
Abstract
Objectives:
The purpose of the study was to examine the various preoperative predictive factors of inferior turbinate surgery and to find possible factors that predict an optimal subjective response using 3 common surgical techniques—radiofrequency ablation (RFA), diode laser, and microdebrider-assisted inferior turbinoplasty (MAIT)—in a randomized, prospective study with a 1-year follow-up.
Methods:
The patients filled a visual analogue scale (VAS) questionnaire regarding the severity of nasal obstruction prior to and 1 year after surgery. A VAS score improvement of 3 points or more was chosen as an optimal subjective response. Univariate and multivariate regressions were used to evaluate the effect of the predictive factors. In total, 80 patients attended a 1-year control visit.
Results:
In the multivariate analysis, patients without anterior septal deviation had a statistically significantly higher odds ratio of a satisfactory subjective response compared to patients with anterior septal deviation (5.6; 95% CI: 1.4-23.1; P = .02). Patients treated with RFA had a statistically significantly higher odds ratio of an optimal subjective response compared to patients treated with MAIT (9.0; 95% CI: 1.5-54.2; P = .02).
Conclusions:
Anterior septal deviation seems to decrease the likelihood of an optimal subjective response to inferior turbinate surgery, which supports the consideration of concomitant septoplasty at least in clear cases to optimize the subjective response. Radiofrequency ablation had a significantly higher likelihood of an optimal subjective response compared to MAIT. Further investigations regarding the findings are needed.
Introduction
Inferior turbinate enlargement due to chronic rhinitis is one of the main causes of chronic nasal obstruction. 1 If the conservative treatment of rhinitis with intranasal corticosteroids does not relieve the nasal obstruction enough, inferior turbinate surgery can be considered.2,3 Various techniques have been described for the reduction of enlarged inferior turbinates. Radiofrequency ablation (RFA) and microdebrider-assisted inferior turbinoplasty (MAIT) are the most commonly used techniques worldwide, 4 and diode laser treatment has also gained in popularity in recent years. 5
There are not many studies that have evaluated the effect of various possible predictive factors on the results of the surgery. Most of those studies have dealt with the predictive effect of the preoperative vasoconstriction test on inferior turbinate surgery results.6-8
The purpose of the present study is to examine various preoperative predictive factors of inferior turbinate surgery and to try to find possible factors that predict an optimal subjective response to inferior turbinate surgery.
Patients and Methods
This prospective randomized study was carried out at Tampere University Hospital, Tampere, Finland, between February 2014 and July 2018. The institutional review board approved the study design (R13144), and all the patients provided written, informed consent.
A total of 98 consecutive adult patients with enlarged inferior turbinates due to persistent perennial allergic or nonallergic rhinitis were enrolled in this study. The patients presented symptoms of bilateral nasal obstruction related to inferior turbinate congestion that had not responded to a 3-month trial of appropriate treatment with intranasal corticosteroids. Patients with severe nasal septal deviation affecting the nasal valve region (minimal cross-sectional area [MCA] value < 0.35 cm2) in acoustic rhinometry (Acoustic rhinometer A1, GM instruments Ltd) on the deviated side, internal/external valve collapse/stenosis, chronic rhinosinusitis with or without polyposis, previous nasal surgery, sinonasal tumor, severe systemic disorder, severe obesity, or malignancy were excluded.
Cone beam computed tomography (CBCT) (Planmeca Max, Planmeca) was used to exclude patients with chronic rhinosinusitis from the study. Coronal and axial CBCT projections were also used in the evaluation and classification of septal deviation in addition to clinical examination and acoustic rhinometry. Serum-specific immunoglobulin E (IgE) level measurements were used to identify patients with an allergic sensitization. Allergic sensitization was defined as a specific IgE >0.35 for any common airborne allergen (cat, dog, horse, birch, grass, mugwort, Dermatophagoides pteronyssinus, and molds). The definition of inferior turbinate enlargement was based on persistent bilateral symptoms, a finding of bilateral swelling of the inferior turbinate in nasal endoscopy, and the evident shrinking of both turbinates in a decongestion test. The nasal response to the topical vasoconstrictor 0.5% xylometazoline hydrochloride (Nasolin) in both nasal cavities 15 minutes before obtaining the second measurement was evaluated objectively using acoustic rhinometry. An improvement of less than 30% in anterior nasal cavity volume (V2-5 cm) in one or both nasal cavities was considered normal, and those patients were excluded from the study. The limit value of 30% was chosen according to previous literature.9-11
Patients were consecutively randomized into placebo, RFA, diode laser, and MAIT groups in a ratio of 1:2:2:2 using Minim, an MS-DOS program that randomizes patients to treatment groups by the method of minimization. Proportional amounts of patients with allergic sensitization were kept similar for each group. Age and sex distributions were also kept similar for each group.
