
Abstract
We describe an extremely rare papillary thyroid carcinoma metastasic to the paranasal sinuses and our surgical management. A 39-year-old patient with a history of papillary thyroid carcinoma diagnosed five years earlier who presented with symptoms of chronic sinusitis. Medical imaging demonstrated opacification of the frontal sinuses and the anterior ethmoid sinus without signs of angiogenesis, bone destruction or calcification. Biopsy under general anesthesia revealed presence of papillary thyroid carcinoma cells. Treatment consisted in sinus endoscopic surgery with Draf III procedure followed by 131I therapy. To our best knowledge, this is the first described case of papillary thyroid carcinoma metastatic to the frontal sinus and frontal recess.
Introduction
Papillary thyroid carcinoma (PTC) is the most frequent type of differentiated carcinoma of the thyroid1-3. Distant metastases are observed in 5 to 15% in patients with PTC1,4, with the most common sites being the lung followed by bone and brain 1 . There have been only isolated case reports of thyroid carcinomas metastatic to the paranasal sinuses (PNS)2,3,5, and most have been of follicular carcinomas5-7. The few reported cases of PTC metastasizing to the PNS have been described mostly in the maxillary sinuses2,7. We present a case of an unusual metastasis of PTC in the frontal sinuses, 5 years after primary cancer diagnosis.
Case Report
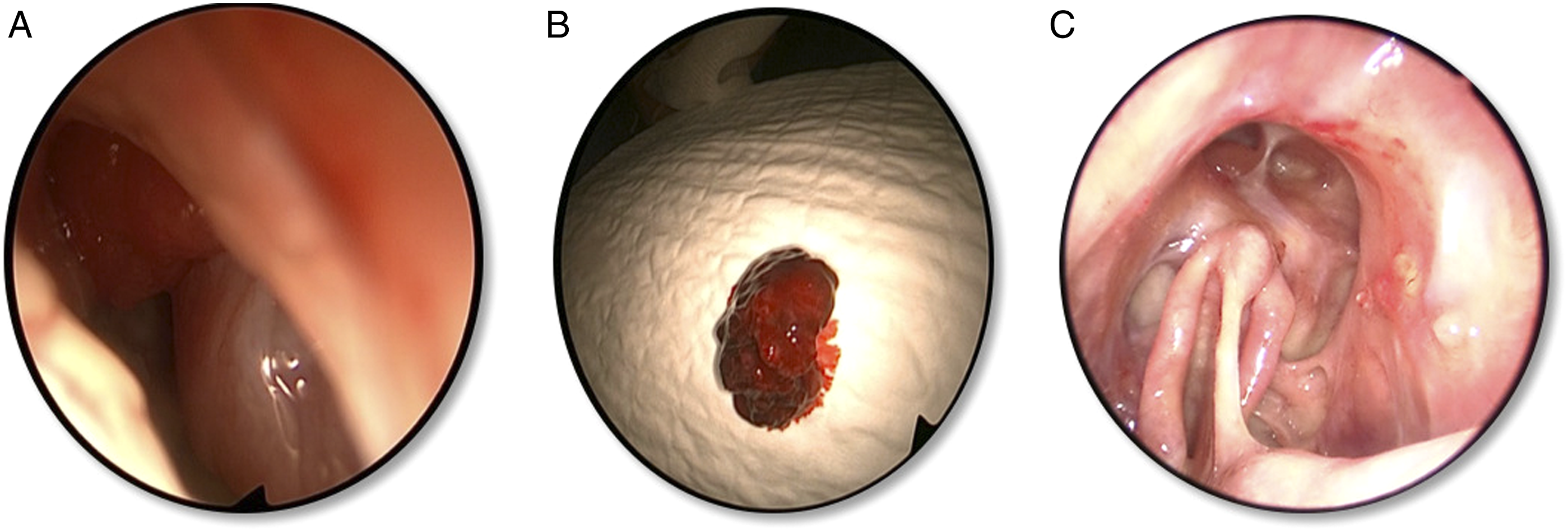
