
Abstract
Metastatic parapharyngeal lymph nodes (LNs) from papillary thyroid carcinomas (PTC) are uncommon and can easily remain undetected. We describe a case that involves a 62-year-old woman treated for a PTC, who presented a rise in serum thyroglobulin (TG) levels. A computed tomography scan was performed, and revealed metastatic nodes in the left parapharyngeal space (PPS). A surgical resection of the nodes was performed with external cervical approach. A histological exam confirmed the diagnosis of a metastatic LN of a PTC. The aim of this report is to emphasize on the possibility of parapharyngeal metastatic nodes in PTC and to describe the diagnosis methods, treatment options, and impact on the prognosis.
Introduction
Lymph node metastases of papillary thyroid carcinoma (PTC) usually happen in the paratracheal and internal jugular chain and are unusual in the parapharyngeal space (PPS). 1 In routine, this region is not examined. As a result, LNs in this area could be left undetected. In these cases, magnetic resonance imaging (MRI), computed topography (CT), or nuclear imaging can be helpful to make the diagnosis.
The aim of this report is to emphasize on the possibility of parapharyngeal metastatic LNs in PTC and to describe the diagnosis methods, treatment options, and impact on the prognosis.
Case Report
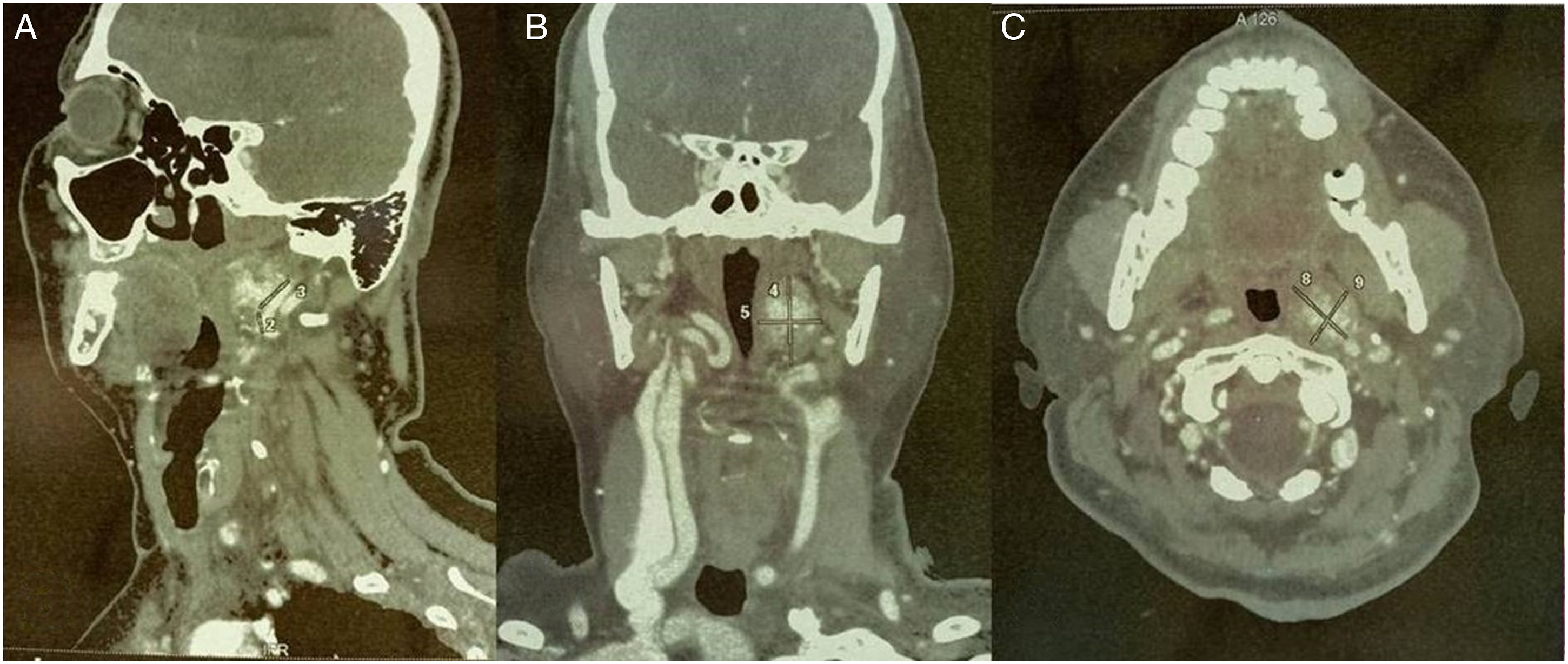
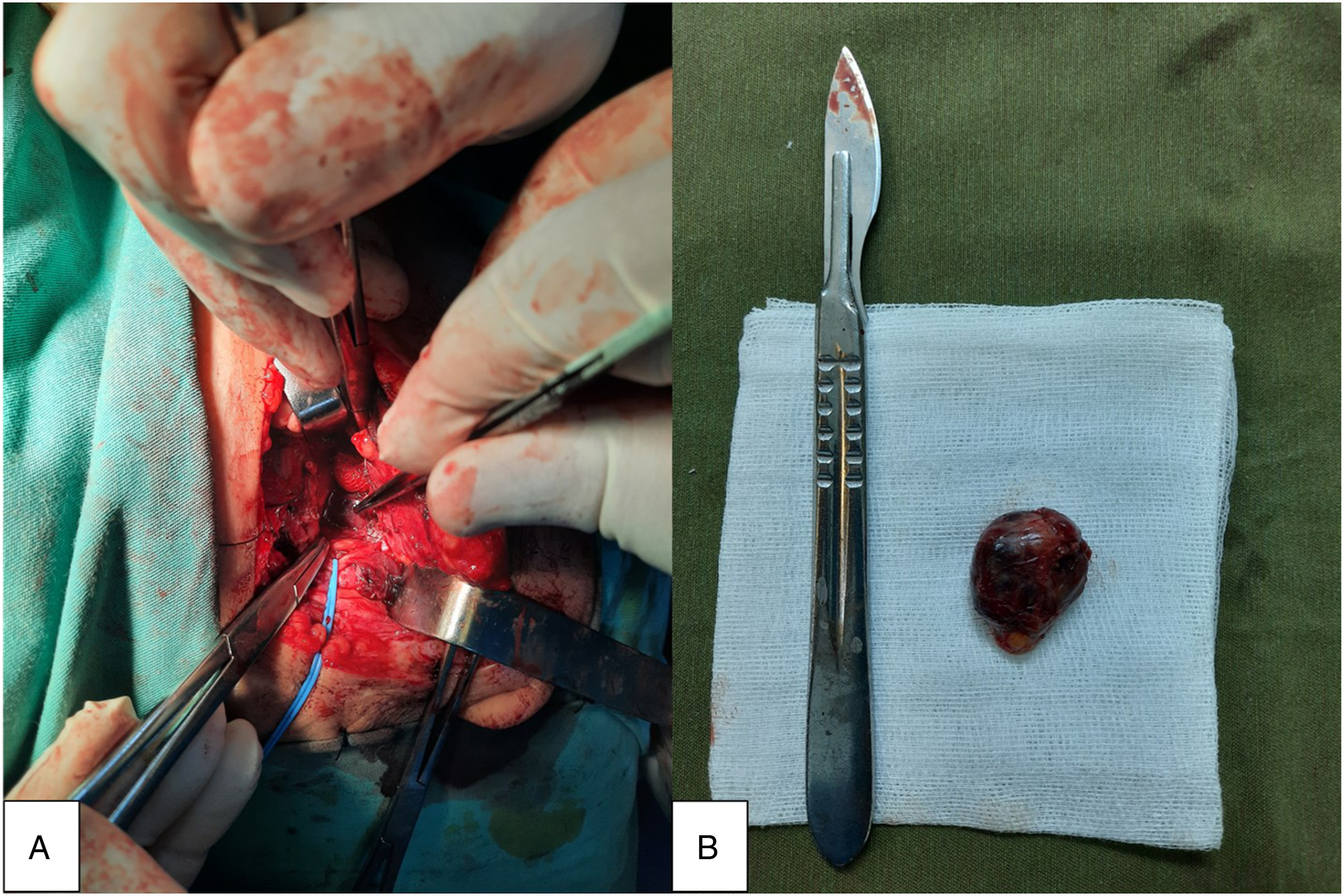
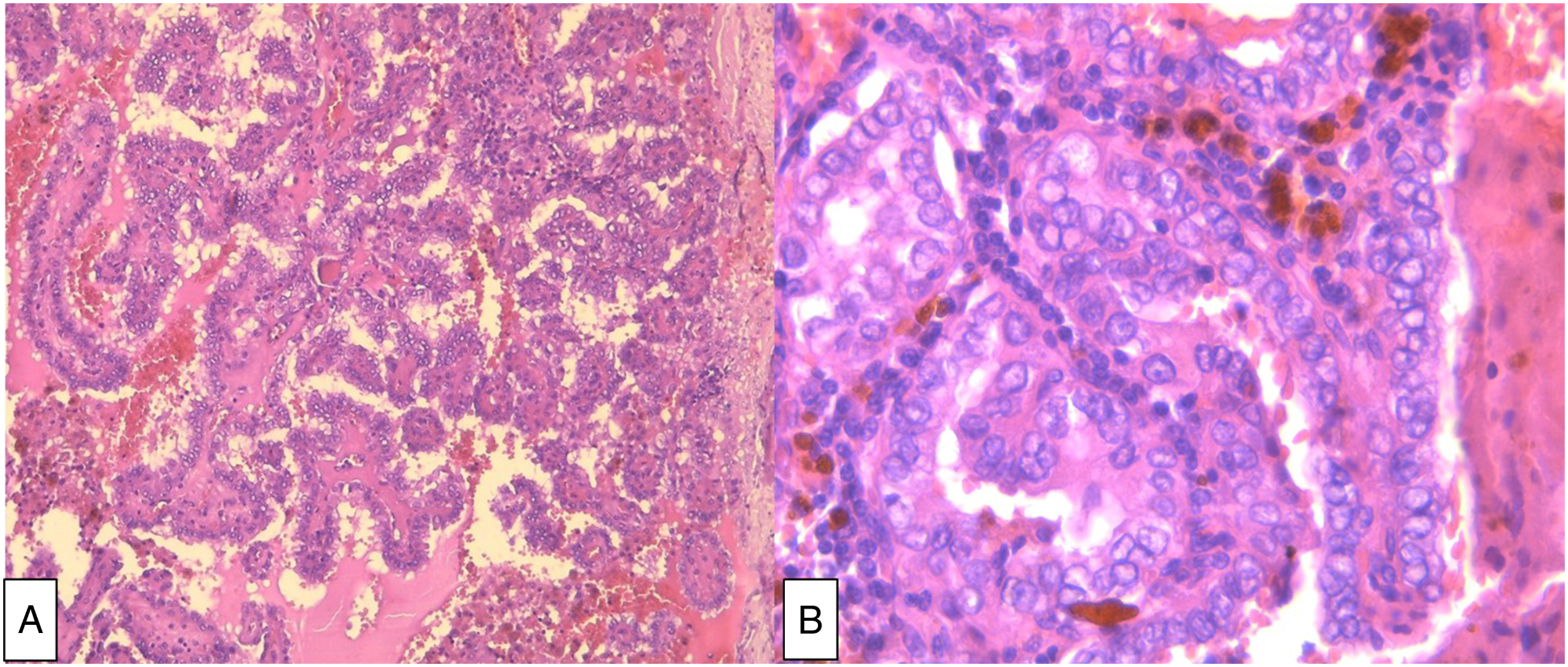
A 62-year-old woman, with no significant medical history, presented with a dysphagia evolving since 2 years. Examination revealed an anterior neck mass. On ultrasound, it was an EU-TIRADS 5 thyroid nodule, measuring 3.5 cm, occupying the totality of the left lobe. Consequently, the patient underwent a total thyroidectomy with a bilateral central dissection and a left selective neck dissection (II-IV). Extemporaneous examination