
Abstract
Ectopic bronchogenic cyst arising from the parapharyngeal space is extremely rare and has only been reported once in a case report written in Chinese. Here, we reported one case with such a rare congenital abnormality. The patient accidentally found a mass in the parapharyngeal space when taking the head MRI scan. The CT scan showed a 2.6 × 1.9 cm low-density nodule with a well-defined border. The pathological exam confirmed its diagnosis of parapharyngeal bronchogenic cyst.
Introduction
A bronchogenic cyst is a congenital pulmonary anomaly resulting from abnormal budding of the tracheobronchial tree during embryological development. 1 In clinical practice, it is rare to encounter the ectopic bronchogenic cyst that arises outside the lung and mediastinum as the bronchogenic cyst usually arises from the lung or mediastinum (bronchial cyst BC and mediastinal bronchial cyst MBC). 2 Based on previous literature, ectopic bronchogenic cysts were found in the cervical area, abdomen, diaphragm, spinal canal, or even under skin3-8 but not in parapharyngeal space. We then did an extensive search in CNKI (Chinese database) and found only one article reporting such a rare anomaly. 9 Our report is the first English report on a parapharyngeal ectopic bronchogenic cyst which may be of interest to many head and neck surgeons.
Case presentation
A 37-year-old female presented to our department with an accidentally discovered mass in the parapharyngeal space. The patient was asymptomatic and denied any fever, hoarseness, bucking, shortness of breath, dysphagia, shoulder movement disorder, or other symptoms during history taking, we also did not palpate any mass in the cervical region during physical examination.