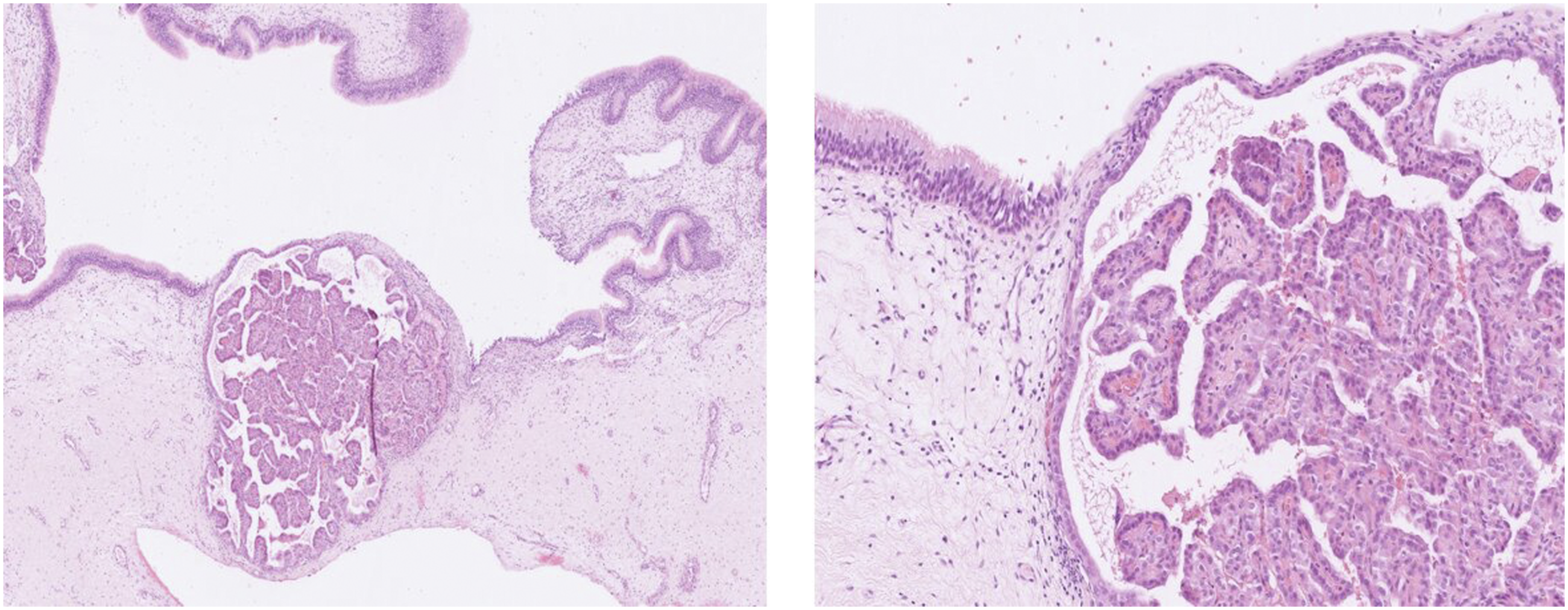
We report the case of a 39-year-old man with a history of PTC staged T3N1aM0 that was diagnosed five years earlier and treated with total thyroidectomy, 131I therapy and two neck dissections. During follow-up, he presented symptoms of headache and purulent rhinorrhea. Nasal endoscopy evidenced secretions in the right middle meatus with no signs of tumor. There was no elevation in thyroglobulin level. A cervical and facial computed tomography (CT) (Figure 1A) and a magnetic resonance imaging (MRI) (Figure 1B) showed opacification of the frontal sinuses and the anterior ethmoid sinus without signs of angiogenesis, bone destruction, or calcification. The patient underwent endoscopic sinus surgery following antibiotic therapy and local nasal treatment as there was no symptomatic improvement. After the anterior ethmoidectomy was performed, a bleeding red lesion mimicking thyroid tissue was observed in the frontal recess and biopsied (Figure 2). Histologic examination revealed papillary carcinoma (Figure 3). Diagnosis of PTC metachronous metastasis was established. A complete endoscopic resection, as decided at the multidisciplinary oncological meeting, using Draf 3 technique, was carried out. Surgery was followed by 131I therapy. The postoperative period was uneventful. The patient has been on regular follow-up until this day and no evidence of recurrence was observed (Figure 2C). .
