
Abstract
Objectives
Pharyngocutaneous fistula (PCF) is the one of the major complications after total laryngectomy (TL), which can result in saliva leakage, rupture of major vessels, and increased hospitalization. Several flaps have been tried to prevent PCF during TL, and they are usually associated with donor site morbidity and uncertain viability in case of previously irradiated patients. This study aimed to report a novel bilateral pedicled thyroid gland flap (TGF) technique for delicate and effective reinforcement of neopharynx suture line after TL.
Methods
Bilateral pedicled TGF was performed for the reinforcement of neopharynx T-shape suture sites after TL in this case series.
Results
A total of five cases of the TGF were performed during TL, with four of them being salvage setting following previous chemoradiation therapy (CRT). The well-adapted and viable TGF status was confirmed by post-operative computed tomography scan and normally preserved thyroid hormone levels in all patients. No post-operative infections, hemorrhage, hypothyroidism, hypoparathyroidism, or PCF were reported.
Conclusion
The TGF is an effective and reliable flap in TL patents and should be considered as a method in neopharynx reconstruction, even in salvage TL following prior CRT.
Introduction
Total laryngectomy (TL) is one of the major treatment options for advanced laryngeal and hypopharyngeal cancers. Pharyngocutaneous fistula (PCF) is a common and devastating complication after total laryngectomy (TL), which can result in major vessel rupture, delayed adjuvant therapy, increased duration of hospitalization, higher medical expenses, and poorer quality of life.1-4 PCF usually occurs within two weeks after TL. 5 Although most of the patients with PCF can be managed conservatively, some of them require surgical interventions because of prolonged fistula, infection, and impending rupture of major vessels.6,7 Therefore, it is very important to prevent PCF during TL, and several surgical techniques including free flaps, pectoralis major myocutaneous flap (PMMF) and sternocleidomastoid muscle (SCM) flap. 8 However, free flaps and PMMF could make donors site morbidity and require separate surgical field from TL site.8-10 Otherwise, supraclavicular flap (SCF) and SCM flap could be performed within same surgical field of TL, but viability of flap might be decreased when previous history of irradiation and neck dissection exists.4,11
