
Abstract
Objective:
The aim of this study is to research the correlation between pharyngeal mucosal suture techniques and pharyngocutaneous fistula (PCF) development after total laryngectomy. We also aimed to investigate other risk factor for fistula development.
Methods:
Medical charts of 85 patients who had total laryngectomy during August 2016 and February 2020 were reviewed. Sixteen patients were excluded due to exclusion criteria. Patients were grouped according to pharyngeal mucosal suture technique. Group 1 had modified continuous Connell suture and group 2 had interrupted submucosal suture for mucosal closure of pharynx. Demographic, medical, and surgical records reviewed for comparison.
Results:
Overall PCF rate was 28%;PCF rates were 16% (5/31) in group 1 and 39% (15/38) in group 2. This difference was significant (Pearson χ2 P = .033). There was no difference between groups due to age, gender, smoking history, tumor stage preoperative albumin levels, preoperative hemoglobin levels, radiotherapy status, chronic obstructive pulmonary disorder and diabetes mellitus history of patients, previous tracheostomy, neck dissection. But correlation analysis revealed that PCF formation significantly related with suture technique (P = .032), preoperative albumin level <3.5 g/dL (P = .028), preoperative hemoglobin level <12.5 g/dL (P = .041), and previous radiotherapy status (P = .012) of the patients. We also showed that suture technique is an independent predictive factor for PCF formation when other factors were controlled by univariate analysis.
Conclusion:
The suture technique used for pharyngeal mucosal closure, preoperative albumin level <3.5 g/dL, preoperative hemoglobin levels<12.5 g/dL, and previous radiotherapy to the head and neck are risk factors for PCF development. Modified continuous Connell suture is a good option for pharyngeal closure.
Introduction
The critical functions of the larynx, such as vocalization and swallowing, have shifted the treatment algorithms of laryngeal cancer from radical surgeries to organ preservation protocols. This switch has decreased the number of total laryngectomies as a primary option in laryngeal cancer. However, total laryngectomy (TL) is still the primary option, specifically in laryngeal cancers with extralaryngeal extension; TL is also widely accepted as a salvage treatment option after (chemo)radiotherapy failure to ameliorate the disease. Thus, nowadays, patients having TL are more prone to postoperative complications, because, they have either advanced cancer stage or a (chemo)radiated neck field that makes surgery and postoperative follow-ups more challenging.
Pharyngocutaneous fistula (PCF) is the most common complication after the TL. Pharyngocutaneous fistula rate differs among reports between 2.6% to 65.5%. 1 Fistula formation lengthens hospitalization and increases the transition time to oral feeding. This troublesome complication also has a deleterious effect on both patients’ quality of life and economic prospects, due to longer hospitalization time and potential additional surgeries. Most importantly, PCF delays patients’ potential adjuvant therapy protocols, such as radiotherapy ± chemotherapy after the surgery, which may directly affect the prognosis of the disease.
Head and neck surgeons are specifically interested in this topic. There are numerous reports, meta-analyses, and reviews about the PCF. 2 -8 Predictive factors for PCF formation differ across the researchs. However, prior (chemo)radiotherapy, simultaneously performed neck dissection, preoperative albumin level, preoperative hemoglobin level, and extent of surgery (partial or total laryngopharyngectomy) all seem to be generally accepted risk factors. Closure of the anterior pharyngeal wall during TL is perhaps the most critical intraoperative step of the surgery, as far as PCF is concerned. Although there are numerous articles about the topic, the pharyngoplasty suturing technique during TL has not been appropriately evaluated.
Closure involves 2 components: the closure line and the suturing technique. The closure line means the direction of pharyngeal closure sutures’ line, which can be vertically oriented, horizontally oriented, or T-shaped. 9,10 There is disagreement about the closure line and PCF formation among the studies, 4,11 -13 and one can find differing opinions as to the superiority of one or the other in these articles. This inconsistency may indicate that the closure line may not be the sole important parameter regarding the PCF development. A further problem with these reports is that the researches did not expressly state which suture techniques had been used for mucosal pharyngeal closure.
