
Abstract
Purpose:
To evaluate the risk factors of pharyngocutaneous fistula after total pharyngolaryngectomy (TPL) in order to reduce their incidence and propose a perioperative rehabilitation protocol.
Materials and Methods:
This was a multicenter retrospective study based on 456 patients operated for squamous cell carcinoma by total laryngectomy or TPL. Sociodemographic, medical, surgical, carcinologic, and biological risk factors were studied. Reactive C protein was evaluated on post-op day 5. Patients were divided into a learning population and a validation population with patients who underwent surgery between 2006 and 2013 and between 2014 and 2016, respectively. A risk score of occurrence of salivary fistula was developed from the learning population data and then applied on the validation population (temporal validation).
Objective:
To use a preoperative risk score in order to modify practices and reduce the incidence of pharyngocutaneous fistula.
Results:
Four hundred fifty-six patients were included, 328 in the learning population and 128 in the validation population. The combination of active smoking over 20 pack-years, a history of cervical radiotherapy, mucosal closure in separate stitches instead of running sutures, and the placement of a pedicle flap instead of a free flap led to a maximum risk of post-op pharyngocutaneous fistula after TPL. The risk score was discriminant with an area under the receiver operating characteristic curve of 0.66 (95% confidence interval [CI] = 0.59-0.73) and 0.70 (95% CI = 0.60-0.81) for the learning population and the validation population, respectively.
Conclusion:
A preoperative risk score could be used to reduce the rate of pharyngocutaneous fistula after TPL by removing 1 or more of the 4 identified risk factors.
Introduction
Pharyngocutaneous fistula, or pharyngostoma, is a common complication occurring between the 2nd and 23rd post-op day after total laryngectomy (TL) or total pharyngolaryngectomy (TPL). 1 It causes high morbidity, that is, an increase in the length of hospitalization and sometimes requires surgical resumption. The incidence of salivary fistula varies between 3% and 65% depending on the study. 2,3 Three factors have proven significant in several studies and meta-analyses: a history of cervical radiotherapy, post-op anemia, that is, hemoglobinemia of less than 12.5 g/dL, and perioperative malnutrition, as defined by the criteria of the High Authority of Health (HAS) in 2007. 4 -6
Other factors have been found to be significant only in some studies and remain controversial: size and tumor site, unhealthy surgical margins, post-op antibiotic therapy, preoperative tracheostomy, blood transfusion, and comorbidities such as diabetes and associated liver disease. 7,8 Finally, the type of pharyngeal suture has also been implicated. 9
Surgery has been marked in recent years by the emergence of early rehabilitation programs. Initially performed as part of colorectal carcinologic surgery, they have been extended to other surgical specialties. 10 In 2016, the French HAS published an improved recovery program after surgery, the objectives of which are to increase patient satisfaction, reduce the risk of post-op complications, and reduce the length of hospital stay. 11 Several studies have examined the risk factors for salivary fistula, the incidence of which remains high. We studied these risk factors in a cohort of patients and established a risk score for pharyngocutaneous fistula after TL or TPL. The objective was to be able to use this preoperative risk score to modify practices and thus reduce the incidence of salivary fistula.
Material and Methods
This was a retrospective, analytical, multicenter study based on the available data from 3 hospitals. All patients who received TL, TPL, or circular total pharyngolaryngectomy (CTPL) between January 1, 2006, and December 31, 2016 were included. The absence of data on the presence or absence of salivary fistula was the only exclusion factor.
Risk factors were classified as pre-, peri-, or postoperative (Table 1). Preoperative risk factors were those relating to the patient and their cancer. Patient-related factors included age, performance index (World Health Organization [WHO] score), diabetes, liver disease, gastroesophageal reflux disease, smoking over 20 pack-years (PY) active, alcoholism defined by more than 3 glasses of alcohol per day, and undernutrition. Preoperative hemoglobinemia and albuminemia as well as the presence or absence of preoperative re-nutrition were also taken into account. Cancer-related factors included a history of radiotherapy, chemotherapy, or concomitant radiochemotherapy, a history of cervical surgery, size, and tumor stage (as classified by the TNM 7 UICC 2009 classification) and the need for a preoperative tracheotomy.