In this study, we performed thyroid gland flap (TGF) during TL to prevent PCF. TGF is a pedicled flap that is relatively less affected by radiation, and there is no additional skin incision or donor site morbidity because it is within the surgical field of the TL. Here we presented five cases of TGF.
Case Reports
Surgical Technics
Five patients received TL with TGF with following surgical technics. Apron incision was made for subplatysmal flap elevation (Figure 1A) and division of thyroid midline was performed. Bilateral superior and inferior parathyroid was identified and saved with intact blood supply. Blood vessels located at inferior and lateral side of thyroid (inferior thyroidal artery and inferior and middle thyroidal vein) were ligated, and bilateral superior thyroidal artery and vein were preserved. Bilateral superior thyroid artery and vein pedicled thyroid flaps were retracted laterally, and TL was performed (Figure 1B). Pharynx and cervical esophagus were simultaneously resected according to primary tumor extent. Neopharynx was made by pharyngeal T suture with remnant pharyngeal mucosa (Figure 1C) or jejunal free flap (JFF) (in case of circumferential pharyngeal defect). After the formation of neopharynx, pedicled TGF was located at superior transverse neopharynx T suture line (the base of the tongue and pharyngeal mucosa) and inferior vertical suture line (neopharyngeal mucosa suture line) (Figure 1D). Two drains were inserted around thyroid gland flaps, and skin was closed. Surgical technic of thyroid gland flap for reinforcement of pharyngeal T-suture site after total laryngectomy. (A) Subplatysmal flap elevation and identification of larynx and thyroid glands. (B) The formation of bilateral pedicled thyroid gland flaps during total laryngectomy by division of thyroid gland midline with preservation of superior thyroidal artery and vein. (C) Pharyngeal T-suture for the neopharynx. (D) Bilateral pedicled thyroid flaps for the reinforcement of pharyngeal T-suture to prevent pharyngocutaneous fistula.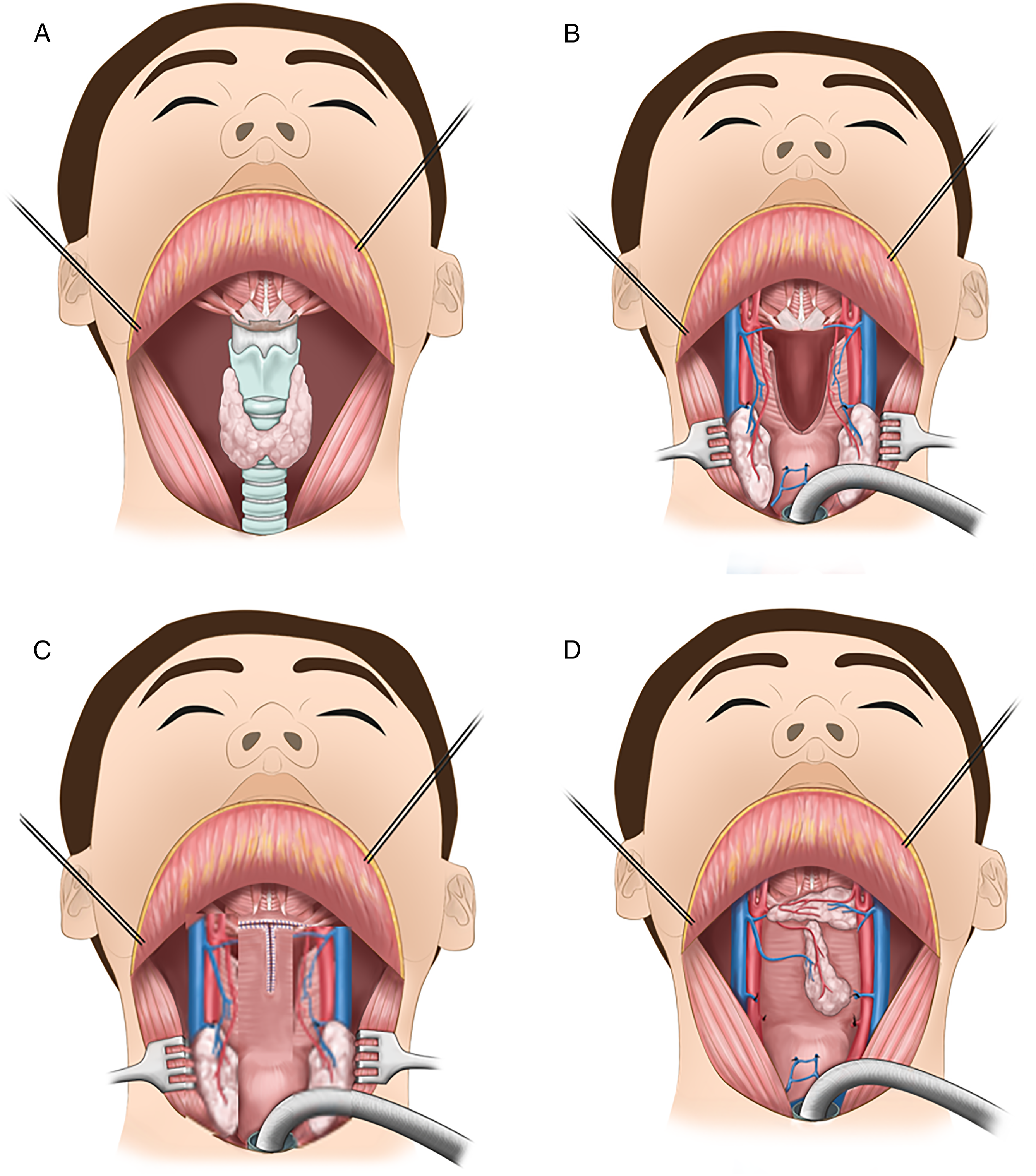
Patients
Case No 1. (63 years old female) had chemoradiation therapy (CRT) for esophageal cancer, and residual cancer was confirmed at 3months after the end of CRT. He had total laryngopharygectomy with cervical esophagectomy and bilateral selective neck dissection. The neopharynx was reconstructed with jejunal free flap and TGF was located at the superior and inferior anastomosis site. Case No 2. (66 years old male) received CRT for supraglottic cancer at 13 years ago, and salvage TL and bilateral modified radical neck dissection were