Fragments of sinonasal mucosa infiltrated by islands of malignant cells displaying a papillary architecture. The papillae contain a thin fibro-vascular core lined by a single layer of cuboidal cells. The nuclei are enlarged and crowded, sometimes overlapping. A few nuclear grooves and pseudoinclusions can be seen. The cells express both TTF1 and PAX8.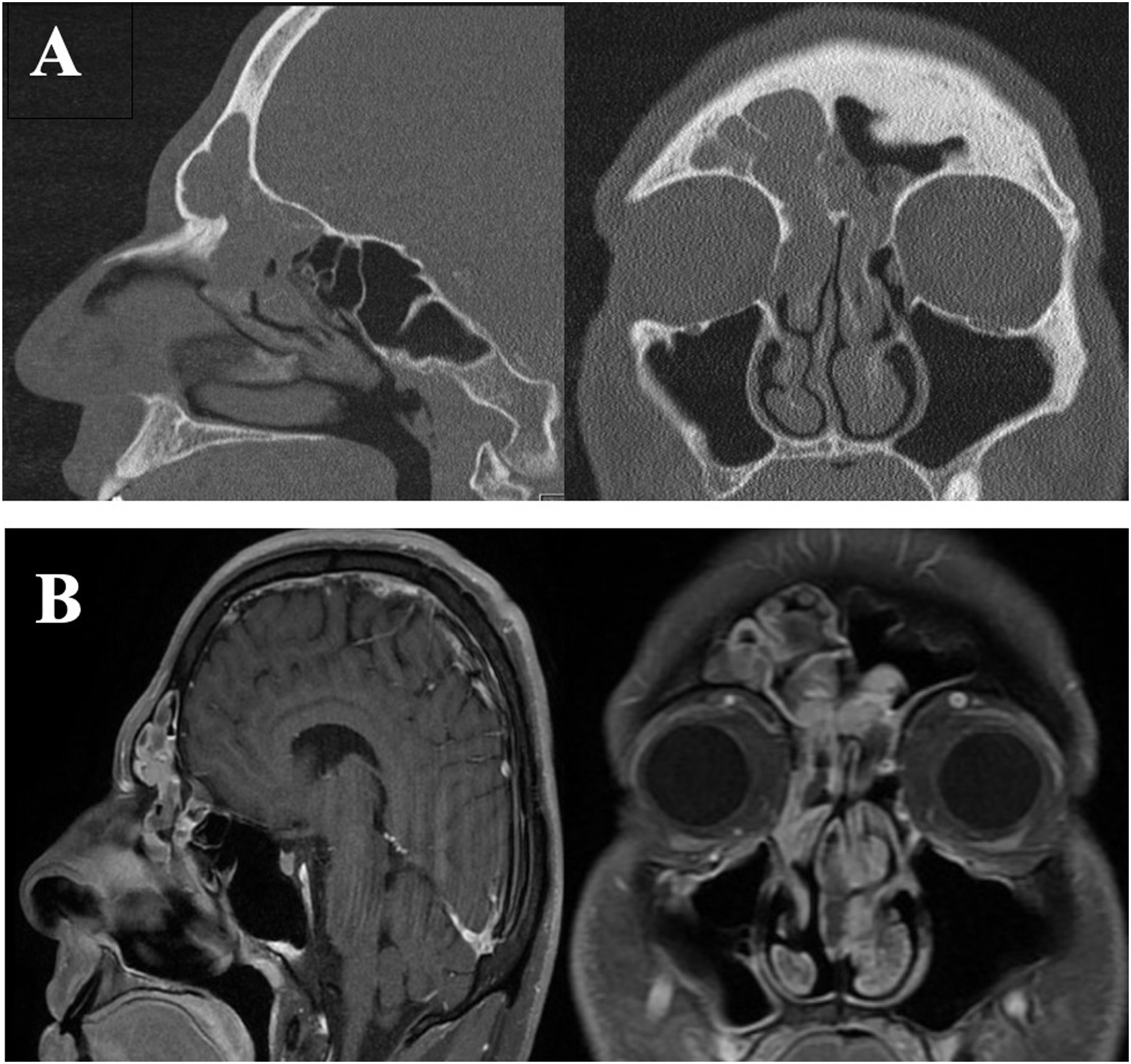
Discussion
PTC accounts for 85% of the well-differentiated thyroid carcinomas1,3. It is often slow-growing and localized. PTC has a low mortality rate (6% after 16 years of follow-up) 8 . The distant metastasis rate is 5 to 15% in patients with PTC 4 . Recurrence and cancer-related mortality risk factors are age at diagnosis, histologic type, extent of the tumor, and presence of metastases1,8. PTC often shows lymphogenous rather than hematogenous spread1,9. The lung is the most common site of distant metastases, followed by bone and brain1,4.
Cancer metastatic to the PNS is uncommon and most often originates secondarily to renal cell carcinoma and bronchogenic carcinoma7,9. The proposed route of spread is through the nonvalved vertebral venous plexus. Reflux occurs when interpleural or abdominal pressure is elevated, causing tumor cells to reach the intracranial venous plexus and finally migrate farther to the PNS 9 .
Metastasis of thyroid carcinomas to the PNS is rarely reported worldwide. There have been only isolated case reports of thyroid tumors metastatic to the paranasal sinuses (PNS)2,3,5. The commonest histology reported is follicular carcinomas5-7. The most frequently affected is the maxillary sinus followed by the sphenoid sinus2,7. In 77% of cases, metastasis is found in a single paranasal sinus lesion 6 . There are no specific symptoms but the main complaint described is intermittent epistaxis2,3.