Characteristics of Risk Factors and Management of Salivary Fistulas.
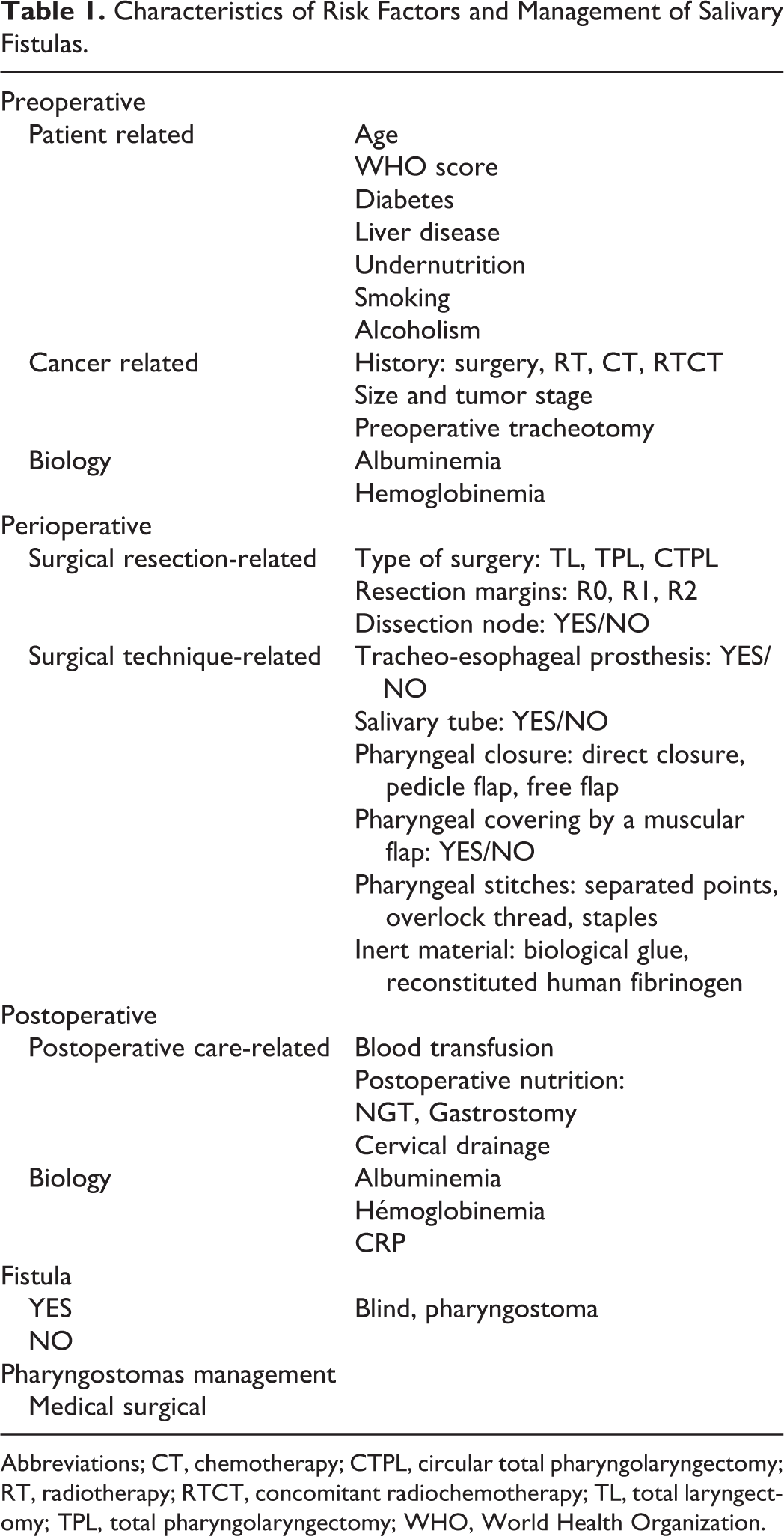
Abbreviations; CT, chemotherapy; CTPL, circular total pharyngolaryngectomy; RT, radiotherapy; RTCT, concomitant radiochemotherapy; TL, total laryngectomy; TPL, total pharyngolaryngectomy; WHO, World Health Organization.