All surgical procedures were performed by the same surgeon (T.H.). First, the inferior turbinate was topically anesthetized using cotton strips with a mixture of lidocaine 40 mg/mL (Lidocain) and 2 to 3 drops of epinephrine 0.1% in 5 to 10 mL of lidocaine. Next, 1.5 mL of local anesthetic (Lidocain 10 mg/mL circa adrenalin 10 µg/mL) was then injected to the medial portions of both inferior turbinates. In all the groups with every technique, the treatment was performed on the medial side of the anterior half of the inferior turbinate.
The RFA treatment was carried out with a radiofrequency generator (Sutter RF generator BM-780 II). A “Binner” bipolar needle electrode was inserted into the medial submucosal tissue of the inferior turbinate. The upper and lower parts of the anterior half of the inferior turbinate were treated for 6 seconds at 10 W output power in 3 areas.
The diode laser treatment was given with a FOX Laser (A.R.C. LASER GmbH). The settings were as follows: wavelength of 980 nm, output power of 6 W in continuous-wave mode, and laser delivery by a 600 µm fiber using “contact” mode. Four parallel stripes were made on the mucosa by drawing the fiber from the posterior to the anterior direction along the medial edge of the anterior half of the inferior turbinate.
In the MAIT treatment, a 2.9 mm diameter rotatable microdebrider tip (Medtronic Xomed) was firmly pushed toward the turbinate bone until it pierced the mucosa of the anterior face of the inferior turbinate. Next, a submucosal pocket was dissected and the resection of the stromal tissue was carried out by moving the blade back and forth in a sweeping motion with the system set at 3000 rpm using suction irrigation.
Patients in the placebo group were excluded from the study after the 3-month follow-up. The results of the 3-month follow-up with the placebo group have been reported in a previous paper. 12 The follow-up of the genuinely treated patients was continued. In total, 80 patients (26 in the RFA, 28 in the diode laser, and 26 in the MAIT group) attended a 1-year control visit. One patient in the RFA group withdrew from the study at 3 months due to poor response. Another patient in the RFA group and 2 patients in the MAIT group did not come to the 1-year control visit for unknown reasons.
All the patients were evaluated prior to surgery and 1 year after surgery. Patients filled a visual analogue scale (VAS) questionnaire regarding the severity of nasal obstruction. A VAS score improvement of 3 points or more was chosen as an optimal subjective response. The chosen limit value of the VAS score improvement was based on our previous finding regarding the magnitude of the placebo effect in inferior turbinate surgery. 12
Univariate and multivariate regressions using IBM SPSS version 25.0 were used to evaluate the effect of the predictive factors—age, preoperative subjective severity of nasal obstruction, preoperative V2 to 5 cm change (%) after decongestant (vasoconstriction test), amount of perennial allergens sensitized, sex, possible anterior septal deviation, and operation technique—on the likelihood of an optimal subjective response.
Results
The distributions of the predictive factors’ values (continuous variables) and patient numbers (categorical variables) between the VAS score improvement groups are described in Table 1. Some 67% of the patients with anterior septal deviation and 87% of the patients without anterior septal deviation had a VAS score improvement for the severity of nasal obstruction of 3 points or more. Some 65% of the patients treated with MAIT, 75% with the diode laser, and 89% with RFA had a VAS score improvement for the severity of nasal obstruction of 3 points or more.
The Distributions of the Predictive Factors’ Values (Continuous Variables) and Patient Numbers (Categorical Variables) Between the VAS Score Improvement Groups.
