
Abstract
Objectives:
Neurilemmoma in the nasal cavity and paranasal sinuses is very rare. The study aimed to improve the understanding of neurilemmoma in the nasal cavity and paranasal sinuses.
Materials and Methods:
The clinical data of 10 patients with neurilemmoma in the nasal cavity and paranasal sinuses treated from January 2014 to June 2019 in our hospital were retrospectively studied.
Results:
There were 6 females and 4 males patients in our study. The mean age was 49.5 years (range 37-77 years), and the most common clinical symptom was unilateral nasal obstruction. The site of tumor included the nasal cavity, maxillary sinus, ethmoid sinus, and sphenoid sinus. There were 2 cases with malignant neurilemmoma. Nine patients underwent functional endoscopic sinus surgery (FESS); however, 1 patient underwent FESS combined with the lateral rhinotomy for complete resection of the tumor. Two patients with malignant neurilemmoma received postoperative radiotherapy. The mean follow-up was 3.82 years (range 2-7 years). There were no incidences of tumor recurrence during the study period.
Conclusions:
Neurilemmoma in the nasal cavity and paranasal sinuses is a mainly benign tumor. Complete surgical excision by FESS is the only treatment option for neurilemmoma in the nasal cavity and paranasal sinuses; while malignant neurilemmoma needs postoperative radiotherapy.
1. How was the determination of malignant neurilemmoma made?
The diagnosis of malignant schwannoma is mainly dependent on histopathological examination because of its atypical clinical symptoms and lack of specific imaging manifestations. Immunohistochemical examination is still needed to assist diagnosis when it is difficult to distinguish between benign and malignant tumor. In our study, the histopathological examination combined with immunohistochemical examination showed that 2 cases were malignant neurilemmomas.
2. One of the cases of malignant neurilemmoma required a lateral rhinotomy—was that necessary to obtain clear margins?
One of the malignant neurilemmomas or schwannomas required functional endoscopic sinus surgery (FESS) combined with the lateral rhinotomy. Because of the wide range of the tumor in this case, FESS combined with the lateral rhinotomy was needed to completely remove the tumor. Moreover, complete surgical resection with wide negative margins is the current standard of care for localized high-grade MPNST (malignant peripheral nerve sheath tumor) and is a strong predictor of survival. Specifically, it is recommended that tumors should be excised with wide margins.
3. The other malignant neurilemmoma was in the sphenoid and one presenting symptom was facial numbness—was there any consideration for postoperative radiation?
Patients with malignant neurilemmomas or schwannomas need postoperative radiotherapy, because postoperative radiotherapy can reduce the local recurrence rate and prolong overall survival. When malignant neurilemmoma or schwannoma involves the nerve, it is necessary to remove the nerve at the same time for the purpose of complete resection of the tumor, which may cause neurological dysfunction, so postoperative radiotherapy is required.
Introduction
Neurilemmomas or Schwannomas are mainly benign tumors derived from Schwann cells of the nerve sheath and occur in all parts of the body. Previous studies have shown that neurilemmoma is the most common benign nerve sheath tumor of the head and neck (approximately 25%∼45%); however the nasal cavity and paranasal sinuses are rarely involved, only less than 4% are found in the nasal cavity and paranasal sinuses. 1,2 Because of their rarity and nonspecific symptoms, it is difficult to have a precise preoperative diagnosis. We retrospectively analyzed the clinical data of 10 patients admitted to our hospital and reviewed the relevant literature to improve the understanding of neurilemmomas in the nasal cavity and paranasal sinuses.
Materials and Methods
A retrospective study was performed on 10 patients with neurilemmoma in the nasal cavity and paranasal sinuses diagnosed in our hospital during January 2014 and June 2019. All the patients were examined by paranasal sinus computed tomography (CT) and magnetic resonance imaging examination. The final diagnosis was confirmed by histopathological examination and immunohistochemistry. The study was approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University, and all patients signed an informed consent form.