Intraoperative risk factors included type of surgery (TL, TPL, and CTPL), healthy margin resections (R0), microscopic or less than 3 mm (R1), or macroscopically invaded (R2) invasions, the association with a lymph node recess (functional or radical), the placement of a tracheo-esophageal prosthesis and/or a salivary tube, and pharyngeal coverage by a muscle flap. Pharyngeal closure by direct closure, pedicle flap or free flap, and pharyngeal suture by separate stitches, overlock, or staples were noted, as well as the addition of an inert material such as biological glue or recomposed human fibrinogen.
Post-op risk factors included blood cell transfusion, post-op nutrition (nasal feeding tube and gastrostomy), and cervical drainage time (suction drains). Post-op albuminemia and hemoglobinemia as well as reactive C protein (RCP) measured on fifth day (D5) post-op were also noted. Post-op antibiotic therapy was not included as a risk factor because it was systematically prescribed according to the recommendations of the Société Française d’Anesthésie et Réanimation.
Pharyngocutaneous fistulas were grouped into blind fistulas, diagnosed on pharyngeal–esophageal transit (POT) or pharyngeal-cutaneous fistulas, that is, pharyngostomas. Blind fistulas that did not progress to a pharyngostoma were not considered true salivary fistulas. In each case, the treatment performed (compression dressing or surgical resumption) and the time before food resumption were noted.
Data were summarized by frequency and percentage for categorical variables and by median and range for continuous variables. Comparisons between groups were performed using the χ2 or Fisher exact test for categorical variables and the Mann–Whitney U test for continuous variables.
According to the recommendations of Moons et al, the study population was divided into 2 groups according to the year of surgery in order to perform a temporal validation of the risk score. 12 Patients who underwent surgery between 2006 and 2013 and between 2014 and 2016 were included in the learning and the validation population, respectively. A risk score was developed from the learning population data. A penalized logistic regression model with elastic net regularization was used to identify factors associated with the occurrence of a salivary fistula. 13 Using a resampling approach, bootstrap selection stability (BSS) was computed for each factor and only those with a BSS >70% were included in the final model. Risk score was created from the associated regression coefficients and then applied on the validation population. The score performance was quantified in terms of discrimination (area under the receiver operating characteristic [ROC] curve, AUC) and calibration (ie, agreement between observed outcome frequencies and probabilities predicted by the risk score) for the learning and the validation population.
The discriminant capacity of RCP was assessed using the AUC curve. The AUC, sensitivity, specificity, positive, and negative predictive values (NPV) were estimated with their 95% confidence intervals (CIs).
Results
Five hundred seventy-four patients received a TL, TPL, or CTPL between January 1, 2006, and December 31, 2016. One hundred eighteen were excluded due to lack of data. Among the 456 patients included in the study, 328 were operated between 2006 and 2013 (learning population) and 128 between 2014 and 2016 (validation population). Their characteristics are presented in Table 2. The study population was 87% male (n = 397) and 45% of the patients were under 60 years of age. The WHO score was 0 or 1 for most of the population (82%). Of the 456 patients included, 149 had a pharyngocutaneous fistula (33%). In 60% of cases, surgical reoperation was necessary. Average dietary recovery was 11 days versus 45 days for patients without or with salivary fistula, respectively.
Statistical Results of Risk Factors According to Population.