The previous head MRI from another hospital showed a 2.8 cm oval-shaped mass with an intact capsule in the parapharyngeal space. The mass demonstrated low signal intensities on T1-weighted imaging and high signal intensities on T2-weighted imaging. We performed an electronic nasopharyngoscopy but failed to observe any abnormality in the pharynx. A pre-operative contrast CT scan showed a 2.6 × 1.9 cm low density nodule with a well-defined border (15–40 HU), no enhancement was observed (Figure 1A–C). A. Contrast CT did not show any enhancement; B, C. Coronal and sagittal view showed that the cyst was close to the skull base and was surrounded by blood vessels.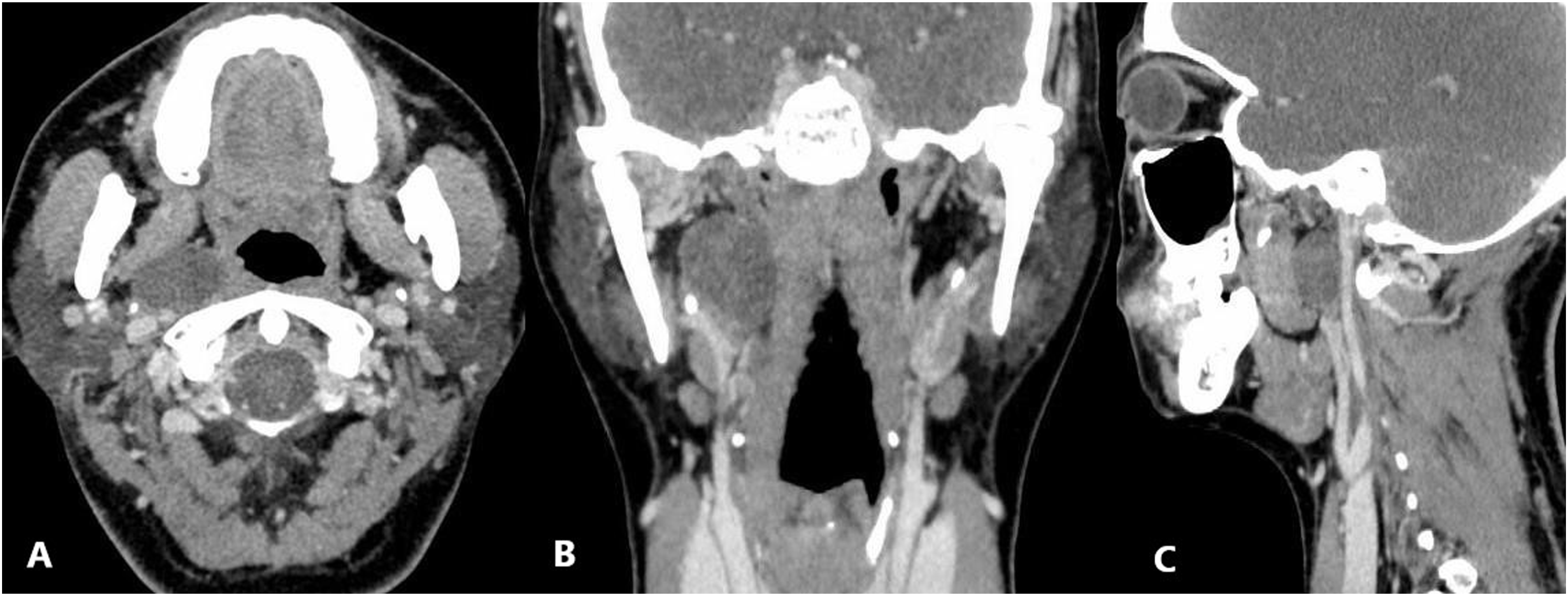
The patient then underwent excisional surgery. We used the submandibular approach to enter the parapharyngeal space, and an oval-shaped mass was discovered in the upper parapharyngeal space. The cystic mass had a thick wall and intact capsule, and the diameter was around 3 cm. We cut the cyst open and found yellowish cloudy fluid. The postoperative pathological examination indicated it was a cystic mass lined by ciliated columnar epithelium in the inner surface, and the pathological diagnosis showed it was an ectopic bronchogenic cyst (Figure 2). Microscopy showed cystic pathological change, lined by ciliated columnar epithelium, suggesting bronchogenic cyst (HE × 100).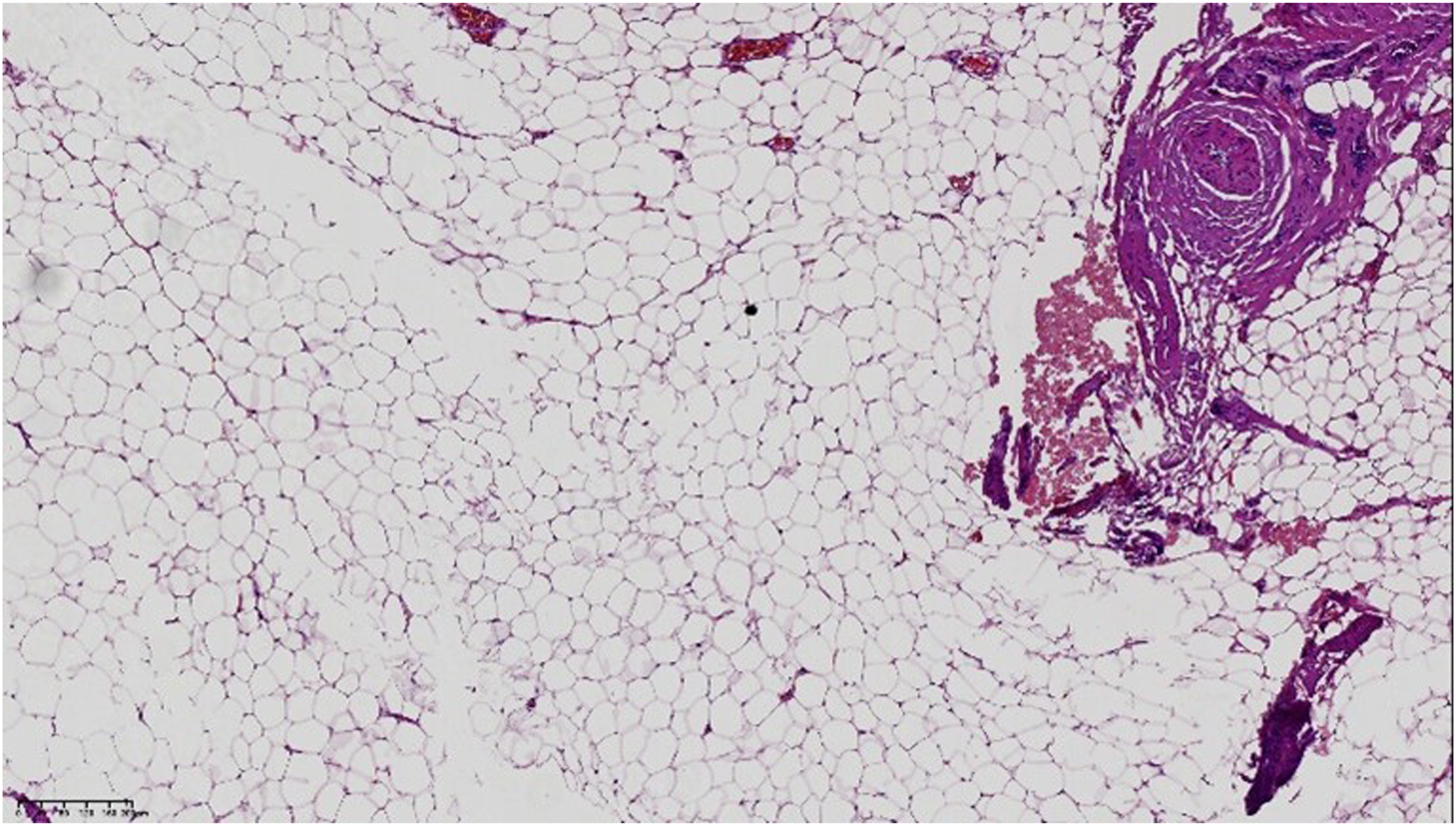
The patient was then discharged without any complications 3 days after the surgery, and no recurrence of the cyst was observed in the 6-months follow up.