performed due to local and regional recurrence (Figure 2). Neopharynx was made by T-shape closure with remained pharyngeal mucosa, and TGF was located at the superior horizontal suture site and inferior vertical suture site. Case No. 3 (60 years old male) had glottic cancer with compromised airway, and total laryngopharyngectomy and TGF was done. Case No 4. (57 years old male) and case No. 5 (63 years old male) had CRT for glottic cancer about one year ago, and they received total laryngopharygectomy with right neck dissection and TGF for local recurrence. Case No. 2 (66 years old male) who had salvage total laryngectomy for recurred supraglottic cancer after chemoradiation. (A) Pharyngeal defect after salvage total laryngectomy with bilateral neck dissection. (B) Neopharynx formation using pharyngeal T- suture with remnant pharyngeal mucosa. (C) Reinforcement of pharyngeal T-suture site to prevent pharyngocutaneous fistula with bilateral thyroid gland flaps (white asterisks). (D) No contrast leakage in esophagography at 1 week after the surgery. (E) Contrast enhancement of both thyroid gland flaps in CT scan at 3 months after the surgery.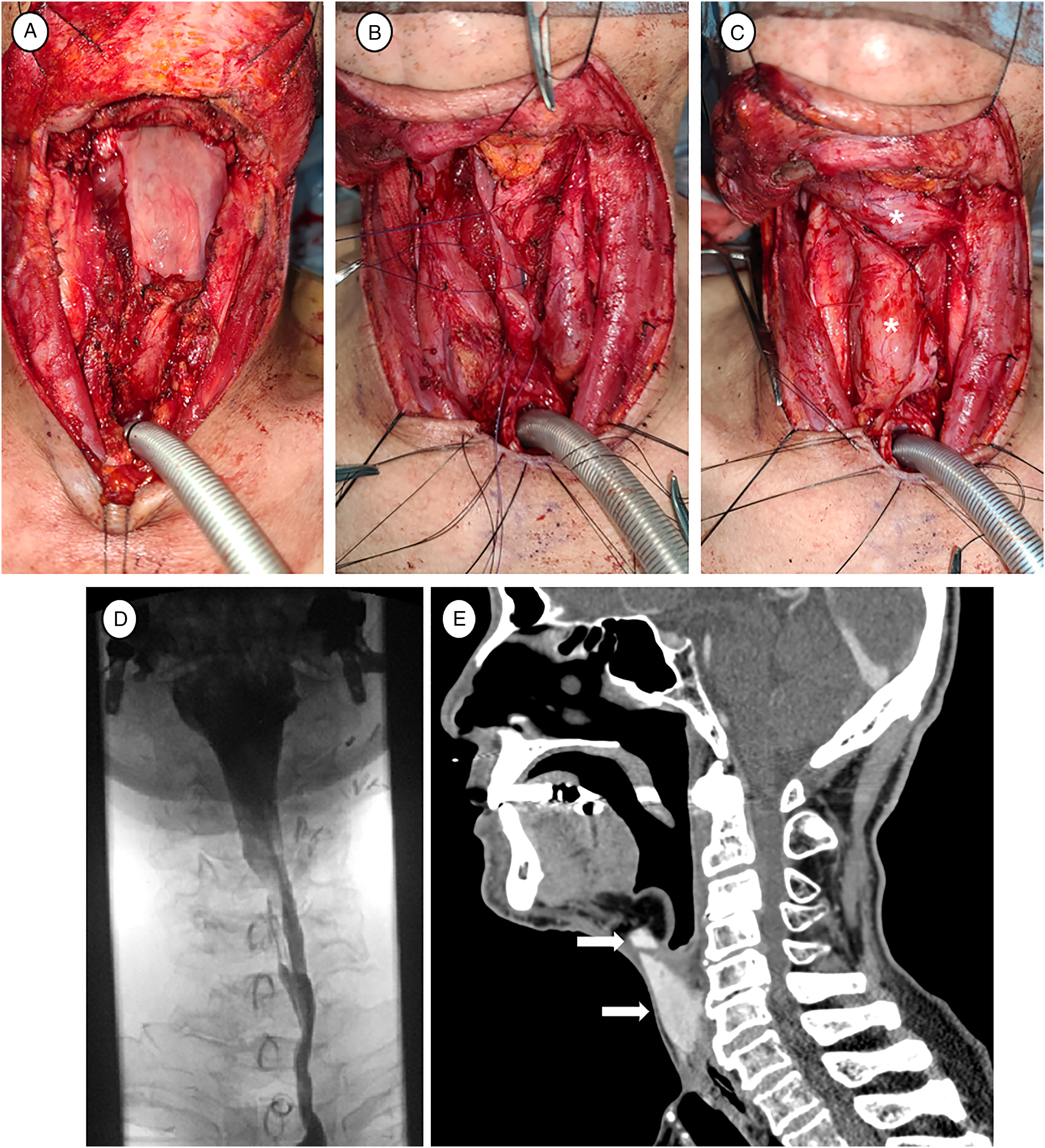
All patients had regular blood lab check-up (complete blood count, ESR, and C-reactive protein) twice a week and esophagography to check the PCF 1week after the surgery. All patients showed no contrast leakage at esophagography, no infection sign, and significant abnormality in blood lab. All patients had oral feeding after the confirmation of no PCF, and there was no sign or symptom of PCF during oral feeding.
Thyroid stimulation hormone level of enrolled patients (Case No. 1–5) was within normal limit or decreased (5.4, 7.2, 0.084, 3.5, and 3.7 μIU/ml, respectively), and free T4 level was also within normal limit (1.31, 1.10, 1.84, 1.21, and 1.04 ng/dl, respectively). Parathyroid hormone was within normal limit in all patients (22.1, 47.9, 29.4, 27.1, and 22.4 pg/ml, respectively). There was no hypofunction of thyroid and parathyroid in all patients.
Discussion
TL is typically used to treat advanced laryngopharyngeal cancer or as a salvage procedure for recurrent or residual disease following radiotherapy (RT) or CRT. Despite the organ preservation treatment with radiation-based treatment allows patients to achieve locoregional tumor control without compromising their natural voice, complication rates are higher than in the initial TL setting.12,13 Complications including bleeding, wound infection, neopharyngeal stricture, tracheostoma stenosis, and PCF were reported up to 67.5%.12,13 Among them, PCF could cause wound infection, longer hospitalization, delayed adjuvant therapy, and major vessel bleeding. The pooled incidence of PCF after TL was 28.9% (range: 5.6–73.3%) in the meta-analysis of Hasan et al. 14