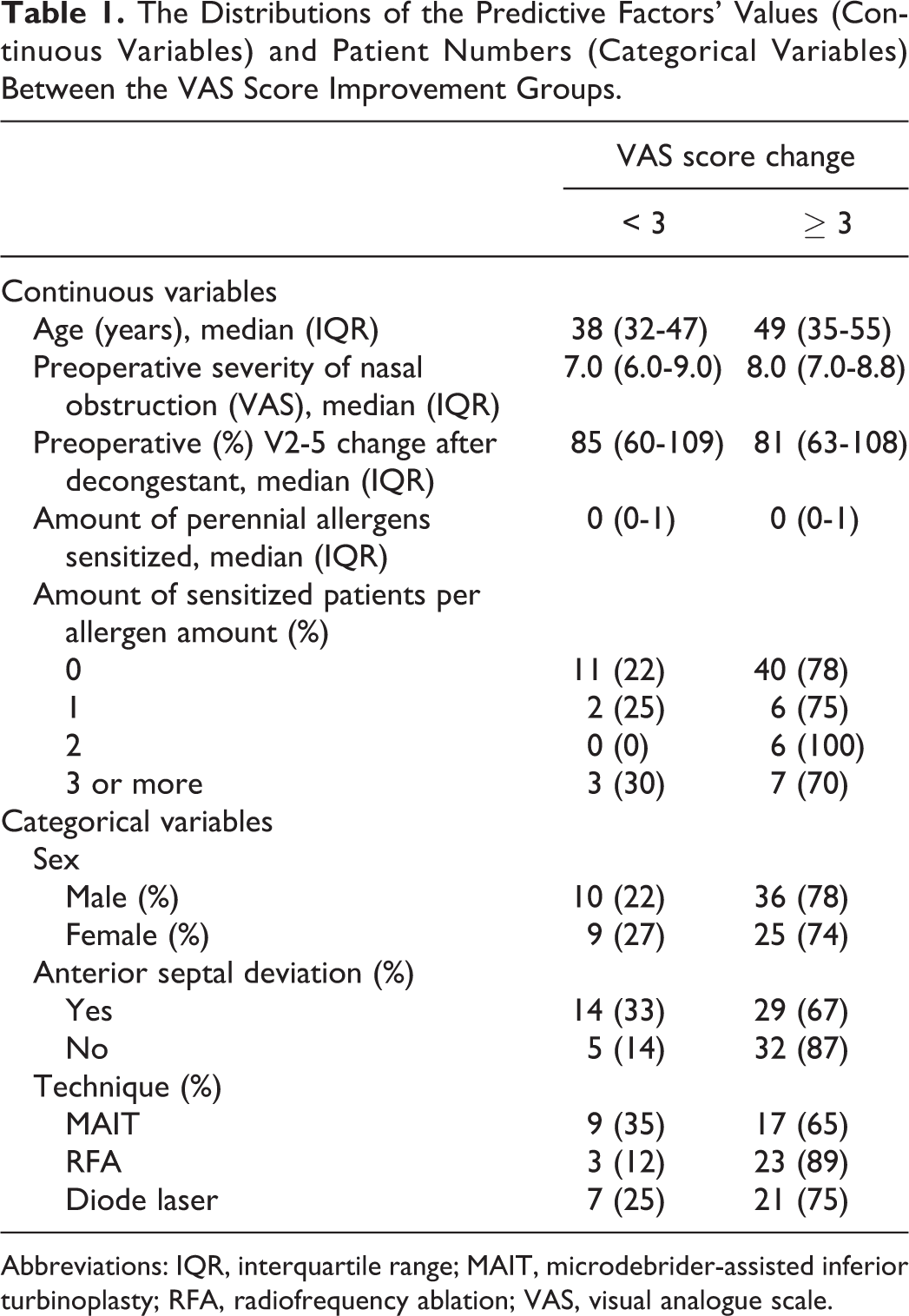
Abbreviations: IQR, interquartile range; MAIT, microdebrider-assisted inferior turbinoplasty; RFA, radiofrequency ablation; VAS, visual analogue scale.
Logistic regression models of the likelihood for an optimal subjective response to inferior turbinate surgery by precipitating factors are described in Table 2. In the multivariate analysis, patients without anterior septal deviation had a statistically significantly higher odds ratio of an optimal subjective response compared to patients with anterior septal deviation (5.6; 95% CI: 1.4-23.1; P = .02). Patients treated with RFA had a statistically significantly higher odds ratio of an optimal subjective response compared to patients treated with MAIT (9.0; 95% CI; 1.5-54.2; P = .02). Patients treated with the diode laser also had a higher likelihood of an optimal subjective response compared to patients treated with MAIT, but the finding did not achieve statistical significance (P = .07). An increase in age increased the likelihood of an optimal subjective response, and the finding was borderline regarding statistical significance (P = .06; see Table 2).