Discussion
The parapharyngeal space is divided into pre-styloid and post-styloid compartments separated by fascia from the styloid process to the tensor veli palatini. Anterior compartment contains external carotid artery and external jugular plexus, post-styloid compartment contains the carotid artery/vein, cranial nerve IX–XII, and the sympathetic trunk. The parapharyngeal space is a rare site of tumor origin, while benign tumors account for most of the cases. Salivary gland pleomorphic adenoma is the most common tumor found in parapharyngeal space, followed by the paraganglioma and neurogenic tumors. 3 The treatment of choice for tumors in this anatomical space is surgical excision, surgical approaches include transoral, transparotid, transcervical, submandibular approaches, and so on.
The cyst commonly arises from the lung or mediastinum but can also occur elsewhere as the ectopic bronchogenic cyst. 2 The ectopic bronchogenic cyst can arise from the cervical area, abdomen, diaphragm, spinal canal, or even under skin.3-8 It is extremely rare for it to arise from parapharyngeal space, 9 so our case is valuable for future studies on this disease.
Patients with a tumor in the parapharyngeal space can be asymptomatic in the early stage due to the slow growth of benign tumors. Our patient was completely asymptomatic on admission even though her cyst grew to 2.8 cm in diameter. Du et al. 9 reported a case with a large ectopic bronchogenic cyst in this space, the patient presented to the hospital with a palpable neck mass. The imaging tests showed a 5.1 × 2.8 × 5.2 cm mass protruding into the pharynx. But surprisingly, despite having such a big mass in her neck, she was still asymptomatic. The diagnosis of this disease highly relies on imaging examinations. Normally, the cyst is oval or round in shape with a well-defined cyst border, and the radiodensity (Hounsfield scale) varies on CT scan depending on its content, ranging from 0 to 90 HU. It also will not enhance on contrast CT scan. When the cyst undergoes pathological changes like bleeding or calcification, the Hounsfield scale can go up. Also, the cyst wall can appear to be enhanced on contrast CT when it is inflamed. MRI can be used when the result of CT is inconclusive, and the cyst usually has low signal intensity on T1-weighted imaging and high signal intensity on T2-weighted imaging.
When the image examinations indicate parapharyngeal mass, differential diagnosis like salivary gland pleomorphic adenoma, paraganglioma, schwannoma, first branchial cleft cyst, lymphatic vessel cyst, or ectopic bronchogenic cyst should be considered. Thorough history taking and physical examination should be conducted to check if the patient has symptoms like fever, dysphagia, shortness of breath, and infection. Electronic nasopharyngoscopy should be routinely applied to evaluate the intactness of the pharynx.
The treatment of choice for this disease is surgical excision, we decided to use the submandibular approach in consideration of (1) diameter < 3 cm; (2) location of the cyst which was in the upper parapharyngeal space and close to the skull base where the cyst was surrounded by important blood vessels and nerves; and (3) broader surgical field that submandibular approach can provide thus aiding us in protecting the surrounding structures. The incision of the submandibular approach was located 2 cm below and parallel to the inferior border of the mandible; submandibular gland, digastric, internal carotid artery, internal jugular vein, hypoglossal nerve, vagus nerve, and accessory nerve were exposed. We severed the digastric and dissected all the way up along the carotid sheath until reaching the mass. The mass was peeled out intactly with the capsule. Nerves and blood vessels were gently treated to prevent complications.
In summary, if the parapharyngeal mass locates in the upper parapharyngeal space and has a relatively small size, patients are likely to be asymptomatic in the early stage. When image tests show cystic structure in the parapharyngeal space, ectopic bronchogenic cyst should be considered in the differential diagnosis. Surgical approach is the treatment of choice and should be planned based on the location and the size of the mass. Pathology remains to be the gold standard for diagnosing parapharyngeal mass.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical consideration
Written informed consent for publication of this paper was obtained from West China Hospital and all authors