suggested a PTC. Histopathologic examination of the thyroid gland confirmed the diagnosis of a 3-cm PTC of the left lobe, infiltrating the perithyroidal soft tissue, with positive surgical margins and metastasis on central and lateral LN dissections. The tumor was staged as pT2 N1b M0. Two days after the surgery, a lymphatic liquid leak occurred. It was related to an injury of the thoracic duct. The transected thoracic duct was identified and was ligated resolving further chyle leak (Figure 1). Three months postoperatively, she had radioactive iodine (RAI) ablation therapy. She received a cumulated dose of 200 mCi (2 courses). Ultrasound and thyroid scintigraphy were normal. However, because of a high thyroglobulin (TG) level, a CT scan was performed and showed a left 3--cm prestyloid mass in contact with the left internal carotid artery. The mass was hypodense, with some irregular areas of enhancement: a parapharyngeal metastatic LN was suspected (Figure 2). The patient did not present any symptom related to the mass. On physical examination, there was no evidence of cervical lymphadenopathy, no palpable thyroid lesion, no cranial nerve deficits. The oropharyngeal exam was normal. A surgical resection of the mass was performed with external cervical approach: a mass measuring 3 × 2 cm was found in the left prestyloid space (Figure 3). The patient made an uneventful postoperative recovery. He was discharged from hospital 3 days after surgery. On histopathologic examination, the mass was a metastatic LN of a PTC (Figure 4). Three months after the surgery, the patient was doing fine, with no evidence of disease. (A) Lymphatic liquid leak. (B) The white arrow shows the ligated thoracic duct. Preoperative CT scan of the neck with contrast shows a left 3-cm prestyloid mass, containing irregular areas of enhancement, in contact with the left internal carotid