
Abstract
Cherubism, a type of fibroosteodysplasia, is a rare hereditary disease that causes variable degrees of facial deformity in children. Hypertrophy of the mandible is the most common symptom, but in severe cases, the disease affects the eyes, teeth, and sinonasal cavity. There have been few reports regarding sinonasal complications and no standard treatment has been established. This paper reports long-term treatment of severe cherubism that invaded the sinonasal cavity treated with consecutive endoscopic sinonasal surgeries.
Keywords
Introduction
Cherubism is a type of congenital fibrous osteodysplasia that leads to the destruction of the jaw bone. It is a painless, non-neoplastic disease that causes symmetrical and proliferative lesions in the upper and lower jaws. It is found mainly in children between 2 and 7 years of age and progresses gradually until puberty, and then disappears partially or completely spontaneously. 1 First reported by Jones in 1933, cherubism was named because the patient was thought to resemble a cherub in Renaissance art, with a round and plump face and an upward cast of the eyes. 2 The extent of the disease and the complications vary. Dental or orbital complications are more common, but sinonasal complications have also been reported.1,3
Treatment for cherubism has not yet been established. In most cases, regular follow-up is recommended except in severe cases. However, surgery can be performed when functional or esthetic impairment is severe. 4 If complications such as upper airway obstruction, eating disorders, or tongue displacement occur, intervention is required. 5
Despite the need for an individual approach to the planning of cherubism treatment, limited data are available for the treatment and prognosis of sinonasal complications. In this case report, we report our long-term treatment experience with a child who underwent consecutive endoscopic sinonasal surgery for sinonasal invasion of severe cherubism. The course of the disease and the response to surgery of a patient from aged 6 to 17 years old in a single institution is described.
Case Report
In March 2011, a 6-year-old male patient visited the outpatient department of otorhinolaryngology. He complained of bilateral nasal breathing discomfort with snoring and purulent rhinorrhea that had gradually worsened over five months. Symmetrical and painless hypertrophy was observed on both sides of the cheekbones, maxilla, and mandible. The columella was hypotrophied compared to the alar