Results
The clinical characteristics of these patients were depicted in Table 1. There were 6 females and 4 males among 10 patients. The mean age was 49.5 years (range 37-77 years), and the history of these patients was from 1 month to more than 10 years. The most common clinical symptom was unilateral nasal obstruction. Other clinical symptoms included rhinorrhea, headache, exophthalmos, and facial numbness. The site of tumor included the nasal cavity, maxillary sinus, ethmoid sinus, and sphenoid sinus. Paranasal sinus CT imaging showed a soft tissue mass, and some might be accompanied by adjacent bone destruction (Figure 1A and B). Magnetic resonance imaging revealed that the tumor usually had an isointense or slightly hypointense intensity on T1-weighted images and moderately hyperintense intensity on T2-weighted signals (Figure 2A and B). The tumor enhances with gadolinium contrast. Nine patients underwent functional endoscopic sinus surgery (FESS); however, 1 patient underwent FESS combined with the lateral rhinotomy for complete resection of the tumor. Two patients with malignant neurilemmoma received postoperative radiotherapy. The histopathological examination showed that the tumor cells were spindle cells (Figure 3), and the histopathological examination combined with immunohistochemical examination showed that 2 cases were malignant neurilemmomas. Immunohistochemical results showed that the spindle cells were positive for S-100 protein, and negative for epithelial membrane antigen (EMA) and desmin. The mean follow-up was 3.82 years (range 2-7 years). There were no incidences of tumor recurrence during the study period.
Clinical Characteristics of 10 Cases.
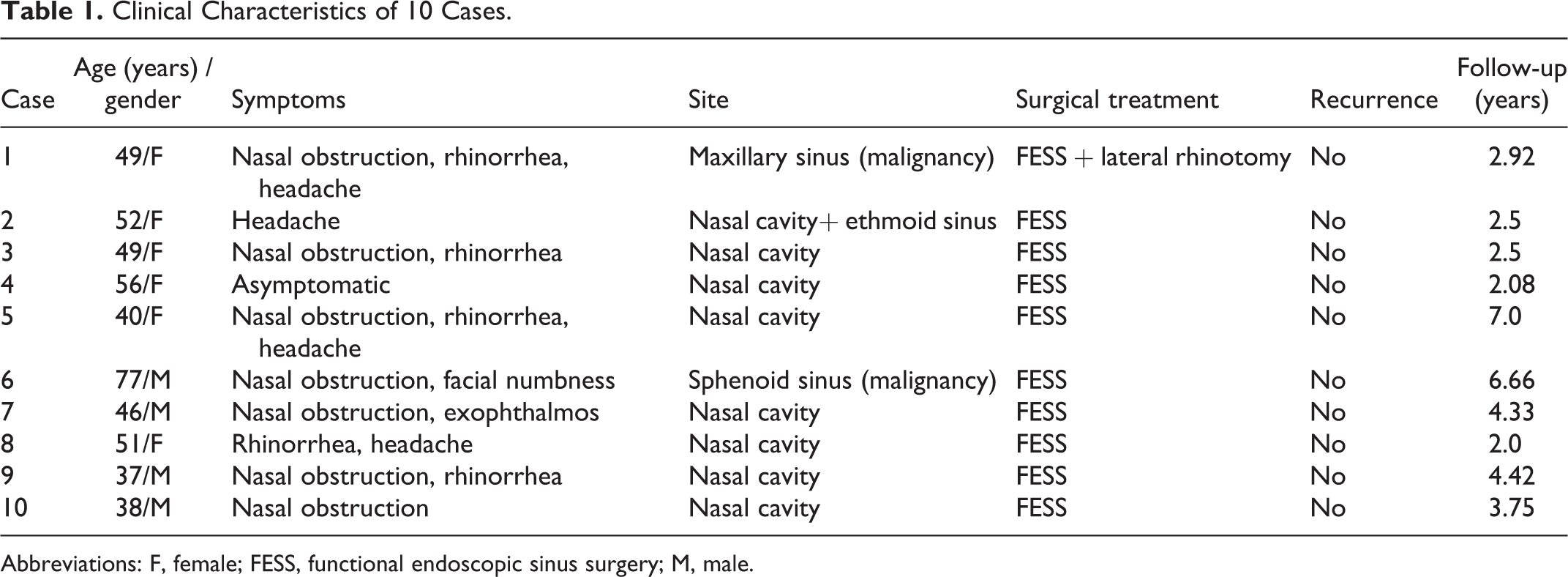
Abbreviations: F, female; FESS, functional endoscopic sinus surgery; M, male.