artery: (A) sagittal section, (B) coronal section, and (C) axial section. (A) Intraoperative view: the white arrow shows the parapharyngeal lymph node metastasis. (B) Gross appearance of the lymph node (surgical piece). Histopathologic examination of the node shows (A) papillary architecture of the proliferation (HE x 100) and (B) papillary carcinoma nuclear features of the neoplastic cells (HE x 400).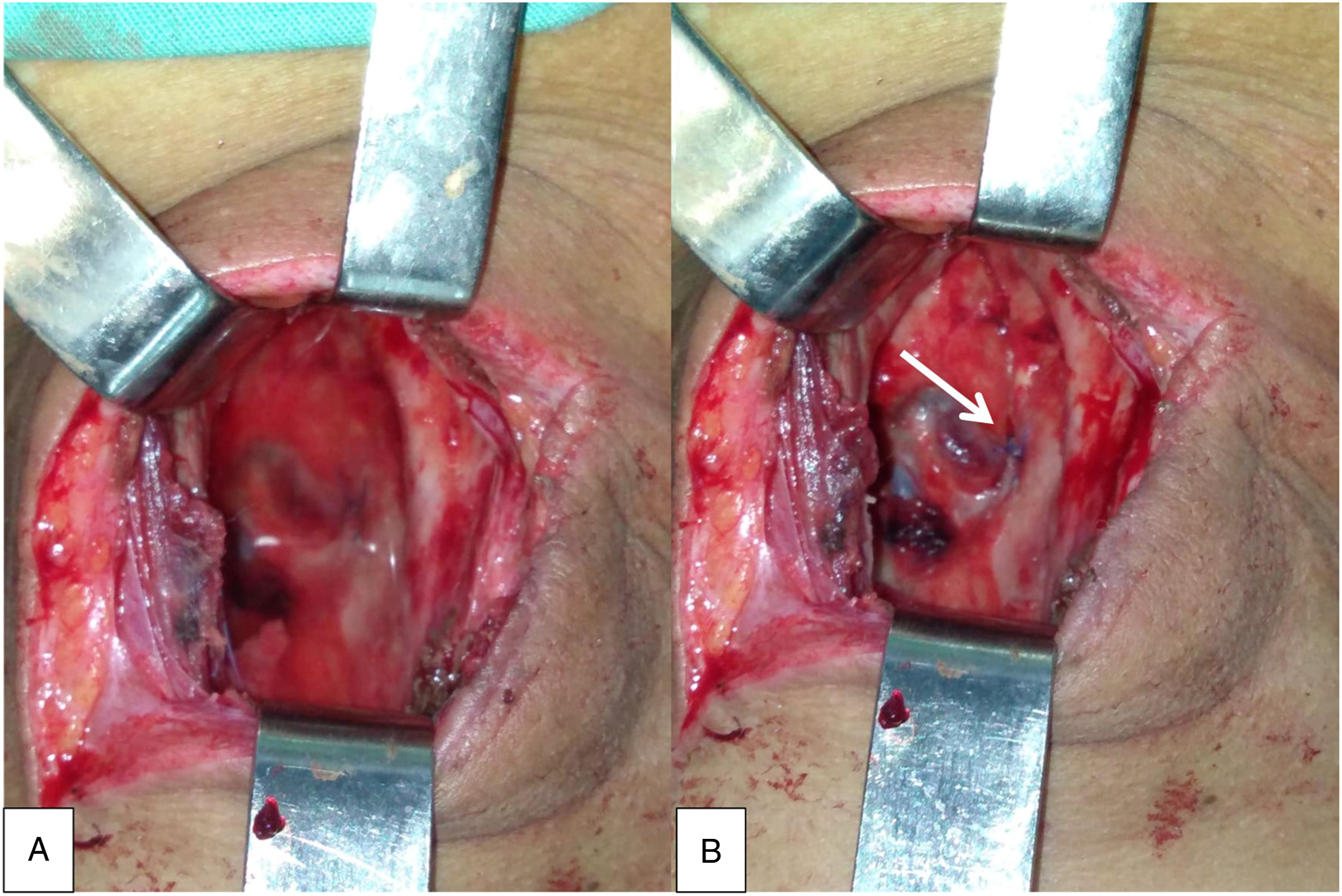
Discussion
Lymph node metastasis is frequent in patients with PTC and has been found in 20–50% of patients before initial treatment. 1 The spread of thyroid cancers usually follows a common sequence, initially to the central compartment nodes (level VI and VII) and then to the lateral compartment (level III, IV, and V). 2 Level VI may be skipped in tumors of the upper pole. 2 In these cases, cancers spread directly to the lateral neck nodes. 2
In addition to the neck region, PTC can also diffuse to ectopic locations, such as retropharyngeal, parapharyngeal, retrocarotid, sublingual, axillary, and intraparotid locations. 2 Studies have shown that .4% to 5% of patients with PTC can develop metastases in the retropharyngeal and the PPS. 3 These locations are associated with a younger age, a more aggressive disease, and a poorer prognosis. 3
A lymphatic vessel from the upper pole of the thyroid gland to the retropharyngeal lymphatic system has been described by Rouviere.1-3 It was reported in only 20% of the cases.1-3 The tumor can then spread from the retropharyngeal lymphatic system to the PPS using an anatomical dehiscence behind the fascia of the superior constrictor muscle.1-3 For the recurrent cases, the metastatic parapharyngeal LN can be the result of a retrograde lymphatic drainage due to a compression by metastatic LN or the fibrosis resulting from a neck dissection, redirecting drainage to the LN of the PPS.1,2,4 They might also be the consequence of hematogenous spread. 