and the nasal tip was not defined (Figure 1A). On nasal examination, the right nasal cavity was partially obstructed by septal deviation and the left side was completely blocked by a mass-like lesion (Figure 2A). The enlargement of the bilateral submandibular lymph nodes was palpable. No family members had similar symptoms. Computed tomography (CT) revealed extensive multifocal bone defects and honeycomb-like cystic lesions caused by cortical bone constriction and expansion over the mandible and maxilla. These lesions occupied both nasal cavities, paranasal sinuses, and the orbital floor (Figure 3A). We diagnosed the child with cherubism, Motamedi grade VI6 with sinonasal complications, and planned treatment. Facial appearance of the patient showing no definite resolution of facial contours over time. A, Initial appearance at age 6. B, Age 9. C, Age 13. D, Age 17. Gradually improving nasal obstructing lesion in nasal endoscope after treatment. A, Pre-surgery at age 6. B, Post-primary ESS at age 7. C, No sign of recurrence in both nasal cavity at age 17. Axial and coronal section of CT scan serial CTs. A, Preoperative expansile osteolytic cystic lesions with bulging contours occupying nasal cavity and sinonasal cavity (age 6). B, Postoperative state of ESS showed improved aeration of nasal cavity. C, Recurrence of cherubic lesion obstructing entire nasal cavity (age 9). D, Postoperative state of second ESS. E, Recurrence of intranasal lesion (age 11). F, Postoperative state of third ESS. G, Eight-year follow-up without further surgery (age 14). H, Eleven-year follow-up without further surgery (age 17) (all modified Motamedi grade VI) CT, computerized tomography; ESS, endoscopic sinonasal surgery.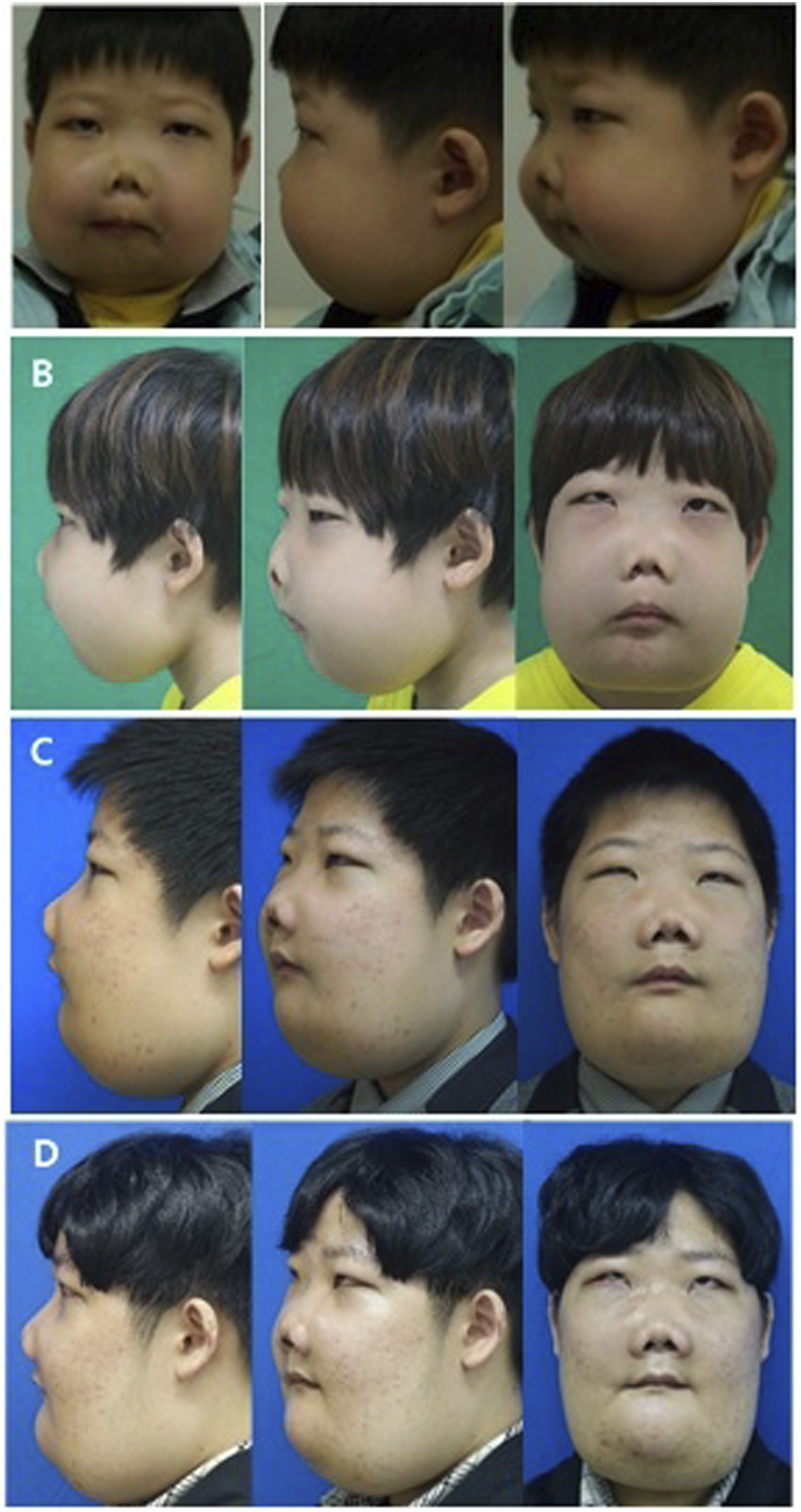
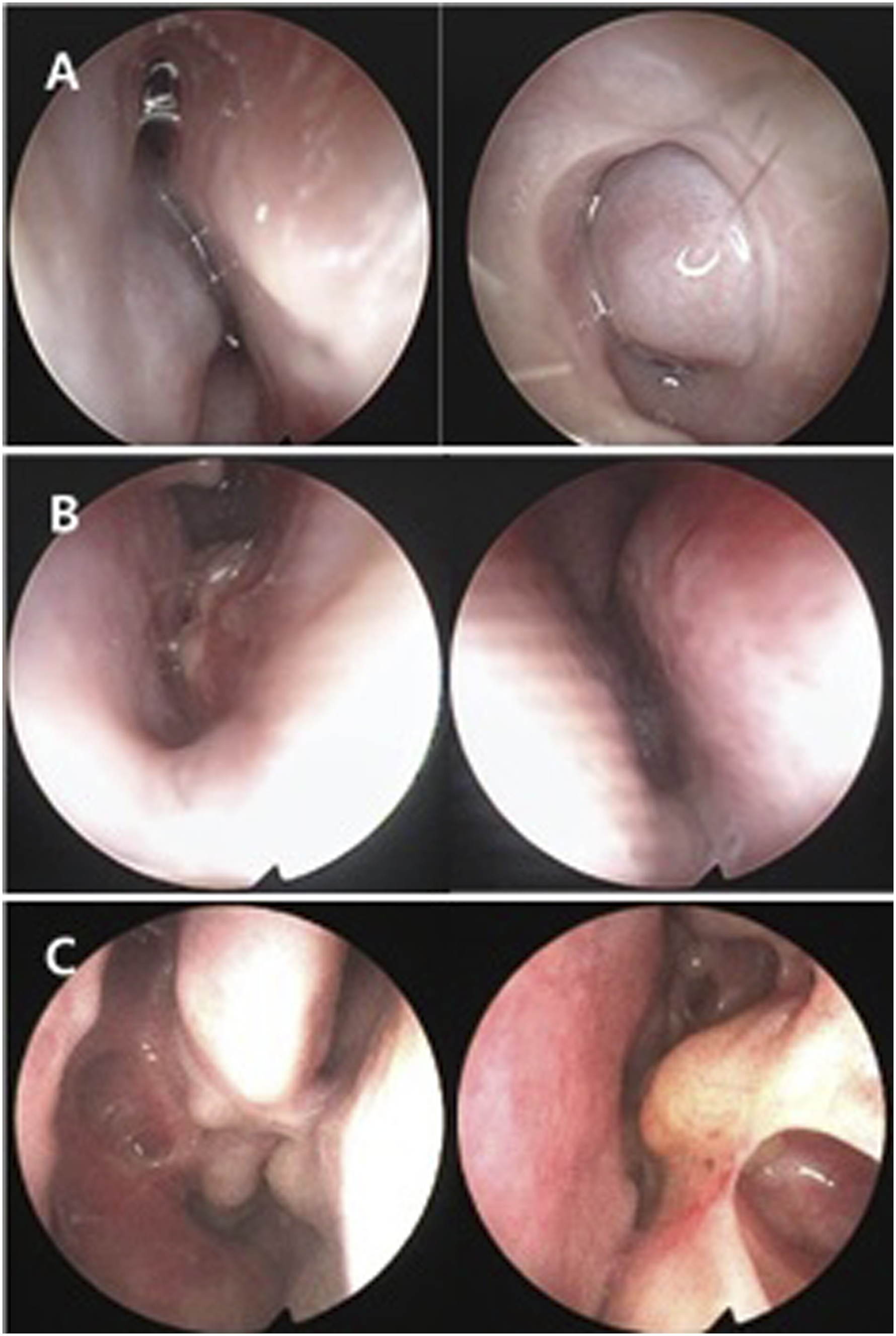
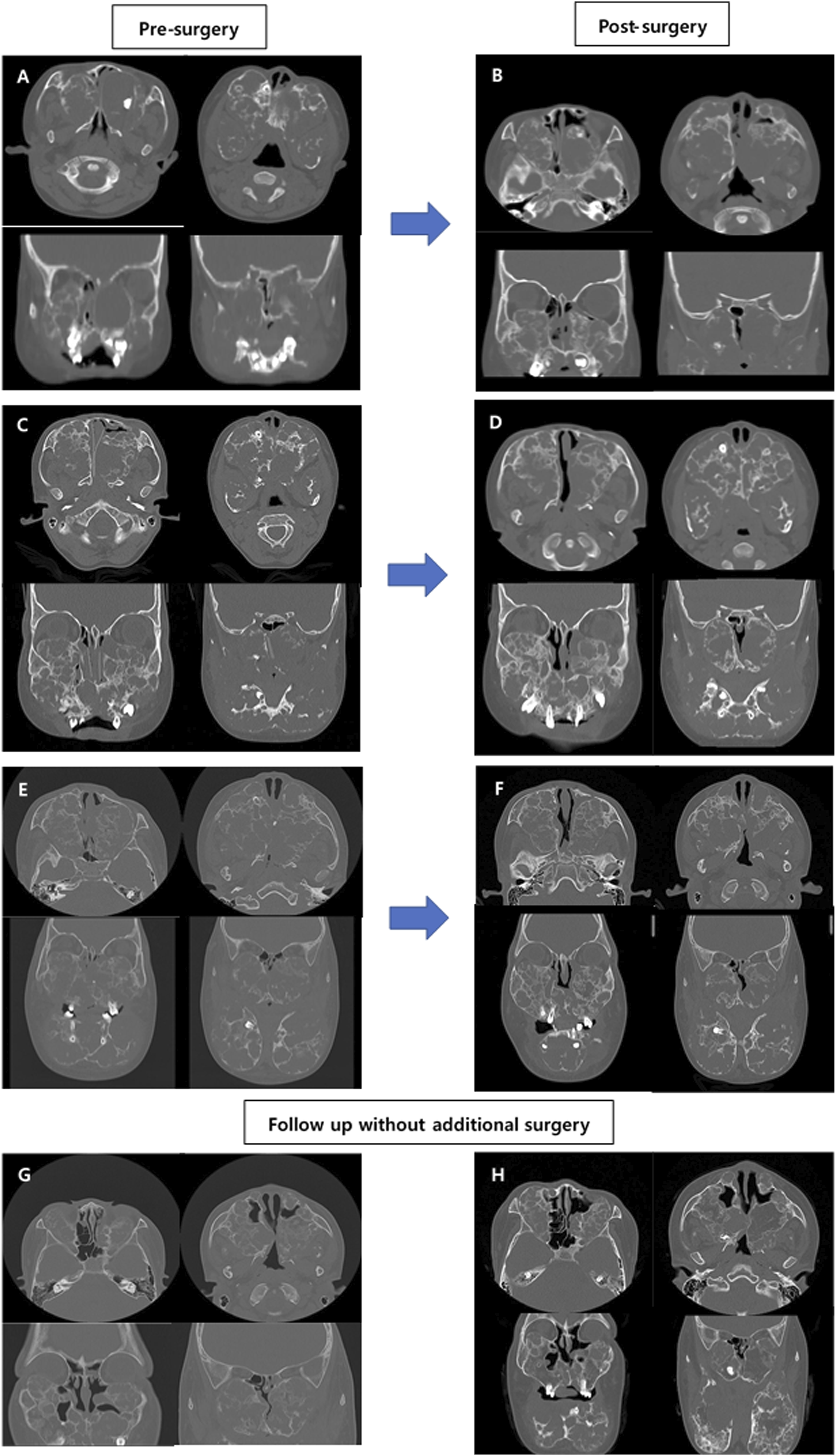
Conservative medications such as oral antihistamines or intranasal steroid spray did not relieve any of the symptoms, and the child suffered ongoing severe nasal obstruction. Parents of the child wanted aggressive treatment despite the possibility of recurrence. Therefore, we planned endoscopic sinonasal surgery to address the obstruction. We removed obstructive osseous lesions along the nasal cavity to the choana and paranasal sinuses, including the ethmoid sinus and maxillary sinus, and widened the nasal airway. A silicone tube was inserted to prevent postoperative adhesions. After three procedures of intranasal irrigation and dressing in the operating room, we