Logistic Regression Models of the Likelihood of a Satisfactory Subjective Response to Inferior Turbinate Surgery by Precipitating Factors.
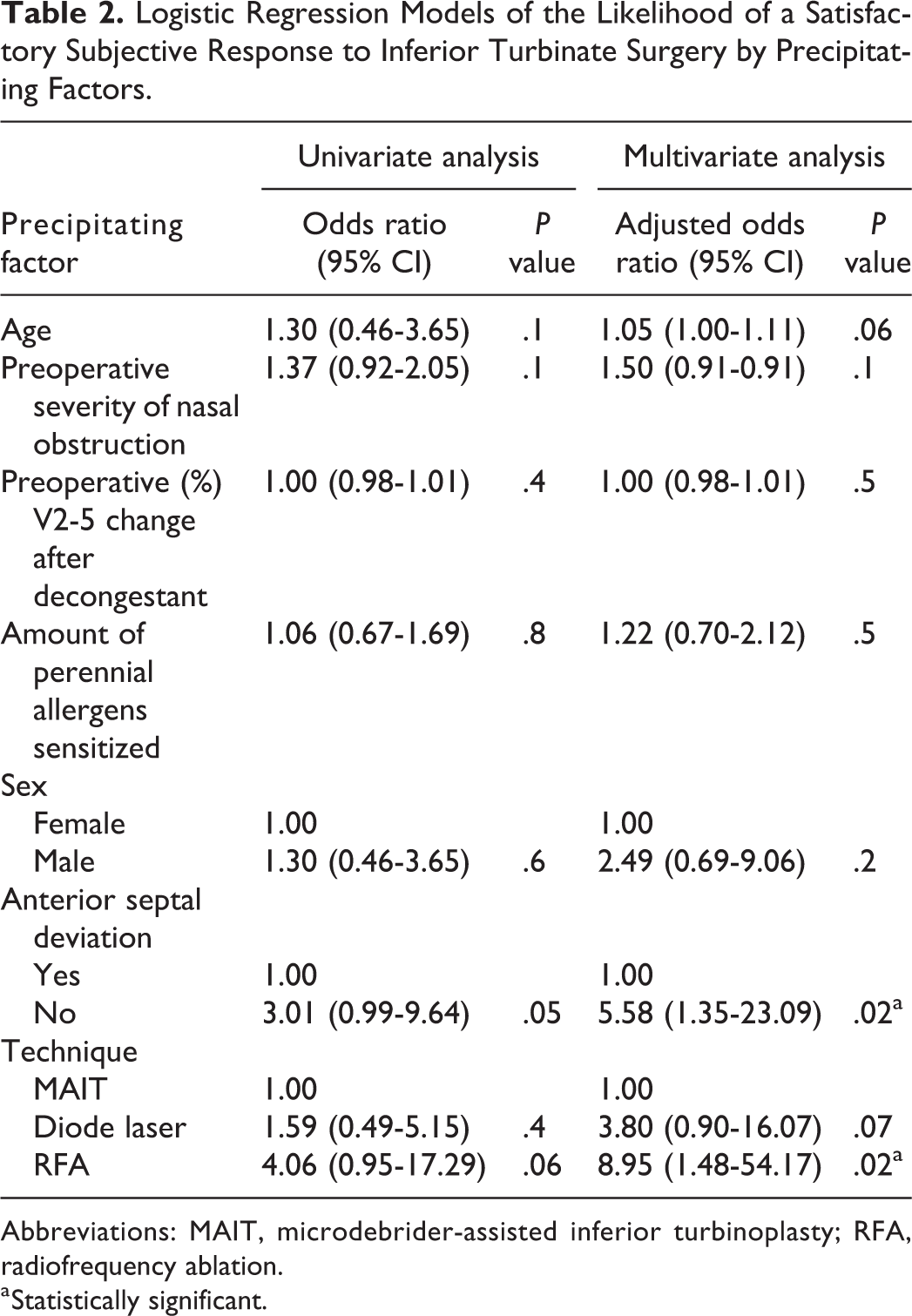
Abbreviations: MAIT, microdebrider-assisted inferior turbinoplasty; RFA, radiofrequency ablation.
a Statistically significant.
Discussion
Previously, we carried out a placebo-controlled study with a 3-month follow-up using the same study population. The RFA, diode laser, and MAIT techniques all decreased the symptom score for the severity of nasal obstruction significantly better than the placebo produce. The mean true treatment effect in the VAS score change compared to placebo was found to be −2.1 for all 3 techniques. However, the mean decrease of the symptom score in the placebo group was −2.6, which was also a significant improvement. 12 Based on this result, in the present study, we defined an optimal subjective VAS score improvement to be 3 or more.
