20 survey, they detected a significant improvement in the patients’ QOL in all 3 groups during a 6-month follow-up. Despite the slight differences, the study could not point to any of the techniques being preferable. 10 In several studies, the inferior turbinate intervention has also been found to improve the QOL when performed together with or compared to septoplasty or septorhinoplasty.12,13,17 However, 2 randomized clinical trials compared the QOL of groups who had septorhinoplasty with or without inferior turbinate intervention and did not find the addition of inferior turbinate intervention to be significant in improving the patients’ QOL.9,11
The present study is the first placebo-controlled study investigating the effect of inferior turbinate procedures on the patients’ QOL. The finding that all 3 studied surgical techniques improved the patients’ QOL significantly is in line with the previous literature.8,14-16 No statistically significant differences in the GHSI scores were found between the 3 surgical techniques (diode laser, RFA, and MAIT). However, when comparing the treatments to the placebo procedure, only MAIT improved the GHSI total score significantly better than placebo. In MAIT, the submucosa of the turbinate is emptied immediately during the operation, which leads to potentially faster response compared to the RFA and diode laser procedures, in which the heat caused by the device creates a submucosal scarring and tissue volume reduction.1,31 In addition, more crusting was seen in the noses of the patients in the RFA and the diode laser groups at the control visit. These are possible explanation for the finding that why only the MAIT technique improved the GHSI total score significantly better than the placebo procedure.
The aim of a placebo control is to find the true treatment effect of the intervention. In the present study, the mean true treatment effect in the GHSI total score for MAIT was 9.7. Without the placebo control, we would have detected a falsely greater and more significant improvement in the patients’ QOL caused by the procedure. It is notable that also the placebo procedure improved the GHSI total score and the general subscale score significantly. Considering how complex parameters for feelings of nasal obstruction or patency are, it is understandable that improvement in the GHSI scores was detected also with the placebo procedure. In general, the improvement of a symptom can be explained by the natural course of a disease or by a therapeutic intervention. In this case, the follow-up period was only 3 months, which makes it unlikely that the chronic nasal obstruction would relieve due to natural course by time. There were no real therapeutic intervention carried out in the placebo group. Therefore, the improvement in the symptom can be explained mainly by the placebo effect.
Although only MAIT showed a statistically significant difference compared to the placebo procedure in the total GHSI score, better scores were achieved also with the diode laser and the RFA procedures than with the placebo procedure. However, with the other 2 techniques, the differences compared to the placebo were nonsignificant. This can be seen most clearly in the total GHSI score and in the general subscale score. This can be partly explained by the relatively small number of patients in the placebo group. With a larger study population, statistically significant differences could possibly have been gained also with the other 2 techniques. In addition, there is no determined minimal clinically important difference value for the GHSI questionnaire, and therefore, the clinical meaning of the finding for the patient is not entirely confirmed. However, statistically significant GHSI score differences of the same magnitude as in the present study can be found in the recent literature. In a randomized controlled trial by van Egmond et al, septoplasty was found to improve the QOL, measured with the GHSI, more effectively than nonsurgical management for nasal obstruction in adults with a deviated septum. The statistically significant GHSI score difference favoring septoplasty was 8.3. 32 In the present study, the follow-up period of 3 months is also relatively short. In the future, placebo-controlled with longer follow-up periods should be considered in order to investigate the real long-term effect of inferior turbinate surgery on QOL.
Conclusion
All 3 inferior turbinate surgery techniques investigated in the present study led to a significant improvement in the patients’ QOL, and no significant differences were found between the techniques. The placebo treatment also improved the patients’ QOL significantly, and only the MAIT technique improved the patients’ QOL significantly more compared to the placebo procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.