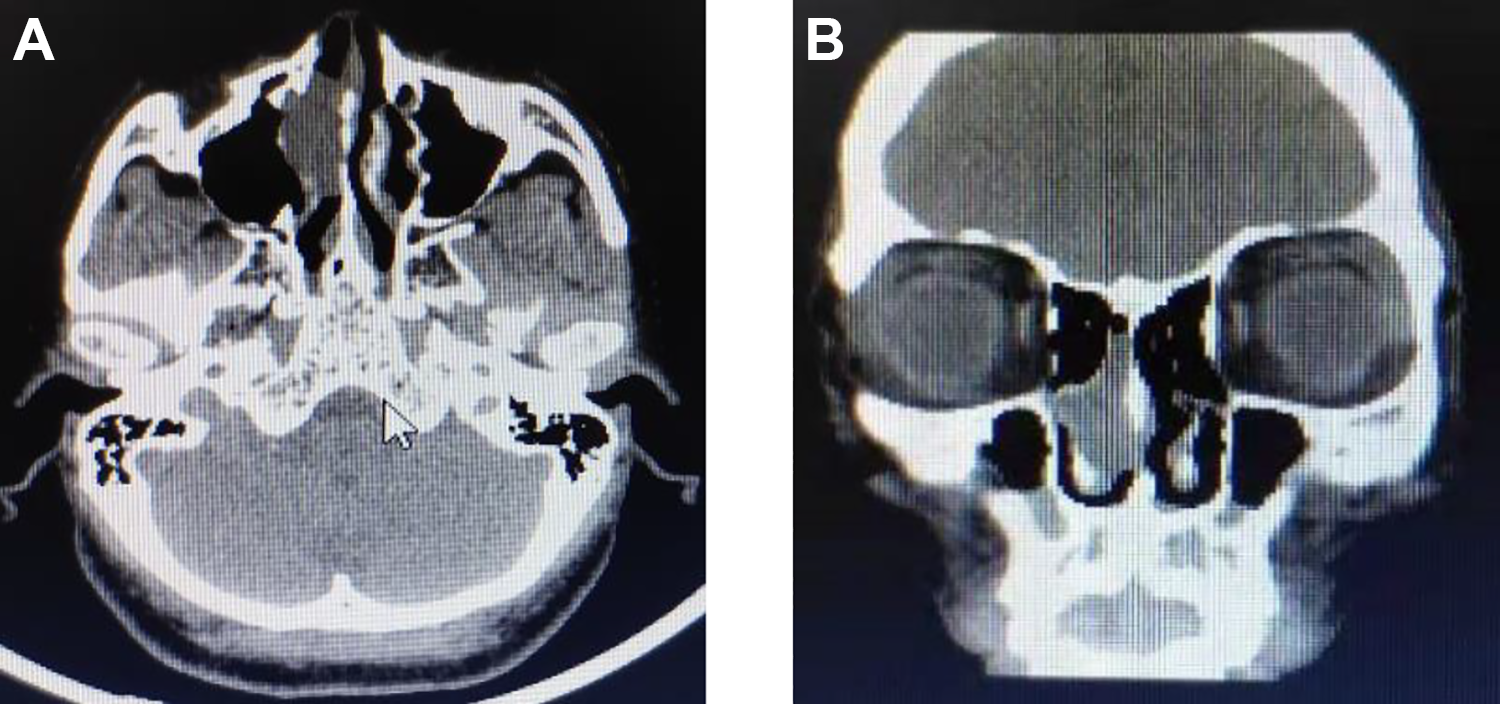
A and B, A CT scan of the paranasal sinus shows a soft-tissue mass in the right nasal cavity. CT indicates computed tomography.