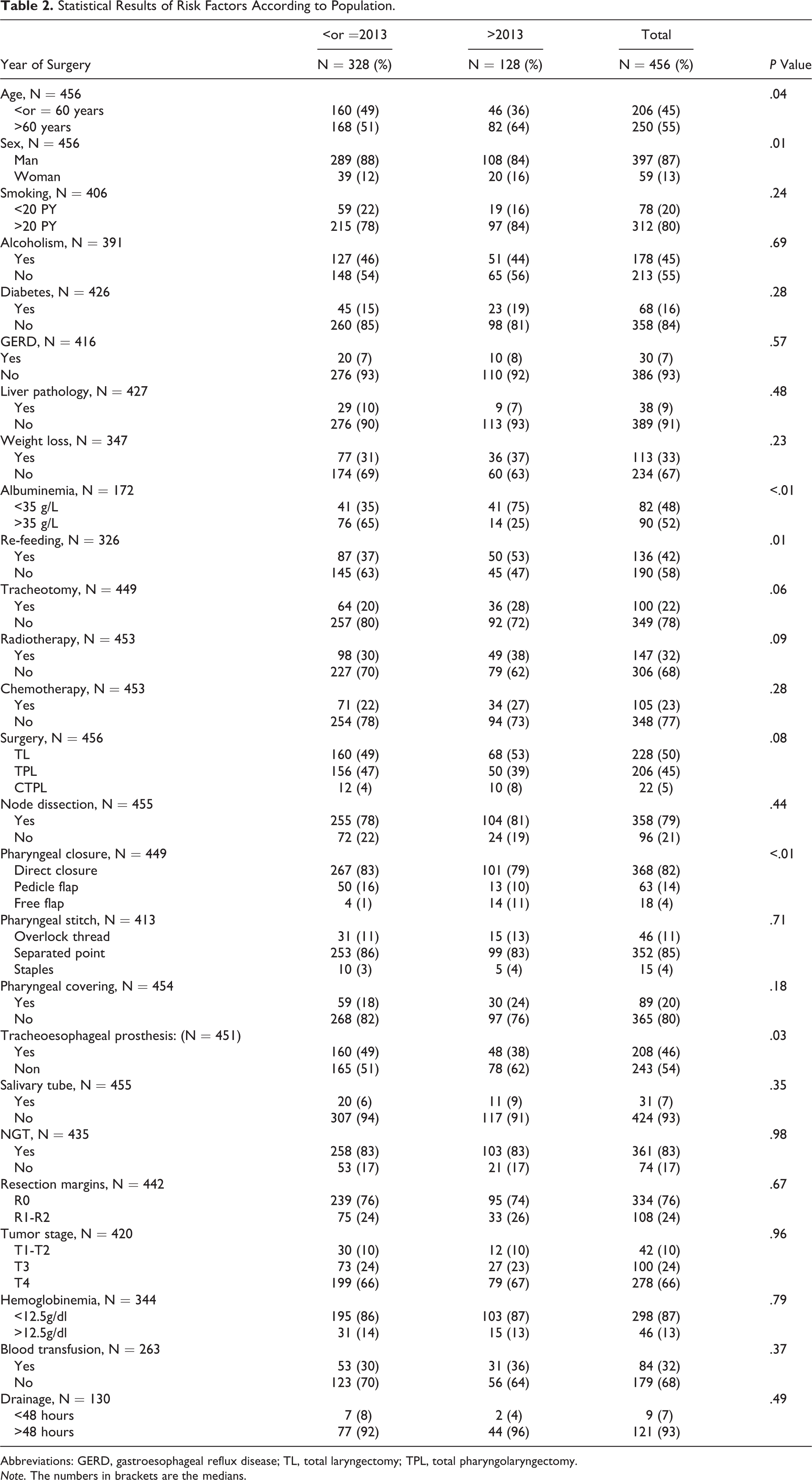
Abbreviations: GERD, gastroesophageal reflux disease; TL, total laryngectomy; TPL, total pharyngolaryngectomy.
Note. The numbers in brackets are the medians.