There are numerous suture techniques available for mucosal pharyngeal closure. 9,11,12,14,15 The technique is quite variable among surgeons, even in the same institution. There are 2 suture techniques used for pharyngeal mucosal closure in our institute. One is an interrupted submucosal suture technique, and the other is a continuous modified Connell suture technique. A very basic but effective modification of the continuous Connell suture has been defined recently. 15 The Connell suture is composed of 2 bites from the ipsilateral mucosal edge; the first bite comes from the outside of mucosa through inside of the mucosa, and after that, second bite goes from mucosal inside to outside classically. The same thing is being repeated on the opposite side. In the modification of the suture, the first bite (from the outside to mucosal inside) should be more distant from the mucosal edge than the second bite (from inside to outside of the mucosa). Ipsilateral mucosal bites should not be on same horizontal line. This maneuver inverts mucosal edges properly (Figure 1). It is described precisely in the article. 15 There are various suture techniques described in the literature, but there are very few studies comparing the suture techniques specifically and these studies are mostly about the difference between stapler suturing techniques and manual suturing. 12,16,17 In our institute, all pharyngeal closures are performed using vertical line closure, due to the head and neck surgeons’ preferences. This surgical preference enabled us to study the suture techniques without any variation about the closure line.
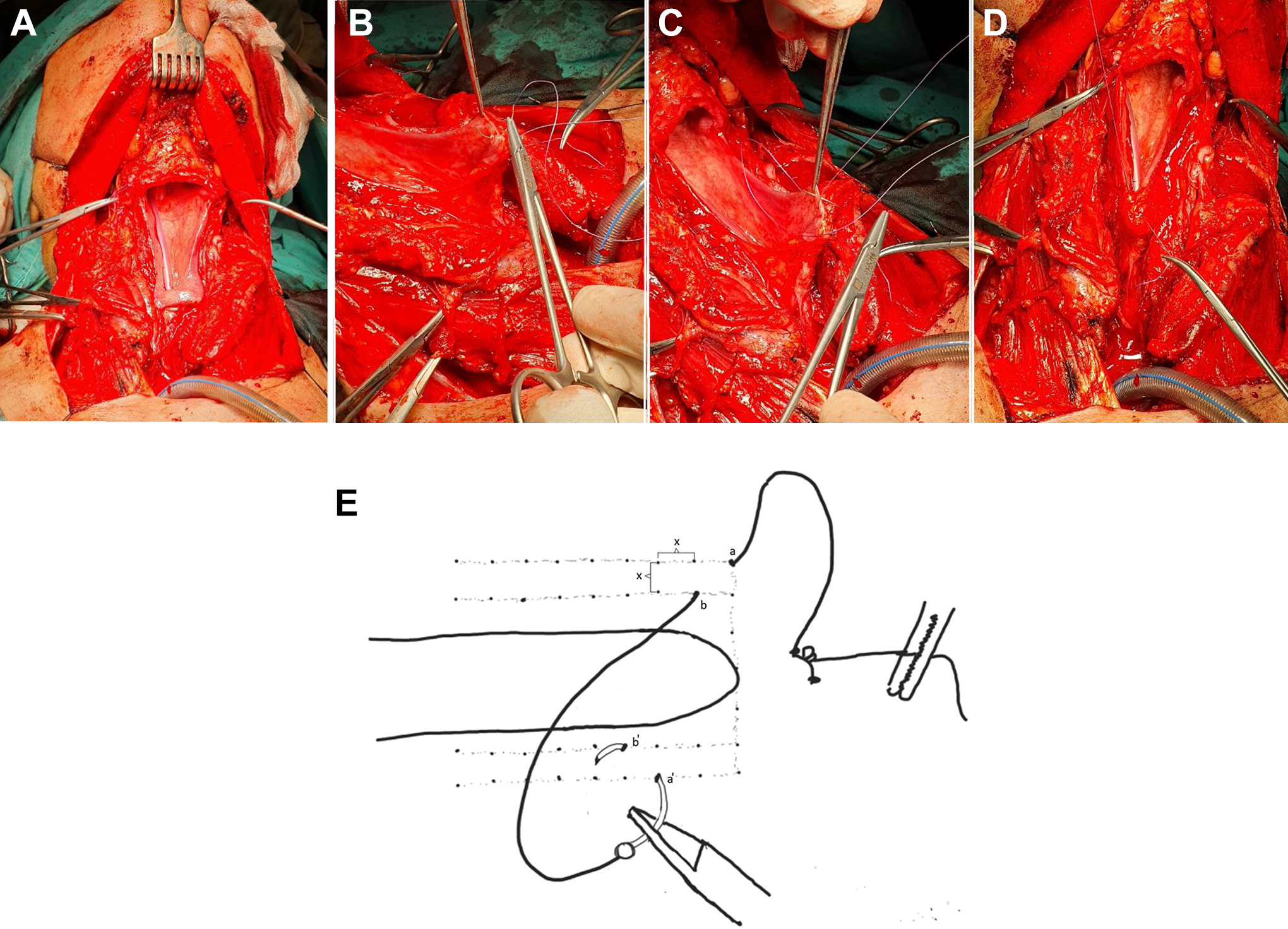
A 65-year-old man had TL. A, photograph shows pharyngeal wall defect after larynx has been removed. B, modified continuous Connell suture is started for pharyngeal mucosal closure. First bite comes from outside to inside of mucosa. C, Second bite comes from inside to outside of the mucosa. Please note that second bite is closer the free edge of pharyngeal mucosa. This maneuver inverts the mucosa properly. D, Appearance of mucosal inversion after the same technique is performed to contralateral side. E, Schematic diagram of modified continuous Connell suture. Note that the distance between the stitch bites are same (showed by X) and none of the stitch bites are on the same line vertically and horizontally. (a) Represents “far outside in bite” from the mucosal edge and it is a bite coming from outside of the mucosa to inside through the mucosa and (b) represents “near inside out bite” from the mucosal edge, it is a bite from the inside of the mucosal edge through the outside. Same is being performed in the other side as a’ and b’. In submucosal sutures as its name indicates, the suture bites does not reach to the mucosa. But in this suturing technique suture comes in and out from the mucosa. In the interlocking sutures, the bites are all on the same vertical and horizontal plane.