4 In the majority of cases, patients with metastatic LNs in the PPS had prior neck dissections rather than occult disease. 2 In our case, the route of metastasis was most likely that of a retrograde lymphatic drainage due to lateral metastatic LN, the neck dissection, or even the thoracic duct injury.
The anatomic features of the PPS make diagnosis of lesions in this site difficult. 5 The major symptoms include a painless neck mass or a globus sensation in the throat. 3 On physical examination, the predominant sign is an intraoral mass displacing the lateral oropharynx medially and a contiguous mass under the angle of the mandible. 6 Other signs include cranial nerve involvement (syndrome of Vernet), involvement of the sympathetic chain (syndrome of Horner), and involvement of the mandibular division of the trigeminal nerve. 6 Studies show that metastatic LN in the PPS cannot be diagnosed on physical examination until they reach a size of 2.5–3.0 cm. 3
Computed topography and MRI are the most frequently used imaging techniques to reach the diagnosis.3,7 The minimal size for detection of LN metastases in this area by CT/MRI is significantly smaller than the minimal size for clinical detection. 3 CT/MRI are also helpful in defining the extent of the tumor, its relationship with surrounding structures, its compartment of origin (prestyloid vs poststyloid), and might even suggest its histologic nature. 7 The tumor shows typical imaging features such as a cystic appearance and calcifications. 7 Consequently, MRI or enhanced CT of the neck should be considered in thyroidectomy patients with rising serum TG levels and normal scintigraphy, especially for patients with metastases in the lateral compartment. 1