removed the silicone tube. The biopsy revealed many osteoclast-like multinucleated giant cells scattered in the fibrovascular stroma along with diffuse fibroblastic proliferation (Figure 4A), which confirmed the diagnosis of cherubism. The patient’s nasal airway was widened and symptoms were relieved (Figure 2B, Figure 3B). However, recurrence occurred 6 and 18 months after the initial surgery. Further endoscopic sinonasal surgery with adenoidectomy was performed, and the silicone tube was left in place for a few years. Histopathologic slides. A, Osteoclast-like multinucleated giant cells(arrows) at age 7 (H&E, x200) and B, no abnormal giant cell identified at age 11 (H&E, x200).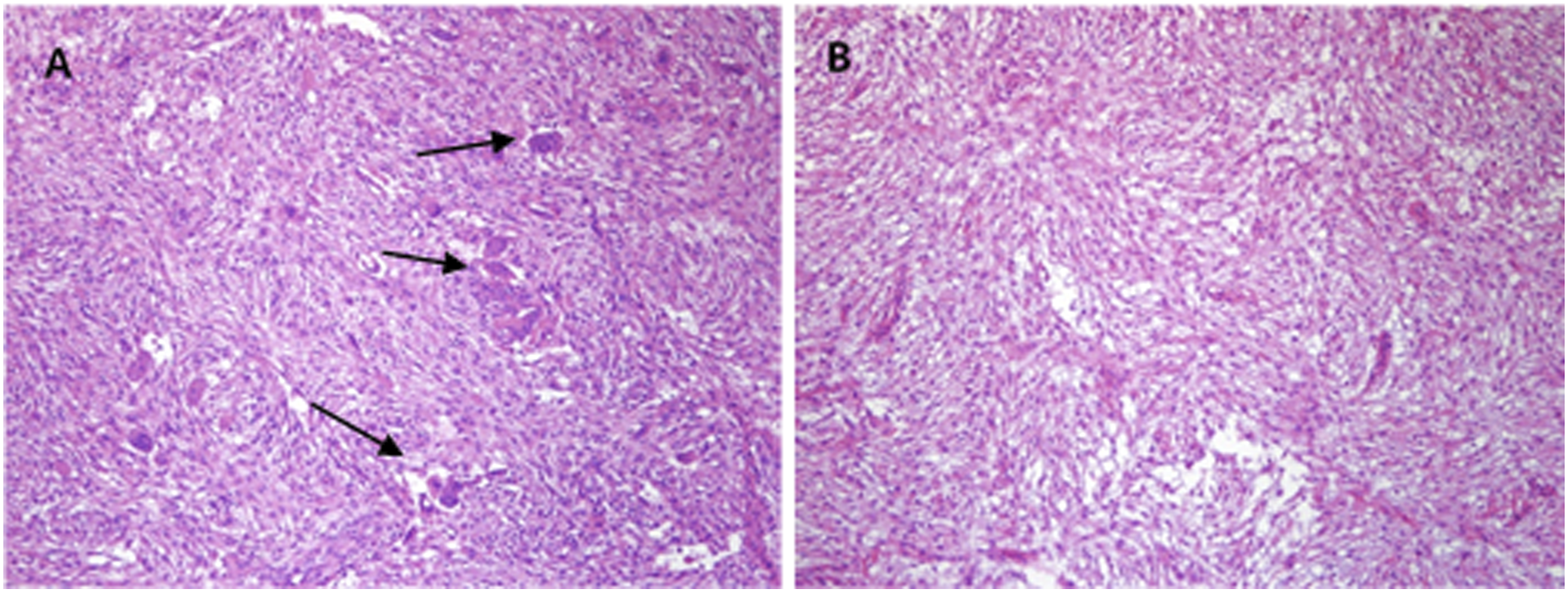
At the age of 9, the patient complained of sleep apnea with recurrent nasal obstruction due to the progression of cherubism. On polysomnography, severe obstructive sleep apnea syndrome (OSAS) was confirmed with an apnea-hypopnea index (AHI) of 74.0/hour. CT revealed further extensive osseous lesions in the mandible and maxilla compared to the initial presentation (Figure 3C). Consecutive endoscopic surgery was performed and patient symptoms resolved; aeration was observed through the nasal cavity on postoperative CT (Figure 3D).