In this study, we aimed to compare the effect of the modified continuous Connell suture technique and the interrupted submucosal suture technique for pharyngeal mucosal closure after TL to the PCF formation.
Material and Methods
The medical charts of the consecutive 85 patients who underwent TL ± bilateral neck dissection due to laryngeal cancer, between August 2016 and February 2020, were reviewed for the study. Because of the senior author’s work status, 2 tertiary referral centers’ databases were used for the review. The primary surgeon in the all cases was one of the two authors. Demographic characteristics of the patients such as age, gender, smoking and alcohol habits, tumor stage, and presence of comorbid situations such as chronic obstructive pulmonary disease (COPD), diabetes mellitus (DM), history of (chemo)radiotherapy, and preoperative hemoglobin and albumin levels, previous tracheotomy, neck dissection were collected. The following data were also noted: Preoperative albumin levels (above or below 3.5 g/dL), preoperative hemoglobin levels (above or below 12.5 g/dL), oral intake time after the surgery, and postoperative complications other than the PCF formation. The pharyngeal closure line and pharyngeal mucosal suturing technique were collected from the operation notes. The patients who had partial or total pharyngectomy, in addition to a TL, and the patients who had been performed pedicled or free vascularized free flap usage for mucosal defects were excluded from the study.
Nasogastric feeding was started on the first postoperative day. The tube was generally removed on postoperative day 7 in otherwise normal follow-up patients and postoperative day 11 in patients who had a history of previous radiotherapy. Oral feeding was tried using water colored by methylene blue dye. The PCF fistula was described as the clinical detection of oral feeding contents from fistula; all the fistulas detected in the first thirty days after the TL were considered as a PCF and surgical complication.
Patients were divided into 2 groups, based on the pharyngeal mucosa suturing technique. The first group (group 1) was composed of the patients who had the modified continuous Connell suture technique performed, and the second group was composed (group 2) of the patients who had the interrupted submucosal suture technique performed during pharyngeal mucosal closure.
Surgical Technique
After the larynx had been removed, multiple intraoperative frozen biopsies were studied in all patients, in order to prevent positive tumor margins. The defect on the anterior pharyngeal wall was closed in the vertical direction in all patients due to surgeons’ preference. However, there are 2 different mucosal suturing technique that can be used for pharyngeal mucosal closure in our institute. The first one is a continuous modified Connell suture (group 1; Figure 1), and the other is an interrupted submucosal suture technique (group 2). Inferior constrictor muscles and strap muscles were reapproximated at the median line in all patients after primary mucosal closure of the pharynx.