Fine-needle aspiration biopsy and analysis of TG in a peroral fine-needle biopsy before surgery can also be an easy method for diagnosis, except for cystic metastases that can be common causes of false negatives. 8
The treatment of choice for PPS tumors is surgery. 3 Approaches for PPS surgery include the transoral, transcervical, or transcervical–transparotid approach, with or without mandibulotomy. 1 In general, the transcervical approach is the most used method because of the wide exposure allowing a more complete removal of the tumor and facilitating the dissection of the carotid artery. 3 For smaller tumors, the transoral approach can be sufficient. 3 Other methods include endoscope-assisted and transoral robotic resections. 3 Major complications of the surgery are palatal weakness, Horner’s syndrome, tongue weakness, facial nerve weakness, vocal cord paralysis, etc. 1 PPS metastatic LNs are not necessarily associated with an increased risk of LN metastases in the lateral compartment because of the presence of a direct pathway of drainage from the thyroid gland to parapharyngeal nodes. 7 Therefore, a prophylactic lateral LN dissection is not indicated. 7 After the surgery, RAI therapy can be administered in some cases of PPS metastases, while external radiotherapy is generally reserved for patients with poorly differentiated or unresectable tumors. 3
Conclusion
PPS metastases from thyroid carcinoma are uncommon, and only few cases have been reported in the medical literature. These PPS LNs are not included during nodal dissection. If these areas are left undissected, they might be the cause of a persistent disease or a delayed recurrence. 2 As a result, for patients with PTC, especially those who underwent neck dissection and have an unexplained increase in serum TG levels, CT or MRI should be done for surveillance rather than ultrasound to detect the presence of nodes in this compartment. 2
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.