Two years later, at 11 years of age, OSAS recurred with an AHI 40.6/hour and additional endoscopic surgery with excisional biopsy was performed. Preoperative CT (Figure 3E) and postoperative CT (Figure 3F) showed improved nasal aeration after surgery. The biopsy revealed a lower ratio of multinucleated giant cells compared to the initial specimen (Figure 4B).
Symptoms of nasal obstruction, OSAS, and chronic sinusitis progressed during outpatient follow-up without further intervention. At 14 years of age, polysomnography improved to an AHI of 0.5/hour. On serial CT (Figure 3G, Figure 3H) and nasal endoscopy (Figure 2C), aeration of the nasal cavity and paranasal sinuses was greatly improved. However, unlike the improvement in rhinosinus manifestations of cherubism, severe osteolytic lesions in the mandible and maxilla did not show any regression, consistent with Motamedi grade VI and facial hypertrophy (Figure 1D).
During follow-up, the patient did not undergo any other treatment for cherubism except levator resection for ptosis, and did not complain of any other severe complications except for the esthetic appearance of the facial contours. Despite the invasion of the orbital floor with cherubism, he had normal visual acuity.
Discussion
Cherubism is a rare benign fibrous bone disease of the maxilla and mandible and only about 300 cases have been reported in the literature. 7 It is an autosomal dominant genetic disorder, which is why it is also called familial fibrodysplasia. The genetic penetration rate is reported to be 100% for men and 50 to 70% for women, but cases without a family history have also been reported.8,9
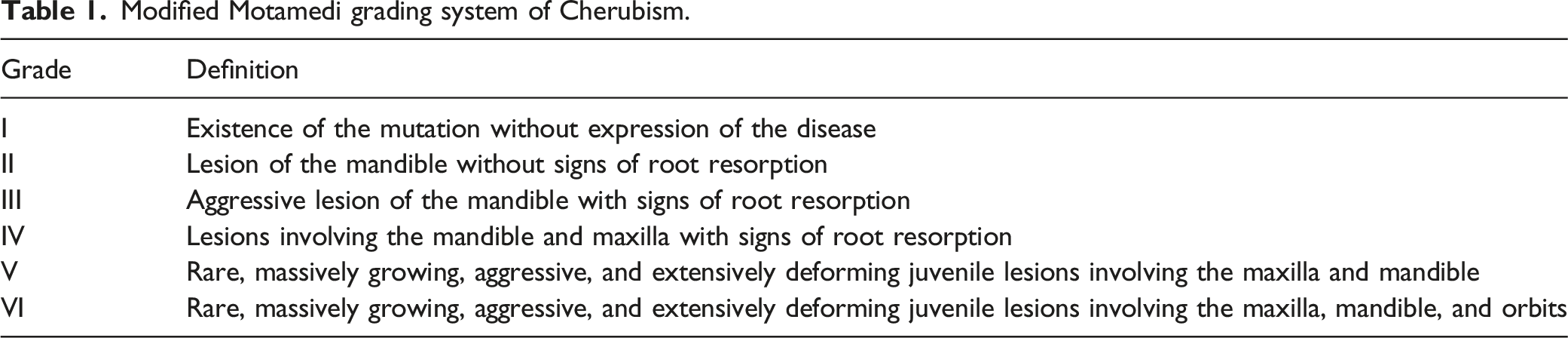
Modified Motamedi grading system of Cherubism.