Statistical Analysis
Analyses were performed with SPSS Statistics version 22.0 (IBM Corp). We used the Pearson χ2 coefficient to evaluate categorical variants between the 2 independent groups (group 1 and group 2), in addition to descriptive statistics. Spearman correlation coefficient was used for nonparametric correlation between variants. The logistic regression model and univariate analysis were performed in order to determine the precise effect of the suture technique on PCF development between the groups.
Results
The medical charts of 85 consecutive patients who were diagnosed with laryngeal cancer between August 2016 and February 2020 were reviewed. Sixteen patients were excluded from the study due to having additional pharyngectomy and/or vascularized flap surgeries; thus, 69 patients were enrolled in the study (64 male and 5 female; mean age 65 ± 4.7 years, range 52-81 years). Patient data are summarized as: 61 patients (88%) had a smoking history (mean smoking value was 34 ± 7.7 package-years), 14 patients (20%) had COPD, 18 patients (26%) had type 2 DM, 15 patients (21%) had hypertension, 17 patients (24%) had prior (chemo)radiotherapy, 7 patients (10%) had T2, 30 patients (43%) had a T3 tumor, and 32 patients (47%) had a T4a tumor, 13 patients (18%) had preoperative albumin levels <3.5 g/dL, 14 patients (20%) had preoperative hemoglobin levels < 12.5 g/dL, 18 patients (26%) had previous tracheotomy, 54 patients (80%) had neck dissection (Table 1). The continuous modified Connell suture technique was performed in 31 (45%) patients (group 1), and the interrupted submucosal suture technique was performed in 38 (55%) patients (group 2) for pharyngeal mucosal closure.
Characteristic Features of the Patients.
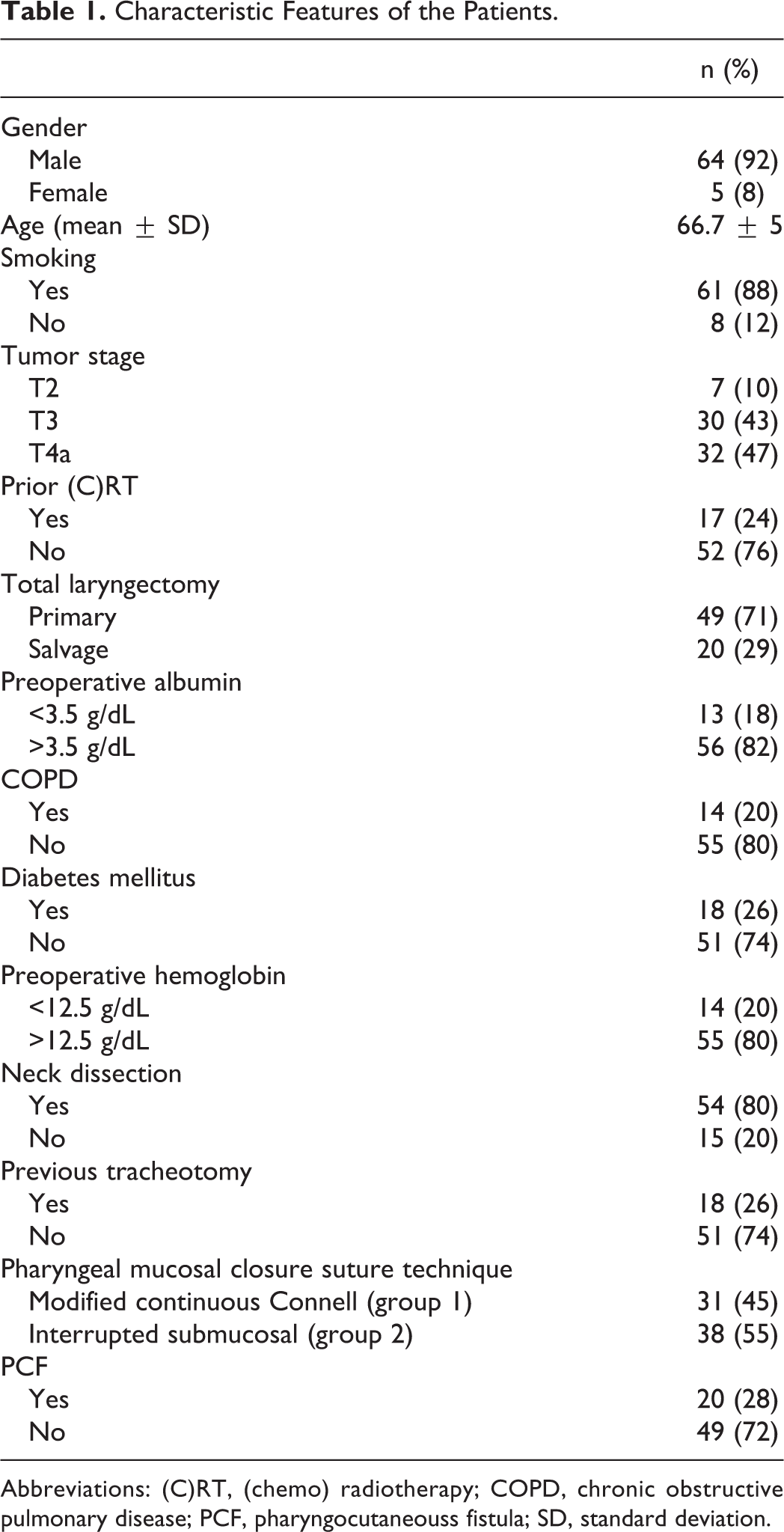
Abbreviations: (C)RT, (chemo) radiotherapy; COPD, chronic obstructive pulmonary disease; PCF, pharyngocutaneouss fistula; SD, standard deviation.
Of the 69 patients, the overall PCF rate was 28% (20/69). Pharyngocutaneous fistula rates were 16% (5/31) in group 1 and 39% (15/38) in group 2. This difference was significant (Pearson χ2 P = .033). There was no difference between groups due to age, gender, smoking history, preoperative albumin levels, preoperative hemoglobin levels, radiotherapy status, COPD, DM history of patients, previous tracheotomy, and neck dissection (P = .48, P = .6, P = .28, P = .45, P = .34, P = .62, P = .71, P = .81, P = .72, P = .82 respectively; Table 2).