Therefore, several efforts have been tried to prevent PCF, and flap reconstruction has been recognized as the most reliable method. Various flap reconstruction techniques and their efficacy in preventing PCF have been investigated. The non-pedicled local flaps, such as SCM flap, have been employed in some cases,11,15 but they can induce discomfort and impaired neck rotation. In previous study of authors’ institution, we reported that the incidence of PCF after TL was 21.1% (66 out if 313 patients). 16 Among the 66 patients, the 33 patients (50.0%) received flap reconstruction including pedicled and free flap. In addition, in case of simultaneously performed neck dissection with TL, blood supply of the SCM flap could be compromised. Because of their limited flap size and vascularity, the importance of vascularized pedicled flaps is being emphasized, particularly in salvage surgery.8,13,17-19
For the reconstruction after TL, regional flaps including PMMF, SCF, and internal mammary artery perforator flap (IMAPF) were used. In addition, free flaps including radial forearm free flap (RFFF), anterolateral thigh free flap (ALTFF), and JFF were also used. For its high vascularity and accessibility, PMMF is one of the most widely used reconstructive methods in the head and neck area. Its well-vascularized muscle benefits prevention and management even in PCF that one meta-analysis reported that better PCF prevention efficacy in onlay PMMF with PCF rates of 10% compared to 28% without flap. 20 However, its significant chest donor site morbidity, as well as the possibility of overlying skin flap unclosure or tracheostoma displacement due to its bulkiness, should be considered. Some case series, on the other hand, introduced the use of SCF and IMAF in PCF closure because to their limited donor site morbidity, ease of harvest, and relatively pliable nature of those flaps.4,21 In one retrospective study using 10 SCF for pharyngeal reconstruction in TL, three PCF were developed, all of which were salvaged following prior RT. 4 Although its flap size is limited in comparison to PMMF and it could be involved in previous radiation field, it can be used to reconstruct smaller defect sites due to the benefits outlined above.