In the previous studies, all the techniques used—RFA, diode laser, and MAIT—have been found to be both subjectively and objectively efficient in the treatment of chronic nasal obstruction in follow-ups of up to 1 year,5,13,14 and responses have been reported for even longer follow-ups of up to several years.15,16 Comparative studies of the 3 techniques that have longer follow-ups of at least 1 year are rare. In one of them, the response to RFA weakened to baseline after 1 year, while the response to MAIT was sustained for up to 3 years. 17 In another study, which combined inferior turbinate procedure with septoplasty, the response to diode laser treatment weakened after 3 months, but it was sustained in the RFA and anterior turbinoplasty groups for up to 2 years. 18
Considering the previous literature, our finding that RFA treatment had a significantly higher likelihood of an optimal subjective response compared to MAIT is rather surprising. In both the RFA and diode laser techniques, the efficacy of the treatment is based on heating the tissue, which leads to scarring and the shrinking of the submucosal turbinate tissue. In MAIT, however, the submucosal tissue is removed by a blade directly, which is more time-consuming and operator dependent. Depending on the patient’s anatomy and other circumstances, with MAIT, it may be sometimes more difficult to operate on patients homogenously when compared with the heat techniques. Therefore, some patients may benefit greatly from a MAIT operation, whereas others would benefit much less. In the anterior nasal cavity, the microdebrider can be used quite aggressively also in local anesthesia. Therefore, we think that the lack of aggressivity in using microdebrider due to local anesthesia is not the explanation of our results. On the other hand, the size of the study population is not very large, and this may influence the result. It would be interesting to see if the result would be similar with a larger study population.
Based on a recent systematic review, 19 most of the previous studies found no additional benefit of inferior turbinate surgery with septoplasty. However, in most of the previous studies, the nasal obstruction was considered to be caused mainly by septal deviation, and in many studies only the contralateral compensatorily enlarged inferior turbinate was reduced. There are also studies that have included patients with both bilateral and unilateral turbinate reduction and studies which have not reported at all whether the turbinate procedure was unilateral or bilateral.
In the present study, nasal obstruction was considered to be caused by chronic bilateral enlargement of the inferior turbinates due to chronic rhinitis. Patients with severe anterior septal deviation were excluded. A MCA value < 0.35 cm2 in the deviated side was chosen as the objective limit value for severe septal deviation. 20 However, according to the literature, nasal septal deviation may have a prevalence of up to 80%. 19 Therefore, it is understandable that most of the patients in the present study had at least some kind of septal deviation as well. The internal nasal valve in the anterior part of the nose is the narrowest part of the nasal cavity, which comprises up to 50% of the total airway resistance. 21 Even minor septal deformities in this area are likely to have critical functional importance, whereas posterior deviations only increase resistance if they are of a significant extent. Patients with anterior septal deviation have also been shown to benefit the most from septoplasty in the previous literature. 22
In our multivariate analysis, patients with no anterior septal deviation had a significantly higher likelihood of an optimal subjective response to inferior turbinate surgery compared to patients with anterior septal deviation. There are no previous reports on the effect of anterior septal deviation on the results of the inferior turbinate surgery. Based on this result, the authors recommend taking possible anterior septal deviation and concomitant septoplasty into consideration when carrying out bilateral inferior turbinate surgery procedures on patients suffering from chronic nasal obstruction due to rhinitis-based inferior turbinate enlargement to optimize the subjective response to surgery. The consideration of septoplasty is recommendable at least in clear cases of where the deviated side remains objectively narrow (MCA < 0.5 cm2) after the vasoconstriction. 23 However, further studies are needed to prove that concomitant septoplasty provides more likely the optimal subjective response than inferior turbinate surgery alone.