Patients Grouped by Pharyngeal Mucosal Closure Technique.a
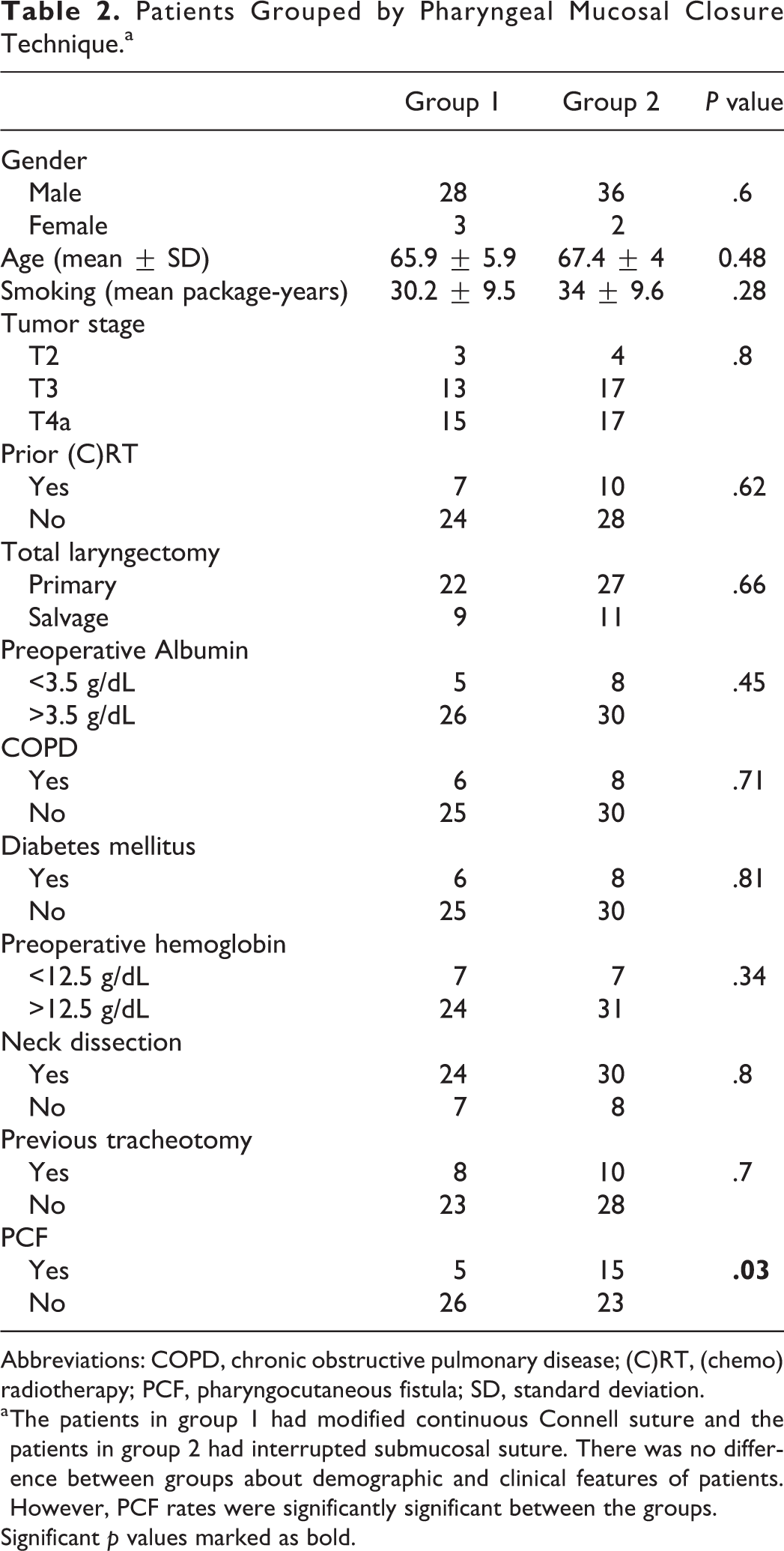
Abbreviations: COPD, chronic obstructive pulmonary disease; (C)RT, (chemo) radiotherapy; PCF, pharyngocutaneous fistula; SD, standard deviation.
a The patients in group 1 had modified continuous Connell suture and the patients in group 2 had interrupted submucosal suture. There was no difference between groups about demographic and clinical features of patients. However, PCF rates were significantly significant between the groups.
Significant p values marked as bold.
In the correlation analysis, there was a significant relationship between fistula formation and suture techniques (P = .032), preoperative albumin levels (P = .028), preoperative hemoglobin levels (P = .041), and radiotherapy status (P = .012; Table 3). There was no correlation between fistula formation and age, gender, smoking history, and any other comorbidities.
There Was Correlation Between PCF Development and Suture Technique, Preoperative Albumin and Hemoglobin Levels, and Previous Radiotherapy Status.