Thyroglobulin level may serve as a good indicator to assist in monitoring of patients surgically treated for differentiated thyroid cancer. However, when thyroglobulin is undetectable, a degree of caution is advisable in the presence of thyroglobulin-antibodies 1 .
Metastasic disease in differentiated thyroid carcinoma is a poor prognosis sign and their treatment requires careful consideration, as skull base involvement is not rare, thus often making surgical treatment impossible 5 . 131I therapy is considered to be the first line of treatment for distant metastases from thyroid carcinomas1-3,5. Radical treatment by endoscopic endonasal surgery (EES) remains controversial and can be used for palliative treatment, for example, to relieve pain and control bleeding 10 . An exception is an isolated metastasis case, for which a radical ESS may be a viable option 2 . In our case, metastasis of the thyroid carcinoma was found in the frontal sinus and frontal recess without any extra-sinusal extension. Decision of the extent of resection and its surgical margin remain difficult, as there is no consensus due to limited reported cases. Our decision to perform a Draf III technique was explained by better access to the different lesions and better control during follow-up. Further investigations are required for the surgical method for treating thyroid metastatic lesions in the PNS.
Conclusion
This report describes a case of PTC metastasis to the frontal sinus and frontal recess, managed through EES surgery. To our best knowledge, it is the first case of PTC metastatic to the frontal sinus and frontal recess described within the literature. Although rare, metastases should be included in the differential diagnosis in patients with sinus lesions and a history of PTC.
Further investigations are required for the surgical treatment of thyroid metastatic lesions in the PNS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The patient gave his consent for this publication.
Data Availability
All data concerning this case report are available at the corresponding author