The preoperative topical vasoconstrictor test seems to be the most commonly examined predictive factor of inferior turbinate surgery. Jones et al treated 22 patients with submucosal diathermy. In their study, preoperative reduction in nasal resistance by the application of topical decongestant predicted a good outcome both objectively and subjectively. 6 Yilmaz et al treated 22 patients with RFA and found out that the subjective improvement of nasal obstruction due to surgery depends on how much the patient’s turbinates respond to the topical vasoconstrictor preoperatively in a 24-week follow-up. 7 In a study by Volk et al, there was a strong correlation between the presurgical effect of topical decongestion in rhinomanometry and the objective but not subjective improvement of nasal airflow by diode laser surgery in an 8-week follow-up. 8 In studies by Sabin-Yilmaz et al and Koleli et al, preoperative objective response to the decongestant showed a highly significant correlation with postoperative objective outcomes but not with subjective outcomes of RFA until 6 months postoperatively.24,25
In the present study, we chose a preoperative V2 to 5 cm change (%) after decongestant in acoustic rhinometry for the regression model. Previously, it has been shown to be a sensitive measurement for mucosal swelling during decongestion. 26 However, the degree of preoperative turbinate decongestion did not predict the optimal subjective response to the inferior turbinate procedure. This finding is in line with the previous abovementioned studies where preoperative topical decongestion did not correlate with subjective outcomes. However, the bilateral decongestion of the turbinates was one of the main inclusion criteria of the patients in the present study. We did not include patients with only a minor or no reaction to a vasoconstrictor in the study. The main idea of the vasoconstrictor test is to point out that overall there is enough chronically swollen submucosal tissue that can be operated on. This aspect and the previous results of its usefulness in predicting objective improvement support the use of the vasoconstrictor test in patient selection for inferior turbinate surgery also in the future.
There is little previous data on the predictive meaning of the patient’s subjective sensation of the severity of nasal obstruction in inferior turbinate surgery. In the study by Yilmaz et al, the success of RFA treatment did not depend on the preoperative VAS score for nasal obstruction. 7 If we look at other rhinological procedures, the subjective severity of nasal symptoms seems to have a predictive meaning in the success of the surgery. There are previous reports that show patients with more severe preoperative nasal obstruction may have a greater chance of getting higher satisfaction after septoplasty.27,28 There are also similar reports of endoscopic sinus surgery showing that more severe preoperative symptoms predict a more beneficial quality-of-life outcome after surgery.29,30
In the present study, the patients had a high preoperative VAS score for the severity of nasal obstruction. The minimum VAS score to undergo a procedure was 5. The increase of the preoperative VAS score seemed to increase the likelihood of an optimal subjective response, but the result did not achieve statistical significance. Based on this result and the previous studies of other rhinological procedures, more studies evaluating the significance of the preoperative severity of nasal obstruction as a predictive factor in inferior turbinate surgery are needed.
The effect of allergies on inferior turbinate surgery response has also been very rarely assessed. In a study by Wu et al, patients with allergic rhinitis showed less favorable subjective and objective results compared to nonallergic patients at 1 year after the MAIT procedure. 31 In our material, a notable number of the patients was sensitized to at least one allergen. Since the patients had year-round symptoms, we wanted to evaluate the meaning of sensitization to perennial allergens (mainly dust mite, cat, and dog) as a predictive factor. However, in the multivariate analysis, the amount of perennial allergens to which the patient was sensitized did not seem to have a significant meaning as a predictive factor. Further studies evaluating the significance of allergies as a predictive factor in inferior turbinate surgery are needed.
There are no previous studies of age and sex as a predictive factor in inferior turbinate surgery. In our multivariate analysis, an increase in age increased the likelihood of an optimal subjective response, and the result was borderline regarding statistical significance. Male gender also had a higher likelihood of a better response, but the result did not achieve statistical significance. More studies concerning both of these demographic predictive factors are needed.
The size of the study population was relatively small, which can be considered a weakness of the study. The intention of the study was to find the ways to optimize the subjective response for the surgery by considering various factors in the patients’ selection. The chosen limit value of the VAS score improvement was based on our previous finding regarding the placebo effect. However, the results of the study fully depend on where the limit value lies. In the lack of previous knowledge, the choice of the limit value can always be questioned. This can be considered another clear weakness of the study.
Conclusion
Anterior septal deviation seems to decrease the likelihood of an optimal subjective response to inferior turbinate surgery, thus supporting the consideration of concomitant septoplasty at least in clear cases of septal deviation to optimize the subjective response. Radiofrequency ablation treatment had a significantly higher likelihood of an optimal subjective response compared to MAIT. Further investigations regarding the findings are needed. In general, future studies of inferior turbinate surgery should concentrate more on the examination of predictive factors. This would help otorhinolaryngologists to operate on the patients who are likely to benefit optimally from inferior turbinate surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.