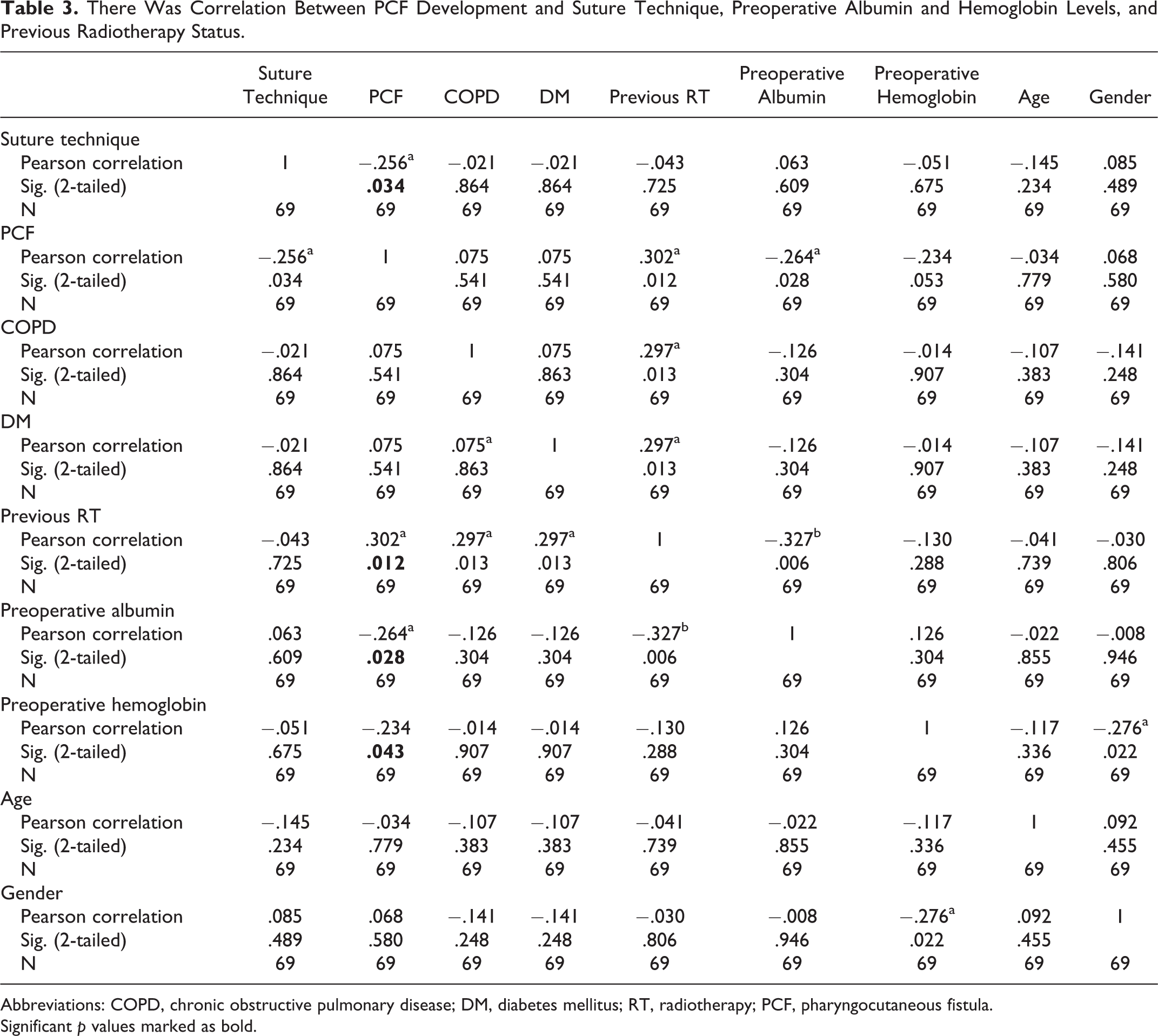
Abbreviations: COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; RT, radiotherapy; PCF, pharyngocutaneous fistula.
Significant p values marked as bold.
Univariate analysis of fistula formation was performed, and suture techniques were considered as an independent factor. This analysis showed that the suturing technique was significantly important when preoperative albumin levels, preoperative hemoglobin levels, and radiotherapy status of patients were controlled as covariates (P = .03).
Discussion
The overall PCF formation rate in the study was 28% (20/69) and a significant difference regarding the incidence of PCF was found between the 2 groups. The other factors studied, age, smoking status, including preoperative albumin and hemoglobin levels, (chemo)radiotherapy status, tumor stage, comorbid situations as COPD and DM, previous tracheotomy and neck dissection were not significantly different among the 2 groups.
It has been shown that the extent of the surgery (additional partial or total pharyngectomy) and vascularized flap usage for mucosal defects has a positive effect on PCF development, 4,6,8,18,19 because after pharyngectomy a vascularized tissue flap is needed for mucosal closure in most cases. This would significantly affect our results, independent of which suture had been used; thus, we have excluded those patients from the study.