Radiologically, cherubic lesions appear as bilateral, multilocular radiolucent cystic lesions with unclear boundaries, and the cortical bone is shriveled and swollen. Unerupted impacted teeth and displaced teeth can also be observed. Histologically, bone tissue is replaced with a fibrous matrix and multinucleated giant cells similar to osteoclasts are irregularly distributed. A well-formed vascular channel and the presence of eosinophils and collagenous substances around the capillaries are important findings when diagnosing cherubism. More dense fibrotic tissue and reduced multinucleated giant cells are seen in mature lesions. Differential diagnosis should include central giant cell granuloma, osteitis fibrosa cystica, giant cell tumor, and ossifying fibroma.14-17
There is still no standardized treatment for cherubism. 16 In cases with a mild phenotype, it has been reported that after puberty, lesions do not progress and spontaneous recovery occurs due to the self-limiting nature of bone growth. Therefore, periodic monitoring is recommended through radiographic imaging every year until puberty. However, surgical intervention can also be considered before puberty if there are functional difficulties due to dental, ocular, or respiratory complications during growth or severe facial deformities. 18 Treatment should be approached individually in each case. It is crucial to analyze clinical behavior to determine the most appropriate time and type of treatment. 5
The result of the surgical outcomes has varied. Some studies did not recommend facial contouring surgery during the growth period as it can accelerate lesion progression by stimulating fibroblasts and osteoclasts.19,20 Another study also opposed surgery due to the high growth potential of cherubism and the difficulty of total resection of pathological tissue. 21 Early intervention in children was prone to recurrence and the prognosis was poor.22,23
In contrast to this, Dukart et al. 24 argued that osteotomy and surgical curettage could inhibit active growth of lesions and promote bone remodeling during the rapid growth phase. Kaugars et al. 14 mentioned that intraosseous curettage with contour plastic surgery promoted recovery to clinical and radiological normality. Raposo et al. reported no recurrence after extensive resection in eight cases. 25 Several studies have supported the advantages of surgical intervention in severe cherubism.26-28
Although non-invasive continuous positive airway pressure could be considered in severe OSAS, sinonasal surgery can also be an alternative, especially in patients with craniofacial abnormalities with nasal obstruction. It effectively improves respiratory disorders by maintaining the nasal airway. 29
There is controversy regarding various treatment methods for cherubism considering the patient's age, disease progression, and functional impairment. To the best of our knowledge, this is the first study to report the long-term prognosis of endoscopic sinus surgery for sinonasal complications of severe cherubism. In this case, the child had severe functional impairment of the nasal cavity due to the invasion of an osseous lesion related to severe cherubism (Motamedi grade VI). He underwent endoscopic sinonasal surgery and nasal and sinus aeration was maintained, reducing sinonasal complications such as chronic sinusitis and OSAS.
The improvement in this case can also be attributed to the self-limiting nature of cherubism. However, extensive lesions along the mandible and maxilla persisted at grade VI during the same period when sinonasal function was significantly improved. This supports the idea that surgical intervention might inhibit the active growth of cherubism. However, when surgery is considered in early childhood, several consecutive surgeries should be considered until progression of the osseous lesions slows.
Footnotes
Declaration of Conflicts of Interest
The authors have no potential conflicts of interest to declare with respect to the research, authorship, and publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea(NRF) grant funded by the Korea government(MSIT) (No. 2022R1F1A1071824) to J.M.L.
Informed Consent
Written informed consent approved in advance by the IRB was obtained from the patient for the publication of this case report and any accompanying images (IRB File No. ISPAIK 2022-07-012-001).
Data Availability
All relevant data are within the article.