The score was developed based on the data from the learning population. Figure 1 presents the results of the Elastic Net BSS selection model. Four risk factors associated with the occurrence of the salivary fistula with a BSS >70% were identified. In decreasing order, they were mucosal closure in separate stitches with regard to overlock (BSS = 80.7%), a history of cervical radiotherapy (BSS = 77.4%), smoking >20 PY active (BSS = 73.3%), and closure by a pedicle flap in tile-type musculocutaneous flap of the large pectoral compared to a free flap (BSS = 72.9%).
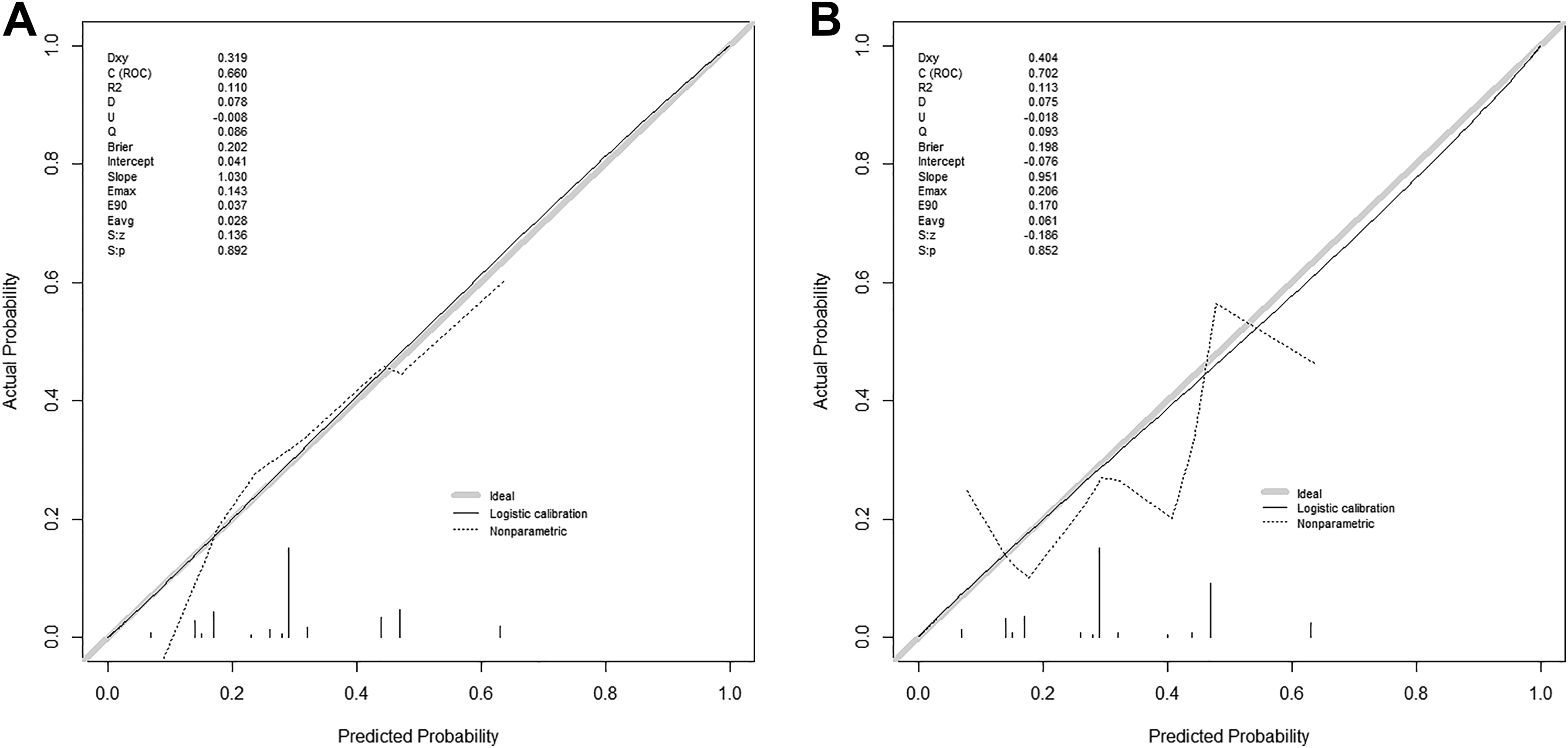
Elastic net/bootstrap selection stability. Calibration: A, learning population; B, Validation population.