The correlation analysis revealed that mucosal pharyngeal suture technique, preoperative albumin and hemoglobin level, radiotherapy status was correlated with PCF development in all patients. There are researches to support these findings. 6,8,19,20 Preoperative albumin and hemoglobin levels may indicate the patient’s nutritional status and preoperative assessment of a patients’ nutritional status may decrease PCF rates. Because oral feeding is not started immediately after surgery, this delay may have a potentially negative effect on wound healing. In order to prevent this problem, we suggest using preoperative albumin and hemoglobin levels as predictive factors to assess the patients’ nutritional status and PCF formation after the surgery. The recent introduction of intensity-modulated radiotherapy and accelerated beam radiotherapy modalities, and very precise dosage measurements may suggest that radiotherapy may not be a risk factor anymore. However, radiotherapy may delay wound healing by obliterative endarteritis, fibrosis hypoxia, impaired leukocyte migration, 21 -23 and radiotherapy to the head and neck area still accepted as a risk factor for PCF. 4,6,8,18 -20 Our study also supported these finding; thus, head and neck surgeons should inform irradiated patients that they have a greater risk for fistula formation.
Deniz et al. concluded that vertical closure with continuous Cushing type suture is superior to horizontal closure with interrupted sutures. 14 This is consistent with our findings. Their study group was composed of 20 patients, while we were able to study the effect of the modified Connell suturing with 69 patients.
In a Dutch study, 4 they conducted a survey among the head and neck surgeons from 8 different head and neck cancer centers, via questionnaire. Twenty-seven of the surgeons (77%) completed and returned the questionnaire; this is important because the questionnaire was about the surgeons’ preference for the pharynx closure technique and oral feeding protocol. Oral feeding time was divided as an early group who had oral intake in the first 3 days and a late group who had their first oral intakes at days 6 to 12. They did not find any differences in PCF development between the early group and the late group. Oral feeding was not included as a variant in our study as we always try to transit oral feeding on postoperative day 7 in nonradiated patients and on postoperative day 11 in radiated patients. We did not use swallow-X rays for the detection of PCF because it is not our daily routine practice. Swallow-X ray studies are time-consuming and require skilled staff and equipment that are not available all the time. Instead, we detected all PCFs clinically—this may be one of the limits of our study.
In same study, 4 they also stated that the information about the pharyngeal closure technique was often missing in the records, and the authors stated that they were disappointed about the missing data. Unfortunately, the closure line and suturing technique of pharyngeal mucosa is not routinely being reported in operating notes of most surgeries in daily practice, making it impossible to evaluate the effect of these variables on PCF formation. We believe that this is one of the important reasons why meta-analyses or review articles about PCF after TL is overlooked, despite this being an important topic. Another vital fact about the pharyngeal closure technique is that it is a surgeon dependent factor, meaning it is modifiable. Most of the other predictive factors about PCF development in the literature have already been highlighted and are mostly patient-related factors that cannot be reversed.
There was a similar research investigation in Australia. 24 A questionnaire about the pharyngeal closure technique was sent to head and neck surgeons, with a return rate of 50%. This report also revealed widespread differences in pharyngeal reconstruction following TL.
Lemaire et al developed a risk score for PCF fistula prediction. 18 They stated that a combination of 4 factors in a patient increases their PCF risk. These 4 factors were active smoking, radiotherapy history to the head and neck field, separate suturing for pharyngeal closure, and pedicled flap usage instead of a free flap when the flap was necessary. In our study, there was no difference between groups due to radiotherapy status, and we excluded the cases where the pedicled or free flaps were used to reconstruct the mucosal defects and we want to study specifically suturing techniques. We believe that the separate or continuous type of the suturing is not only the issue but it is also critical as to which suturing technique was used. Our study demonstrated that the continuous modified Connell suture was superior to the separate submucosal suture. There were other variables affecting the PCF development: preoperative albumin and hemoglobin levels, and radiotherapy status, in which we were able to show a correlation between PCF formations in our study.
There is certain need to assess the various types of continuous suturing techniques in primary pharyngeal closure. This is the only surgery and surgeon related modifiable subject in the TL procedure affecting PCF development. The pharyngeal closure line and suturing technique should be recorded in operation notes in order to further evaluation in future studies. Trying to find better-suturing options may result in decreasing PCF rates. The modified continuous Connell suture is a very good option for primary closure of the anterior pharyngeal wall during TL; it significantly decreases PCF rates. Every head and neck surgeon should be aware of the technique, and it should be applied in appropriate cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.