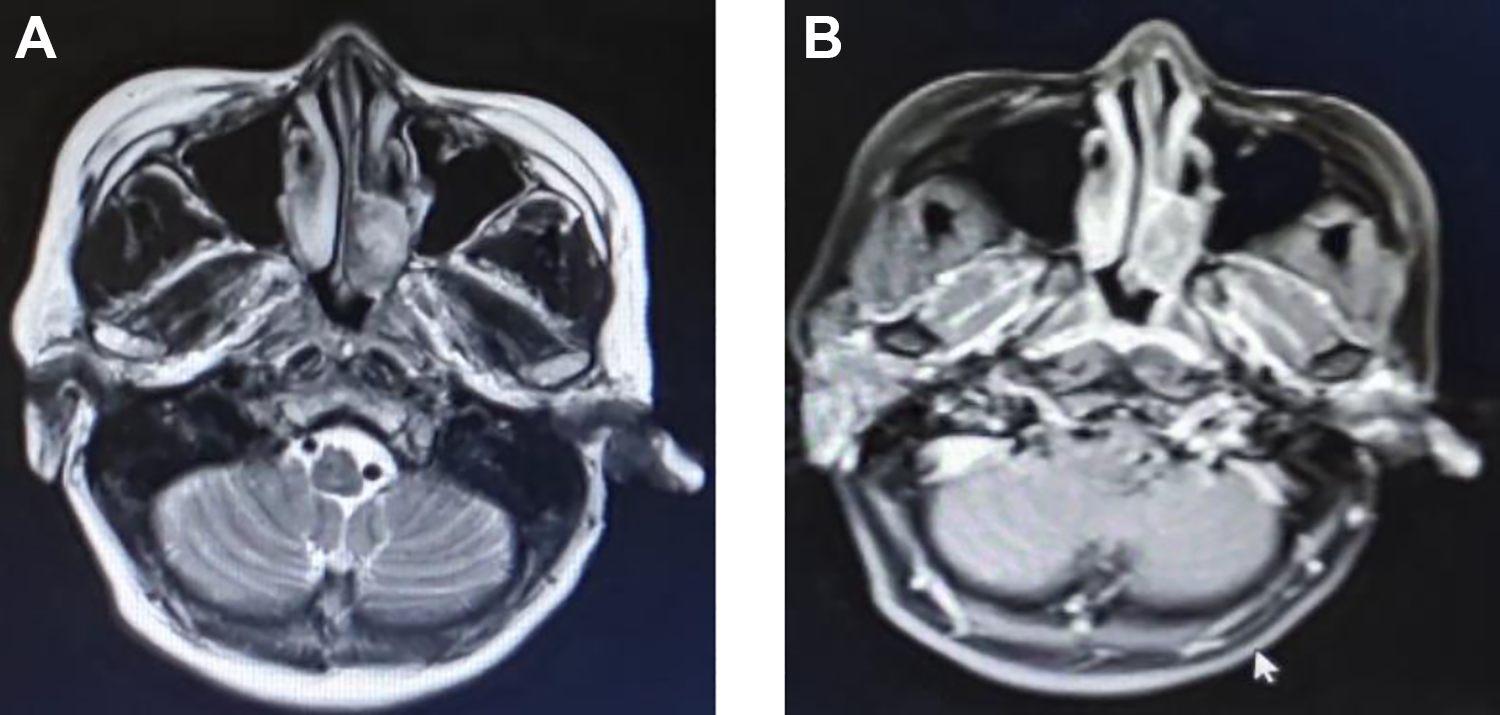
A and B, An MRI of the paranasal sinus shows a mass in the left nasal cavity and ethmoid sinus, and the mass inhomogeneously enhances with gadolinium contrast. MRI indicates magnetic resonance imaging.
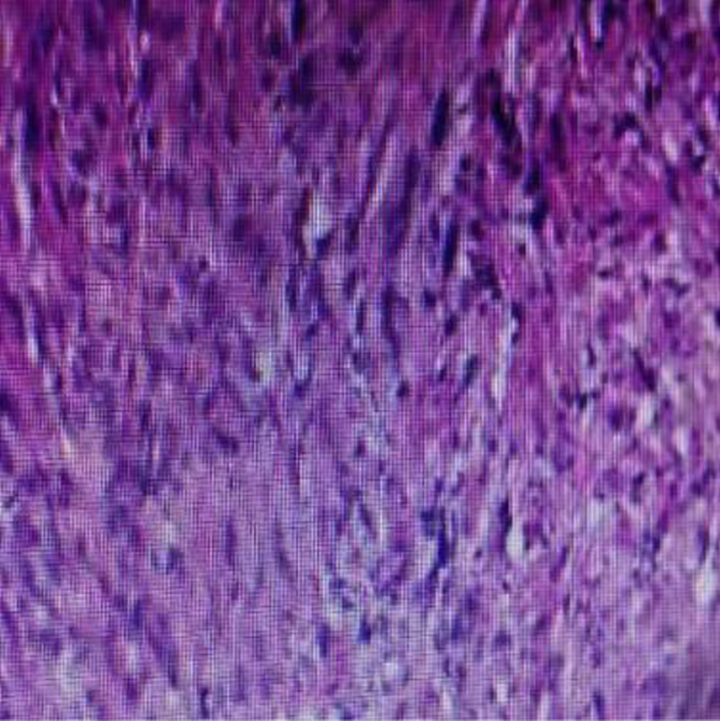
A histopathological examination of the nasal cavity and paranasal sinus neurilemmoma reveals numerous spindle cells (HE, original magnification ×200).