The risk score showed good performance in terms of discriminant capacity and calibration on the learning population as well as the validation population. The AUC was 0.66 (95% CI = 0.59-0.73) and 0.70 (95% CI = 0.60-0.81) for the learning and validation population, respectively. Regarding calibration, average (E avg) and maximum (E max) error was 0.03 and 0.14 for the learning population and 0.06 and 0.21 for the validation population, respectively (Figure 1).
The RCP assay (Table 3) at D5 in 139 patients showed an AUC = 0.77 (95% CI = 0.68-0.85). Therefore, an RCP less than or equal to 40 mg/L provided an NPV of 86.96% and a specificity of 23.53%.
Statistical Analysis of RCP at Day 5.
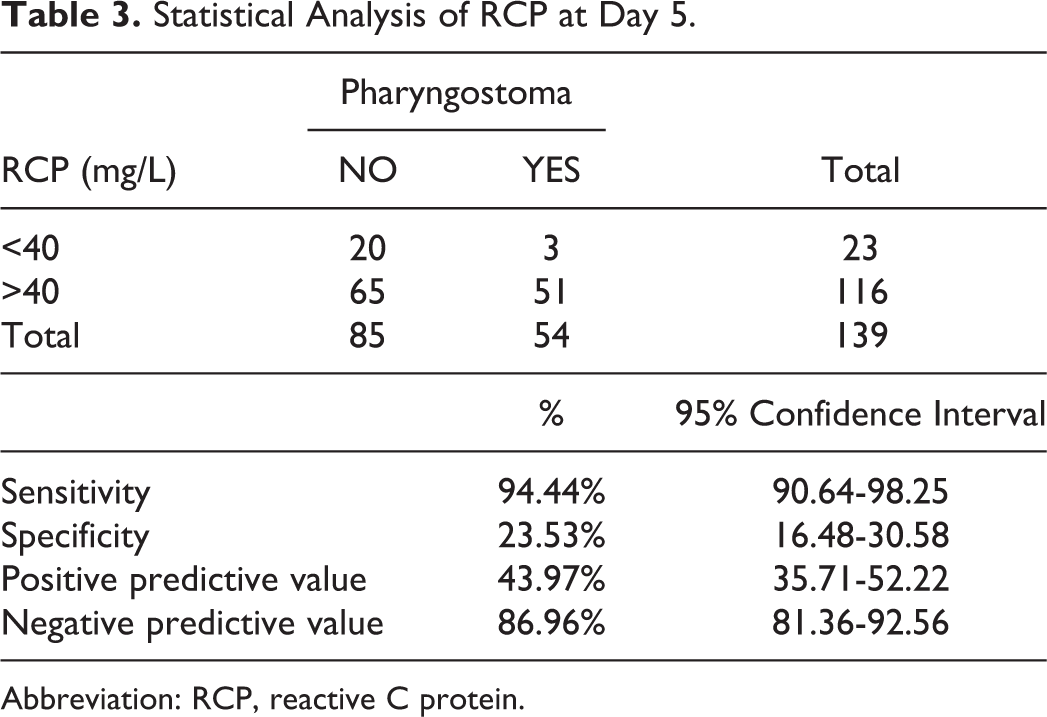
Abbreviation: RCP, reactive C protein.