Free flaps can be easily employed as a patch or a tubed graft depending on the size and shape of the pharynx defect, and they can provide similar outcomes with more versatility and improved cosmetic aspects.8,10 One of its key advantages is that free flap tissue is transferred from a non-irradiated field, which has better vascularity than locoregional flaps especially in salvage TL setting. Among free flaps, RFFF has the advantages of being relatively easy to harvest and having a very flexible nature that matches pharyngeal wall thickness, but it requires an extra skin graft to the donor site. 22 ALTFF, on the other hand, has more vascularity and can be used with wider skin paddles than RFFF, but its bulkiness can make it difficult to manipulate and use as a circumferential reconstruction. 8 One recent multi-center retrospective study, consists of 16 RFFF and 39 ALTFF in salvage TL, showed remarkable outcomes of only three PCF (5.4%) occurrence (two in RFFF and one in ALTFF). 23 JFF is theoretically suitable for neopharynx reconstruction due to its gastrointestinal mucosa, which maintains peristaltic movement, and has also demonstrated its very practical success in circumferential repair as compared with other flaps.10,24 However, its short pedicle, abdominal donor site morbidity and decreased voice outcome due to mucus release from its mucosa should all be taken into account and optimized when choosing patients.8,24 Despite the aforementioned benefits of free flap repair, additional wounds with high donor site morbidity and longer surgery times must be considered when selecting each reconstruction method individually.
In 1990, TGF for laryngeal reconstruction method was first introduced to five cases of vertical partial laryngectomy. 25 They dissected and used a portion of the upper pole based on the defect size, then applied TGF to the defect region. All five flaps remained viable until the last follow-up, and they indicated that TGF is less prone to shrinking than other flaps due to its substantial blood supply. In addition, the pedicle length of the superior thyroidal artery (STA) allows TGF to be easily rotated and used for laryngeal reconstruction.
In our study, we described the five case series of TGF for the reinforcement and reconstruction of pharyngeal T-suture site after TL. Unlike previously reports, we applied the TGF by using whole and both thyroid glands for meticulously reinforcing the neopharynx. We demonstrated that all of our TGF flaps were well adapted to the recipient site, and flap viability was confirmed by enhancement of TGF on post-operative CT and preserved thyroid hormone level. There was also no post-operative hypothyroidism, hypoparathyroidism, bleeding, infection, or PCF despite 80% of our cases previously had CRT.
Based on our experiences, it is important to prevent PCF and TGF is very effective methods by reinforcement of pharyngeal T-suture site after TL. TGF had several advantages in comparison with other flaps. Thyroid gland receives a sufficient blood supply from STA with concomitant vein, allowing TGF to be adequate even in previously irradiated fields.26,27 Furthermore, TGF is easy to harvest and manipulate due to its proximity to pharyngeal defect and sharing the same surgical field with TL. The vascular supply for TGF could be preserved safely even in the patients with bilateral neck dissection. TGF is an ideal flap in TL patients without the need for additional wound in this respect.
To summarize, while there is no clear consensus on which reconstructive approaches provide the best outcomes in PCF prevention for TL patients, TGF should be importantly considered as a novel method in neopharynx reconstruction, even in salvage laryngectomy settings.
Footnotes
Acknowledgment
The authors would like to thank Da Hyeun Lee, an audiovisual engineer at Samsung Medical Information & Medical Services, for designing Figure 1 for this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National research Foundation Korea (NRF) grant funded by the Korea government (MSIT) (No. 2022R1F1A1071634).