Discussion
Neurilemmomas or Schwannomas are predominantly benign tumors deriving from Schwann cells of the nerve sheath, and the relevant literature only contains isolated cases of malignant neurilemmoma, which accounts for 5% to 10% of the total neurilemmomas. Approximately 25% to 45% of all neurilemmomas occur in the head and neck region; however, the occurrence in the nasal cavity and paranasal sinus is very rare. 3,4 The most common sites of neurilemmomas in the nasal cavity and paranasal sinuses are the nasal cavity and ethmoid sinus. 5 In our study, 6 cases occurred in the nasal cavity, 2 in the nasal cavity and ethmoid sinus, 1 in the maxillary sinus, and one in the sphenoid sinus. Moreover, the tumor that only occurs in the maxillary sinus and sphenoid sinus is a malignant neurilemmoma. Malignant neurilemmomas account for about 10% of soft-tissue sarcomas, and are unusual in the head and neck region. Malignant neurilemmoma in the nasal cavity and paranasal sinuses is extremely rare. 6,7 The ethmoid and maxillary sinuses most often occur, and the nasal fossa and sphenoid sinus come next. 8
Most cases of neurilemmomas occur between the second and fifth decade of life and have no gender or race predilection. In our study, the male-to-female ratio was 2:3, with an age range from 37 to 77 years and a median age of 49.5 years. Neurilemmomas are generally slow-growing. Therefore, most patients are asymptomatic in their early stage. The late-stage symptoms and signs usually depend on the location and size of the tumor and the involvement of adjacent structures. The clinical symptom is varied and nonspecific. Unilateral nasal obstruction is the most common clinical symptom in our study. Other clinical symptoms included rhinorrhea, headache, exophthalmos, and facial numbness. The differential diagnosis is made with nasal polyps, inverted papilloma, hemangioma, and other nasal cavity and paranasal sinus tumors. A radiological survey of the paranasal sinus is necessary for preoperative diagnosis. Computed tomography scans show a soft tissue mass and clarify the tumor scope. Magnetic resonance imaging can evaluate the extension and its relationship with adjacent structures. These radiological findings are also nonspecific, but these radiological surveys help preoperative diagnosis and surgical planning. The final diagnosis of neurilemmoma was confirmed by histopathological examination and immunohistochemical examination. Moreover, the diagnosis of malignant schwannoma is mainly dependent on histopathological examination because of its atypical clinical symptoms and lack of specific imaging manifestations. Immunohistochemical examination is still needed to assist diagnosis when it is difficult to distinguish between benign and malignant tumor. Typical histology includes spindle cellular Antoni A areas and hypocellular myxoid Antoni B areas. 9 Tumor cells were positive for S-100 protein, and negative for EMA and desmin. This was consistent with the literature that states the spindle cells were positive for S100 protein and vimentin, and negative for EMA and desmin. 10
This tumor is usually encapsulated. The complete surgical excision is the only treatment option for neurilemmomas because of the benign nature of these tumors and their resistance to radiation therapy. 11 The specific surgical approach is determined according to the location and extent of the lesion. With the development of nasal endoscopic surgery, FESS gradually becomes the preferred treatment of neurilemmomas because it can offer superior visualization of the tumor, shorten hospital stay with minimum complications. The chances of recurrences are rare after total removal. However, the local recurrence rate of malignant neurilemmoma is higher. Therefore, patients with malignant neurilemmoma receive postoperative radiotherapy which can reduce local recurrence and prolong overall survival. 12 In our study, 9 patients underwent FESS; however, 1 patient underwent FESS combined with the lateral rhinotomy for complete resection of the tumor. Moreover, 2 patients with malignant neurilemmoma received postoperative radiotherapy. Besides, there were no incidences of tumor recurrence during the study period. Although neurilemmomas in the nasal cavity and paranasal sinuses are rare, otolaryngologists should take this tumor into consideration.
Conclusions
Neurilemmoma or Schwannoma in the nasal cavity and paranasal sinuses is an uncommon tumor, and this tumor is a mainly benign tumor. Although the clinical symptoms and the radiological findings are nonspecific, these are helpful for preoperative diagnosis. Complete surgical excision by FESS is the only treatment option for neurilemmoma in the nasal cavity and paranasal sinuses; while malignant neurilemmoma needs postoperative radiotherapy.
Footnotes
Authors’ Note
Through the analysis of the clinical characteristics of the patients with neurilemmoma or schwannoma of the nasal cavity and paranasal sinuses, we aim to improve the cognition of this disease and guide the treatment of patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.