Discussion
Few risk factors for salivary fistulas have proved significant in recent meta-analyses. Post-op risk factors reported by Paydarfar et al and Liang et al were anemia as defined by hemoglobinemia <12.5 g/dL, preoperative tracheotomy, and cervical radiotherapy in the former study, and unhealthy resection margins, tumor size and location, post-op anemia, and cervical radiotherapy in the latter, respectively. 4 -6 These risk factors remain controversial since they were found to be significant in some studies and nonsignificant in others. We found 4 main high-risk factors for pharyngocutaneous fistula: active smoking >20 PY, cervical radiotherapy, mucosal closure at separate points, and pharyngeal closure by pedicle flap. The risk of developing pharyngocutaneous fistula is maximal when all these factors are combined in the same patient, so the aim is to reduce the number of factors present in order to reduce the relative risk. Smoking is known to cause delayed healing in skin surgery due mainly to hypoxia and tissue ischemia associated with dysimmunity. 14 It may also be responsible for scarring of the pharyngeal mucosa. In 2005, Kuri et al found improved healing in head and neck cancers in patients who had been weaned from smoking 3 weeks before surgery. 15 Cervical radiotherapy is a known and unmodifiable risk factor. Due to laryngeal preservation protocols, this is an increasingly frequent risk factor, that is, salvage laryngectomy. 16 Several authors have studied the risk factors for pharyngocutaneous fistula in irradiated territories. Two recent meta-analyses concerning only salvage laryngectomies confirmed that the addition of healthy tissues such as an interposed regional muscle flap (onlay technique) or a pediculate flap or free flap suture in patch form to the pharyngeal mucosa reduces the rate of pharyngocutaneous fistula by one-third. 17,18
Two intraoperative risk factors were identified, that is, the type of mucosal suture and mucosal closure by pedicle flap. The finding of an increased risk of a mucosal suture with separate stitches compared to an overlock is consistent with 2 other studies. 19,20 They showed a decrease in pharyngocutaneous fistula rate during overlock pharyngeal closure with 1 fistula in 31 patients and 0 fistula in 13 patients, respectively, in patients who received first-line radical surgical treatment, that is, not in an irradiated territory. Mucosal closure by a pedicle flap rather than a free flap also appears to carry a greater risk. Mucosal closure is a valid procedure when the mucosal resection is too large, and the closure requires a flap. Decreasing the number of these 4 identified risk factors would decrease the rate of pharyngocutaneous fistula. Therefore, a mucosal closure by free flap is preferable to a pedicle flap when possible, with preoperative smoking cessation at least 3 weeks before surgery and a mucosal suture by overlock for selected subjects. It should be noted that we performed running sutures only as simple sutures and not for mucosal closure by flaps.
We also analyzed post-op RCP levels. An RCP at D5 less than or equal to 40 mg/L had a NPV of 87% and a specificity of 24%. The analysis of RCP at D5 is useful when deciding on early refeeding. Some authors found no significant difference in the occurrence of pharyngocutaneous fistula between a recharge at D5 or D10 in patients who had had first-line surgery (unirradiated neck). 21 Krouse et al in 1992 established the indication of post-op POT of a TL or TPL to predict the occurrence of pharyngocutaneous fistula. 22 Pharyngeal–esophageal transit has a specificity of 94% according to White et al, and RCP has NPV of 87% in our hands. 23 Combining an RCP assay on D5 with a POT would allow early refeeding and reduce time in hospital.
Conclusion
The combination of smoking >20 PY active, a history of cervical radiotherapy, mucosal closure at separate points with regard to overlock and the placement of a pedicle flap with regard to a free flap represents a maximum risk of post-op saliva fistula after (P)LT.
Reducing the number of these factors could reduce the incidence of salivary fistulas. In the context of early refeeding, an RCP level of RCP <40mg/L at D5 post-op and POT without signs of fistula have a good NPV. Reducing the incidence of salivary fistulas and achieving early refeeding is part of a perioperative rehabilitation program to be evaluated.
Footnotes
Acknowledgments
We thank our colleagues Gaël Espinasse, MD and Jean Carvalho, MD who participated in discussions and managed patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.